Keywords
Glutathione; Oxidative Stress
Abbreviations
AOPP advanced oxidation protein products; ERCP
endoscopic retrograde cholangiopancreatography; ROS reactive
oxygen species
INTRODUCTION
Free radical production occurs continuously and under
various conditions, as part of normal cellular biochemical
processes. Excess free radical production, originating from
endogenous or exogenous sources, play an important
role in the pathophysiology of many diseases. The free
radicals superoxide (O2-) and hydroxyl radical (♦OH)
are partial reduction byproducts of the mitochondrial
respiration process, created by the partial reduction of
oxygen, together with hydrogen peroxide (H2O2). These
metabolites, known as ROS (reactive oxygen species),
react with cellular macromolecules and in many cases
start chain reactions of free radicals triggering oxidative
stress. Many radicals behave like oxidants or reductants.
The result is that most of the radicals have short halflives
in the biological systems [1]. Superoxide may be
formed by the oxidation of various molecules, including
adrenalin, nuclear acids and sugar. These processes are stimulated by the presence of transition metals such as
iron and copper. Enzymatic systems may also produce
superoxide, for example cytochrome P450 in the liver, or
enzymatic systems that participate in the synthesis of the
adrenal hormones. Additional sources for the production
of superoxide are phagocytic cells in the respiration
processes and endothelial cells of the blood vessels [1].
Oxidative stress may be caused by external and
environmental factors as well, such as the use of alcohol,
medication, trauma, cold, air pollution, toxins, radiation
and UV light. Today, there is no doubt that pulmonary
infection caused by air pollution is a result of pulmonary
oxidative stress [2]. Hydrogen peroxide is not a free radical;
it belongs to the reactive oxygen species metabolites. It
directly attacks proteins and enzymes that contain thiol
groups.
Living cell had developed protection mechanisms
against toxic oxygen metabolites. They may be divided into
three main groups [1]:
Antioxidant enzymes, catalase is the first antioxidative
enzyme described. It catalyses the decomposition of
hydrogen peroxide to water and oxygen. Additional
enzymes with antioxidative properties are glutathione
peroxidase, glutathione reductase, ceruloplasmin and
superoxide dismutase.
Metal binding proteins, proteins able to bind and carry
transition metals' ions, mostly iron and copper (ferritin, transferrin, lactoferrin, ceruloplasmin). It prevents them
from assisting the production of hydroxyl radicals.
Chain breaking antioxidants, when a free radical binds
to another molecule, additional new radicals may be formed
that may bind to other molecules to from new radicals. This
is a chain reaction. A typical example of such a chain reaction
is the peroxidation of lipids. This process will continue
to propagate until two radicals combine to form a stable
product, or until the radicals are neutralized by a chain
breaking antioxidant. Antioxidants are small molecules able
to accept an electron from a radical or to donate an electron
to a radical with the formation of a stable product.
Antioxidants Form Two Groups
Lipid Phase Chain Breaking Antioxidants: Those
processes occur in the membranes and lipoproteins. The
main antioxidant in this group is Vitamin E that in addition
of being an antioxidant plays a role in the membrane
stabilization. α-Tocopherol is a very important human
antioxidant in the tocopherols group (one of the natural
forms of Vitamin E). An additional group of lipid breaking
antioxidants are the carotenoids, the most important being
β-carotene. Some of them are used as building stones for
Vitamin A (retinal) that also has antioxidant properties,
independent of the oxygen concentration [3]. A large group
of antioxidants from food, fruits, beverages, such as wine
and tee was identified. This group is called flavonoids and
is composed of a great number of polyphenolic compounds
[4, 5, 6]. Epidemiologic studies had found an inverse
relation between the flavonoids intake and the frequency
of chronic diseases of the coronary blood vessels [7, 8, 9].
Aqueous Phase Chain Breaking Antioxidants: These
antioxidants act on radicals present in the aqueous
compartment. Quantitatively, the most important
antioxidant in this group is Vitamin C (ascorbate) that acts
as a cofactor for several enzymes and as an antioxidant
in the aqueous environment. In addition to Vitamin C,
some other antioxidants may be found in plasma in high
concentrations, for example uric acid and the bilirubinalbumin
complex. Thiol groups present on plasma proteins
are very important antioxidants. Sulfhydril groups present
on plasma proteins can act as antioxidants by donating an
electron to neutralize a free radical. Albumin is the main
plasma antioxidant protein. It has 17 disulfide links and one
cysteine residue able to neutralize peroxyl radicals [10].
This property is very important due to the albumin role as
a blood carrier of lipid acids. An additional characteristic
of albumin is its ability to bind copper ions thus inhibiting
peroxidation processes dependent on copper presence.
Albumin is destroyed by its activity as antioxidant but due
to its high plasma concentration and its short half-life this
has no biological importance.
In the reduced state, Glutathione is the main source
of thiol within cells, but of minor importance outside the
cells [11]. It is important to mention that antioxidants that
interrupt the free radicals generation chain reactions in
lipid or aqueous environments act in close coordination, therefore it is impossible to determine which one is
more important. All depends on the conditions and
circumstances present in the immediate environment and
on the oxidation damage caused.
Another important characteristic of antioxidants of the
chain breaking type is their ability to act as pro-oxidants.
Sometimes the presence of antioxidants may enhance
the oxidative damage. For example, it was reported that
Vitamin C may sometimes cause a more severe oxidative
damage if given together with iron [12].
Oxidative stress, caused by the imbalance between
free radicals formation and the antioxidant protective
mechanisms, causes damage to the lipid, protein and
nuclear acids molecules. For example, LDL in the oxidized
state has several characteristics that enable it to catalyze
atherosclerosis processes. It is readily uptaken by
macrophages, exhibits chemotactic properties towards
blood macrophages and smooth muscle cells, catalyzes
monocytes binding to the blood vessels endothelium
and displays a cytotoxic effect on the endothelium cells
[13]. Mitochondria play an important role in the life and
death of the living cell. Evidence suggests that calcium
accumulation in the mitochondria, accompanied by high
oxidative stress, affects its permeability and depletes ATP
reserves leading to the necrotic death of the cell or to the
release of cytocrome C and apoptosis [14]. Antioxidants
interrupt the chain reaction by removing free oxygen
residues/ prevent their generation or by repairing the
damage caused within the cell by free radicals [15].
Block et al. had examined in their work [16] two
lipid peroxidation markers ((MDA) malonaldehyde, F2-
isoprostanes (F2- isoP)) in a healthy population and found:
• A significant increase in the values of the markers
in women and in a subgroup with high values of
C-reactive protein.
• A decrease in the concentration of those markers in a
subgroup with a fruits rich diet.
• High plasma values of ascorbic acid, carotene and
transferrin.
• No age connection was found.
• A direct relationship between MDA level and smoking
and plasma cholesterol concentration.
• A strong positive connection between F2- isoP and
BMW.
Alcohol enables the accumulation of ROS, thus affecting
the body defense mechanisms against these products,
mainly in the liver. Alcohol stimulates cytocrome P450 that
enhances ROS production. In addition, alcohol is likely to
affect the concentration of several metals thus promoting
the production of ROS. Finally, alcohol is likely to lower the
antioxidants levels resulting in oxidative stress and cell
damage. ROS production and oxidative stress in the liver
cells play a central role in the development of alcoholic
liver diseases [17].
γ −tocopherol has several properties absent in
α-tocopherol, the ability to reduce nitrogen dioxide
to an antioxidant state and the ability to suppress the
expression of the gene ras-p21 that is responsible for
coding a protein with oncologic properties. It is possible
that this is the connection between Vitamin E and its
ability to prevent gastrointestinal tumors. Tocotrienols,
the main components of Vitamin E in palm oil may
play a role in the pathogenesis of breast cancer. These
substances accumulate mainly in the fatty tissue that is
the main component of the breast. It was found that oral
administration of those substances to mice stopped breast
cancer spreading. It is possible that in the future Vitamin
E will be used for the treatment of the Alzheimer disease,
preeclampsia and upper respiratory duct infections in
adults [18].
ERCP, since the 70s pioneers in the domain of endoscopy
attempted to investigate the papilla of Vater using optical
fibers endoscopes [19]. Five years later, the first incisions
of the papilla (sphincterotomy) were reported [20].
During the intervention, following the identification of
the papilla of Vater opening, a contrast agent was injected
in order to obtain the image of the bile duct and the
pancreas.
There is an increase in the use of contrast agents
for imaging tests in intrusive interventions. Due to
this increase, nephropathy caused by contrast agents
constitutes the third leading cause for acute in-hospital
renal failure. This disease is accompanied by mortality and
death [21]. Studies show that ROS play an important role
in the pathogenesis of kidney damage caused by contrast
agents and that it might be possible to reduce this damage
by antioxidants such as MESNA [22].
MESNA (sodium-2-mercaptoethane sulphonate) is
a small molecule whose sulfhydryl group (SH) provides
it with the ability of neutralizing ROS particles. MESNA
is administrated intravenously, undergoes spontaneous
oxidation in the blood and is converted to its inactive
form dimesna. This substance is taken up by the tubular
cells of the kidney and is reduced by cell glutathione to
mesna. Masna has a short half-life of 0.36 hours, therefore
it is effective only a short time after its injection [23]. ROS,
formed as a result of the use of contrast agents, can cause
damage to the kidneys in several ways: the ionic contrast
agent is hyperosmotic therefore can damage the tissue and
lead to the accumulation of infected cells, polimorfonuclear
leukocytes, at the injured place and to the release of ROS.
Another possible mechanism is accumulation of ROS at the
place affected by the contrast agent. The iodine attached to
the benzoic acid ring can start the free radical generation
process and the accumulation of ROS that can finally
damage the glomerulus [24].
Pancreatitis is the most frequent complication of
ERCP, and in most of the prospective studies was reported
between 2% to 9%. It may appear as a mild disorder
expressed as abdominal pain and abdominal unpleasant
feeling requiring the extension of the hospitalization by one or two days or a very severe disorder accompanied by
pancreas necrosis and even death [25]. The pathogenesis
of this disorder is not known, technical factors, related to
the procedure itself, may be involved such as: mechanical,
chemical (injection of contrast agents to pancreatic
tracts), hydrostatic (excess of contrast agent), enzymatic,
microbiologic and thermal factors. Factors related to
patients' characteristics may also play a role [26]. Attempts
were made to identify in advance patients at risk of
developing acute pancreatitis following ERCP intervention
by using animal models. Evidence shows that activation of
the gastric enzymes occurs in the acinar cells [27].
Oxidative stress may accompany various diseases and
is expressed by oxidation of complex molecules including
proteins. Protein glycoxidation processes, for example, are
a result of the creation of covalent bonds between residues
of glucose aldehydes and free amine groups on the proteins.
These processes trigger unique changes in the proteins'
properties such as structure and activity, ability to bind to
other molecules, prone to lead to devastating results. The
role played by ROS in the pathogenesis of acute pancreatitis
in animal models is known. Not enough data on changes
occurring in the oxidant- antioxidant systems in humans
has yet been accumulated, in spite of a few works showing
dependency between those changes and the severity of the
disease [28]. Decrease in plasma ascorbate concentration
in patients with acute pancreatitis, mainly patients with
severe disease, and increase in the concentration of protein
carbohydrates indicate the presence of oxidative stress.
No increase in the concentration of lipids peroxidation
products (MDA) was found [29]. Fibrinogen is a plasma
protein, very sensitive to oxidation and defined as acute
phase protein marker. Increase in its concentration
increases the risk of cardiovascular disorders and causes
blood coagulation problems. High concentrations of
fibrinogen were found in patients with acute pancreatitis
and in animal models. Attempts were made to use plasma
concentration dynamics as a prognostic marker of acute
pancreatitis [30]. Changes in the oxidative stress appear
in an early stage of the disease and continue for a longer
period of time than the clinical expression. Understanding
the connection between disease severity and the intensity
of oxidative stress changes may open alternative paths for
the treatment of this disease [31].
The Purpose of the Work
Acute pancreatitis after ERCP intervention is the
most frequent complication and its etiology is not clearly
understood.
The purpose of this work is to investigate if the ERCP
intervention causes a change in the oxidative stress, and
if it does, in which group of patients. Oxidative stress
may increase in all the patients that underwent ERCP,
independently of their basic state of health, since it was
proved that contrast agents have the ability to increase
the oxidative stress in kidney cells. The oxidative stress
may also increase as a result of the clinical state of the
patient prior to the intervention and the complexity of the intervention. Therefore we shall measure the oxidative
stress markers prior and after the ERCP intervention
so that each patient will constitute his own control. An
additional object is to check if the levels of oxidative stress
markers in plasma prior to the intervention may be used
as early predictive markers of the development of acute
pancreatitis as a result of the intervention.
If the results are positive, it will be possible, in phase
two, in additional works, to check if early treatment with
antioxidant drugs may prevent or mitigate the severity of
acute pancreatitis.
Work Performance
In a prospective study, all the patients that underwent
ERCP at the gastroenterology institute were assessed after
receiving their informed consent to the participation in
the medical study in humans as required by the Helsinki
Committee procedure. The 6 months study, carried out
on a population of 40 patients, was approved by the
local Helsinki Committee. The following information was
gathered on the patients: Demographic data, background
diseases, coronary artery diseases, diabetes, general
health condition and severity of disease. According to the
recommendations of the American Anesthetists Society
(ASA classification: anesthesia risk class) patients are
classified as Class I (healthy patient) to Class V (severe
systemic disease with tangible death risk). The instruction
for ERCP intervention was classified according to the
indications of the American Society for Gastrointestinal
Endoscopy (ASGE approved indications for ERCP). In
addition, the intervention process and its technical
difficulty level were documented (ERCP degree of difficulty
grades). The patient height and weight were measured and
the BWI (body mass index) was calculated. The behavioral
parameters alcohol intake and smoking were also
recorded. In addition blood tests that included sugar level,
amylase, cholesterol, liver and kidney functions, CRP level
(Plasma C reactive protein) transferrin saturation were
run. Oxidative stress markers in plasma were measured
before ERCP and after 24 and 48 hours:
• MDA (malondialdehyde) plasma level (lipids
oxidation product)
• AOPP (advanced oxidation protein products) level
• Glutathione plasma level (total, and reduced)
Several inflammation markers were measured before
the ERCP and after 48 hours, in addition to the oxidative
stress markers:
• Fibrinogen level
• CRP level
• Transferase saturation level
MDA Level Measurement
The MDA levels will be measured by a TBARS
(Thiobarbituric acid reactive substances) assay using the
spectrophotometric method [32].
A 250 microliter sample of plasma is diluted 1:1 with
the same volume of PBS. To each sample, 1 ml of TBARS
pH=7, 0.12 M solution is added. The samples are heated
in a water bath at 100°C for 30 minutes and centrifuged
at 800 g for 10 minutes. The absorption intensity of the
supernatant liquid is measured by a spectrophotometer at
a wavelength of 532 nm. The MDA levels are determined
from the calibration curve (0-7.5 nmol MDA).
Fibrinogen levels will be measured in the plasma sample
using a commercial kit based on the immunoturbidimetric
assay, and the Cobas Mira analyzer.
Measurement of Glutathione and Oxidized Glutathione
Levels
The Glutathione level in plasma was measured by the
Adam & Griffith method, modified according to Kristal
et al. [33] using Glutathione reductase. Two separate
measurements were performed:
a. Measurement of total Glutathione (total GSH) that
is equal to the reduced Glutathione and the oxidized
Glutathione (GSSG).
b. Measurement of the oxidized Glutathione level only.
The reduced Glutathione level was calculated as the
difference between the total Glutathione and the oxidized
Glutathione levels. GSH=Total GSH – GSSG
Measurement of AOPP (Advanced Oxidation Protein
Products) Level
Plasma samples were diluted 1:5 with PBS and
acetic acid was added. AOPP were measured by the
spectrophotometric method – the absorption was
measured at a wavelength of 340 nm. AOPP concentration
was calculated using a calibration curve of the solution
[33, 34].
Statistical Analysis
Patients' characteristics were described using suitable
location and dispersion measurements.
Quantitative variables (such as age) were described
using average and standard deviation. Characteristics
presented according to division into groups as well as
qualitative variables (such as gender) were described
using frequency and percents. The correlation between
the patient's disease severity and the demographic
characteristics presented as ordered variables or ration
scale variables, the correlation between the disease
severity, the intervention indication, the intervention
difficulty level, patients' data before the intervention,
and the products (changes in the oxidative stress and the
frequency of the complications, were analyzed using the
Spearman correlation coefficient. Non-parametric tests
such as Wilcox rank sum test or Kruskal Wallis test were
used for the analysis of differences in the changes scale
of the oxidative stress , and in the severity of various
diseases between groups of patients. When products were
combined according to subjects, parametric tests such as
t-test for independent samples were run.
RESULTS
The prospective study was performed for 6 months.
40 patients that underwent ERCP were tested. The
patients signed an informed consent to participate in the
study, according to the Helsinki Committee principles,
and after the approval of the institutional committee, no
patients hospitalized due to acute pancreatitis prior to the
intervention were included in the research.
The average age was 74 years, the standard deviation
was 12.8 years, the age range 39-96 years.
Most of the patients were male (N=24, 60%). In regard
with their general health condition and the severity of
their disease most of them were included in group ASA II
or in group ASA III. No patient was included in group ASA
V (Table 1).

Most of the patients had normal weight (N=17, 42.5%)
or suffered from overweight N=18, 45.0%), and a few
suffered from class I or class II obesity. patients were
included in the weight group according to BMI score.
80% of the patients did not smoke, 2.5% were passive
smokers, 10% smoke less than 30 cigars a day, 7.5% smoke
30 cigars a day or more.
87.5% of the patients did not use to drink alcohol, 7.5%
used to drink less than one drink a week, 2.5% used to
drink between 1 – 2 drinks a day.
The causes for the ERCP intervention were classified
according to the indications of the American Society
for Gastrointestinal Endoscopy (ASGE): 37.5% were
referred due to jaundice suspected of being caused by the
obstruction of the biliary tract. 30.0% due to suspicion
of disease of the pancreas or the biliary tract, 32.5% for
papilla incision or cannulation and stent insertion.
Most of the interventions were defined as therapeutic
(80%) and a few as diagnostic (20%).
The intervention process and its technical difficulty
level were documented (ERCP degree of difficulty grades)
in Table 2.
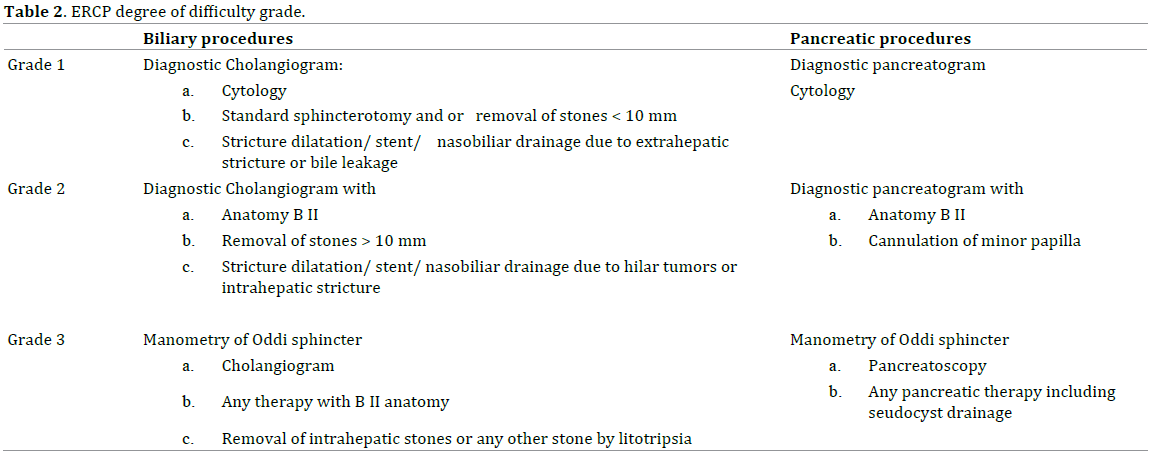
Almost all the activities performed on the bile duct
during ERCP were of the lowest grade, Grade 1, (HN=32,
91.4%). The remaining activities were defined as Grade
2 (N=2, 5.7%) or 3 (N=1, 2.9%). No activities on the bile
duct were performed on five patients. All the activities
performed on the pancreatic ducts on 21 patients were
defined as Grade 1.
The documentation includes, in addition to the
intervention process and its technical difficulty grade, any
unplanned events of the activity. Unplanned events were
divided into two groups: unplanned events one hour after
the intervention and unplanned events that occurred 24
hours after the intervention.
Eight patients suffered from abdominal pain within one
hour from the intervention (N=8, 20%) and one patient
suffered from vomiting after 24 hours, seven patients (17.5%) suffered from abdominal pain, one suffered
had fever, five patients (12.5%) suffered from acute
pancreatitis as a result of the intervention (the diagnosis
was determined based on the clinical findings and the
amylase blood test. For the diagnosis, results two times
higher than the higher limit of the norm. Abdominal CT
was not performed; the inflammation was defined as mild,
Ranson's criteria <3. No bleeding or intestine perforation
events occurred.
The biochemical profile of all the patients was checked
(sugars, blood lipids, blood proteins, liver function) prior
to the intervention. The average values of sugars, blood
lipids and blood proteins were normal.
Amylase, transferrin saturation and oxidative stress
markers values were measured at different time points.
The average values are detailed in Table 3.
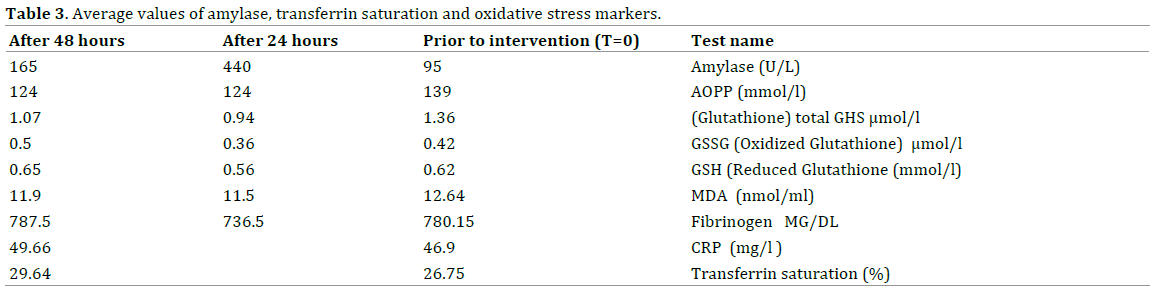
The average value of blood amylase before the
intervention, T=0, was normal. A significant increase in
its value was observed 24 hours after the intervention,
and a significant decrease 48 hours after the intervention,
as compared to its value after 24 hours (Paired T-test, 1
tailed, p=0.002, p=0.0005 respectively) (Figure 1).
Figure 1. Changes in the average value of blood amylase.
The average value of the oxidative stress marker AOPP
prior to intervention was higher than the normal value, a
signi9ficant decrease occurred after 24 hours, but it still
was not normal. There was no change in the average value
of the marker after 48 hours, as compared to its value
after 24 hours (Paired T-test, 1 tailed, p=0.003, p=0.4775
respectively) (Figure 2).
Figure 2. Changes in the average values of AOPP.
The antioxidant enzymatic system, glutathione, was
investigated. A decrease in the average value of total
GHS was observed at 24 hours after the intervention,
then an increase in the average value at 48 hours after
the intervention, compared with the average value
after 24 hours, but these changes were not statistically
significant. Similar changes, also not statistically
significant, were observed in the average values of
reduced glutathione and oxidized glutathione, except for
the increase in the average value of oxidized glutathione
after 48 hours when compared with its average value
after 24 hours, which was significant. (Paired T-test, 1
tailed, p=0.0195) (Figure 3).
Figure 3. Changes in the average value of glutathione.
The changes in the oxidative stress marker MDA were
similar: decrease in the average value (but still above the
normal value) after 24 hours when compared with its
value at time zero (T=0). The decrease was statistically
significant. (Paired T-test, 1 tailed, p=0.034). The increase after 48 hours, to a value lower than that at T=0 was not
statistically significant (Figure 4).
Figure 4. Changes in the average value of MDA.
The average value of Fibrinogen at T=0 was very high,
almost twice more than the higher value of the normal
range, after 24 hours there was a statistically significant
decrease in the average value but it still remained above
the normal range, (Paired T-test, 1 tailed, p=0.0305). After
48 hours another significant increase was observed when
compared with the value after 24 hours (Paired T-test, 1
tailed, p=0.0175) (Figure 5).
Figure 5. Changes in the average value of fibrinogen.
The average value of CRP prior to the intervention, at
T=0, was very high, 9 times more than the normal range.
48 hours after the intervention, its value was still very
elevated and no decrease trend was observed.
A small group of five patients suffered from mild acute
pancreatitis. The average age in this group was 70, most
of them were male (N=4/5, 80%). One patient was graded as Grade I of ASA Class, two patients were Grade II and
two other patients were Grade III. Most of them suffered
from excessive weight, none smoke or consumed alcoholic
drinks. All of them underwent a therapeutic intervention.
The degree of difficulty of the intervention on both the
biliary and pancreatic tracts was Grade I (Figure 6).
Figure 6. Changes in the average values of amylase and AOPP in a group
of patients with acute pancreatitis.
Changes in amylase levels at all times, when compared
with T=0, and the change in the average value after 48
hours, when compared with the value after 24 hours, were
significant (Wilcox Signed Ranks Test, 1 tailed, p=0.031).
The drop in the average value of AOPP, from the value
at T=0 to the value after 24 hours, was significant. The
additional drop after 48 hours, when compared to the
average value after 24 hours, was not significant. The
changes in other parameters were not significant.
The pattern of change in the amylase blood values of the
two groups was studied. One group did not develop acute pancreatitis as a result of the ERCP intervention, the second
one did. At T=0, prior to the beginning of the intervention,
there was no statistically significant difference between
the two groups (Wilcox rank sum test, 2 sided, p=0.774).
The Wilcox Signed Ranks Test was run in order to assess
the differences after 24 and 48 hours: Both groups (that
with and that without acute pancreatitis) showed statistically
significant changes (Table 4 and Figure 6) at both times.

A statistical difference in amylase values was found at
both times, between the group with and the group without
acute pancreatitis.
A statistical difference was found in the amylase values
at the same points in time between the group with and the
group without acute pancreatitis, after the performance of
the ERCP intervention.
At 24 hours after the intervention - Wilcoxon rank sum
test 2 sided, p<<0.001.
At 48 hours after the intervention - Wilcoxon rank sum
test 2 sided, p<<0.001.
As already mentioned, at T=0 there was no statistically
significant difference.
In addition, in the same test, there were statistical
differences in the magnitude of the changes in amylase
levels of the two groups, between any two points in time:
between T=0 and T=24 hours (1 sided, p<<0.001), between
T=24 hours and T=48 hours (1 sided, p<<0.001), between
T=0 and T=48 hours (1 sided, p<<0.005). In the group with
acute pancreatitis, the changes were bigger (Figure 7). No
differences were found between the AOPP and MDA values
in the two groups.
Figure 7. Changes in the amylase values in patients groups with and
without acute pancreatitis.
No difference was found in the fibrinogen concentration
at the different points in time between the two groups,
(with and without acute pancreatitis).
In the group of patients with acute pancreatitis (N=5)
there were no statistical differences in the fibrinogen
concentration at both points in time, on the other hand,
in the group of patients without acute pancreatitis (N=34)
statistical differences were found between T=24 hours and
between T=24 hours and T=48 hours. No difference was
found between T=0 and T=48 hours.
The magnitude of the change in the fibrinogen
concentration between any two points in time was not
different in patients with and without acute pancreatitis.
In the group of patients with acute pancreatitis (N=5)
there was no significant difference in the CRP values
between T=0 and T=48 hours. In the group of patients
without acute pancreatitis no difference was found
between T=0 and T=48 hours, but a difference was found
in the increase of the values at the two points in time, in the group of patients with acute pancreatitis the change was
bigger (Wilcoxon rank sum test 1 sided, p=0.014). there
was no change in the CRP value at T=0 between the two
groups, and at T=48 hours its value in the group with acute
pancreatitis was two times higher (Wilcoxon rank sum test
1 sided, p=0.035).
Since it is known that the sugar levels and the renal
function affect the oxidative stress, the correlation between
the sugar levels and the renal function and the oxidative
stress parameters at T=0 (prior to the intervention) was
investigated: the percentage of diabetic patients and the
percentage of patients with impaired renal function was
similar in the group of patients with normal oxidative
stress values and in the group with high values.
The value of glutathione in the patients that suffered
from acute pancreatitis (N=5) was lower than 2 μmol/l. No
cases of acute pancreatitis were observed. This difference
was not statistically significant, most probably due to
sample size.
No statistically significant correlation was found in the
Nonparametric Correlations test (Spearman`s Correlation
Coefficient test) between the levels of sugar, AOPP, MDA
and glutathione at T=0.
The correlation between the general health status of
the patients, as expressed by their ASA classification, and
the oxidative stress parameters (Wilcoxon rank sum test,
1 sided) was evaluated: the group of patients with higher
oxidative stress levels were not graded higher on the ASA
scale than the group with normal values. Spearman's
correlation test did not show a positive correlation
between ASA grade and the levels of AOPP, MDA and the
blood concentration of glutathione at T=0. The analysis
of the correlation between the various oxidative stress
parameters showed a negative correlation between
glutathione and MDA (Spearman`s Correlation Coefficient
test, Rs=-0.280, 1 sided, p-0.044) and between glutathione
and AOPP (Spearman`s Correlation Coefficient test, Rs=-
0.341,1 sided, p-0.020) and a positive correlation between
the blood concentrations of MDA and AOPP at T=0
(Rs=0.551, 1 sided, p<<0.001). No correlation was found
between gender and oxidative stress parameters (AOPP,
MDA and glutathione level), or between inflammation
parameters (CRP) and fibrinogen. No correlation was
found between age and oxidative stress parameters
(AOPP, MDA and glutathione level) or between BMI values
and these parameters.
Due to the small number of smokers, the correlation
between smoking and oxidative stress parameters was not
evaluated, neither was the correlation between alcohol and
oxidative stress parameters, due to the low consumption
of alcohol reported.
DISCUSSION
The number of studies related to the damage to cells
and tissues caused by oxidative stress had significantly
increased during the last years. The living cells had
developed protection mechanisms against the toxic oxidation metabolites, but these mechanisms do not
ensure complete prevention of the damage. The cells
are constantly under a certain level of oxidative stress,
accompanied by diseases. It must be emphasized that it is
not always clear whether the oxidative stress is the cause
or the result of the disease.
Acute pancreatitis is the most frequent non planned
event that occurs after ERCP interventions. Most of the
prospective studies showed an incidence of 2% to 9% or
more. The severity of the disease ranged from a mild disorder
expressed as abdominal pain and abdominal unpleasant
feeling requiring the extension of the hospitalization by
one or two days, to a very severe disorder accompanied by
pancreas necrosis and even death. The pathogenesis of this
disorder is not known. Independently of the mechanism
that triggers the onset, the disease follows the regular
path of acute pancreatitis. Oxidative stress may play a
role in the pathogenesis of acute pancreatitis [35]. The
role played by surplus ROS in the pathogenesis of acute
pancreatitis in animal models is known. Not enough data
on changes occurring in the balance between oxidant and
antioxidant systems in humans has yet been accumulated.
At present, there is insufficient clinical data to support
the administration of antioxidant drugs, alone or in
combination with conventional therapy, for the treatment
of acute pancreatitis [36].
In addition, it was proved that the contrast agents used
in the ERCP intervention are able to intensify the oxidative
stress. Therefore it was expected to observe an increase in
the oxidative stress as a result of the ERCP intervention. On
the other hand, the probability that candidates to the ERCP
intervention may present high values of oxidative stress
prior to the intervention, as part of their condition, could
not be rejected.
In our study, we found high average values of oxidative
stress markers: AOPP and MDA at time zero, that is prior
to the intervention. Our conclusion is that oxidative stress
accompanied the patients prior to the ERCP intervention.
No increase in the concentrations of the measured oxidative
stress markers occurred as a result of the intervention. On
the contrary, there was a statistically significant decrease
in their values at 24 hours after the intervention, compared
with time zero. This decrease didn't result in normal
values. The conclusion is that high oxidative stress was
present in the candidates to ERCP intervention and that
the intervention itself does not trigger an increase in the
values of the evaluated parameters, but on the contrary – a
decrease in their values.
Most of the ERCP interventions were defined
therapeutic. This may be the reason why the treatment
of the basic problem of the patients caused a significant
decrease in the values of the oxidative stress markers.
If this is true, then why the values did not reach normal
values? And why 48 hours after the intervention the
values were still above normal? Is it possible that this is a
hidden expression of the fact that the intervention triggers
oxidative stress, therefore between 24 to 48 hours after the intervention there was no additional decrease in the
oxidative stress values, but on the contrary the MDA values
after 48 hours were higher than those after 24 hours. It
is possible that the expected changed could have been
identified should we have measured additional oxidative
stress markers. It may be concluded indirectly, from the
decrease in the glutathione values, that the oxidative stress
may have been intensified as a result of the intervention,
thus triggering a response of the protective system in the
form of a decrease in the glutathione values (antioxidative
system).
The average values of the inflammation markers
fibrinogen and CRP were also very high at time zero. 48 hours
after the intervention their values were still very high and
no decrease trend was observed in their values. No positive
correlation was found between the general health condition
of the patients (ASA Classification), gender, age, BMI (body
mass index) values and the oxidative stress markers.
As mentioned above, there was a small group of five
patients that suffered from acute pancreatitis following the
ERCP intervention. No changes in the oxidative stress level
and in the concentration of the inflammation markers were
found in this group at the various time points. Statistically
significant differences were found in the magnitude of
the change in the amylase blood concentration between
the group with and the group without acute pancreatitis.
In the group without acute pancreatitis the changes
were bigger. No difference was found in the fibrinogen
concentration at the different points in time between the
two groups. The magnitude of the change in the fibrinogen
concentration between any two points in time was not
different in patients with and without acute pancreatitis.
The increase in the value of the inflammation marker CRP
was borderline significant from time zero to 48 hours after
the intervention in the group with acute pancreatitis.
The value of glutathione in all the patients that suffered
from acute pancreatitis was lower than 2 μmol/l at time
zero. No cases of acute pancreatitis were observed in
patients with glutathione levels above 2 μmol/l. This
difference was not statistically significant, most probably
due to sample size.
Acute pancreatitis is the most frequent non planned
event that occurs after ERCP interventions. Since the
incidence of this event is not low, and may sometimes reach
10% and more, the large number of studies on this matter
is aimed at a better understanding of its pathogenesis and
at establishing a system that may protect the patients
against it.
Although oxidative stress may play an important role in
the pathogenesis of post ERCP acute pancreatitis, a metaanalysis
that include 11 studies (3010 patients) could not
prove that the administration of antioxidants leads to a
change the incidence and the severity of acute pancreatitis
[37, 38].
In the present work we did not succeed in proving
directly, and based on the parameters evaluated, that the ERCP intervention triggers by itself an increase in
the oxidative stress. We couldn't prove that the oxidative
stress was higher in the group that suffered from post
ERCP acute pancreatitis. We could not define the group
that suffered from acute pancreatitis and could not build a
unique and characteristic model for this group. We found
in literature a work showing that protein carbonyls could
be useful markers of oxidative stress in patients with acute
pancreatitis caused by different factors. These findings
differ from ours. We did not find similar changes in the
AOPP values [29]. That work did not report either higher
MDA values in patients with acute pancreatitis, compared
with the control group.
This result was unexpected, is it possible that the
sensitivity of the test was affected during plasma dilution.
On the other hand the test was sensitive enough when
run on pancreatic tissue and pancreatic liquid in animal
models. Most of the data on changes in the MDA levels
come from works on animal models.
It is also possible that lipids oxidation processes are
transient and quick, therefore if samples are not taken
early enough and close to the event, the early changes in
MDA concentration cannot be identified.
Indeed there are works that show that the peak
concentration of MDA occurs within 4 hours from the
onset of the disease in the animal [29].
It is possible that we did not succeed to show in our work
and increase in the oxidative stress because the MDA level
was measured only 24 hours after the ERP intervention. It
is technically difficult to take plasma samples for the MDA
level tests at such short periods of time therefore the work
must be repeated in order to measure the oxidative stress
markers protein carbonyls, whose half-life is much longer
thus offering the possibility to identify changes in their
levels at different points in time.
Many other studies conducted in the past that aimed
at a better understanding of the pathology of acute
pancreatitis offered several explanations: technical
reasons such as multiple papilla catheterization attempts,
injection of contrast agents, local heat produced during
papilla incision, infection and patients' characteristics.
The ability to develop a predictive tool for the development
of acute post ERCP pancreatitis is very important in the
process of informed consent for better clarifying the patient's
risk to contract this disease and for considering the suitability
of this procedure based on this risk.
Many attempts were made since the development of
the ERCP procedure to identify in advance the patient's
risk of contracting the disease. The present assumption is
that past history of acute post ERCP pancreatitis, sphincter
of Oddi dysfunction, women, normal serum bilirubine
levels are factors related to patient's characteristics.
Fibrinogen is a plasma protein, very sensitive to
oxidation and defined as a marker of the type acute phase
protein. An increase in its concentration accelerates and enhances the risk for cardiovascular diseases and
adversely affects the function of the coagulation system. A
high level of fibrinogen was also found in patients with acute
pancreatitis and in the animal model. Attempts were made to
use the dynamics of plasma concentrations as a prognostic
marker for acute pancreatitis [30]. Changes in the oxidative
stress probably appear in an early stage of the disease and
continue for a longer time than the clinical expression. The
correlation between the severity of the disease and the
intensity of the change in oxidative stress may open new
options for additional therapy for this disease [31].
In our work it was not proved that the oxidative
stress markers measured and the inflammation markers
(including fibrinogen) may be used as early predictive
markers for the development of acute post ERCP
pancreatitis. On the other hand it is possible that the
glutathione level prior to the intervention may constitute
an additional early predictive marker for the development
of acute post ERCP pancreatitis. Patients with levels
above 2 μmol/ l did not develop acute pancreatitis. This
assumption must be further examined in large samples.
CONCLUSION
Most of the patients suffered from high oxidative stress
prior to the ERCP intervention. No direct increase in the
oxidative stress was identified based on the measured
oxidative stress parameters. It may be concluded
indirectly, based on the decrease in the glutathione
levels that the oxidative stress increased as a result of
the intervention. The oxidative stress parameters and
inflammation markers measured are not good predictive
markers for the development of acute pancreatitis. It
is possible that glutathione (oxidative system) may
constitute an early predictive marker. One limitation
of this study is a small number of sample size. Further
studies with larger samples are needed in order to
reinforce this assumption.
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- Young IS, Woodside JV. Antioxidants in health and disease. J Clin
Pathol 2001; 54:176-186. [PMID: 11253127]
- Kelly FJ. Oxidadive Stress: Its role in air pollution and adverse health
effects. Occup Environ Med 2003; 60:612-616. [PMID: 12883027]
- Keys SA, Zimmerman WF. Antioxidant activity of retinal, gluthathione,
and taurine in bovine photoreceptor cell membranes. Exp Eye Res 1999;
68:693-702. [PMID: 10375433]
- Rice-Evans CA, Miller NJ, Paganga G. Structure antioxidant activity
relationships of flavonoids and phenolic acids. Fee Radic Biol Med 1966;
20:933-956. [PMID: 8743980]
- Hertog MGL, Hollman PCH, Katan MB. Content of potentially
anticarcinogenic flavonoids of 28 vegetables and 9 fruits commonly
consumed in Netherlands. J Agric Food Chem 1992; 40:2379-1383.
- Hertog MGL, Hollman PCH, Putte B. Content of potentially
anticarcinogenic flavonoids of tea infusions, wines and fruit juices. J Agric
Food Chem 1993; 41:1242-1246.
- Hertog MGL, Feskens EJM, Hollman PCH. Dietary antioxidant
flavonoids and risk of coronary heart disease: The Zutphen elderly study.
Lancet 1993; 342:1007-1011. [PMID: 8105262]
- Hertog MG, Kromhour D, Aravanis C, Blackburn H, Buzina R, Fidanza
F, et al. Flavonoid intake and long-term risk of coronary-heart-disease
and cancer in the 7 countries study. Arch Inter Med 1995; 155:381-386.
[PMID: 7848021]
- Rmm EB, Katan MB, Ascerio A, Stampfer MJ, Willett WC. Relation
between intake of flavonoids and risk of coronary heart disease in male
health professionals. Ann Inter Med 1996; 125:384-389. [PMID: 8702089]
- Stocker R, Frei B. Endogenous antioxidant defences in human blood
plasma. In: Rice-Evans C. ed. Oxidative stress: oxidants and antioxidants.
London Academic Press 1991: 213-243.
- Sastre J, Pallardo FV, Vina J. Glutathione, oxidative stress and aging.
Age 1996; 19:129-139.
- Suh J, Zhu BZ, Frei B. Anti and pro-oxidant effects of ascorbate on
iron-mediated oxidative damage to bovine serum albumin. Free Radic
Biol Med 1999; 27:305s1.
- Hessler JR, Robetson AL, Chisolm GM. LDL cytotoxicity and its
inhibition by human vascular smooth muscle and endothelial cell culture.
Atherosclerosis 1979; 32:213. [PMID: 223585]
- Duchen MR. Role of mitochondria in health and disease. Diabetes
2004; 53:96s1. [PMID: 14749273]
- Whitaker SH, Pierce JD. Oxygen free radicals and the disease process.
Nurse Practitioner 2003; 28:53-54. [PMID: 12902941]
- Block G, Dietrich M, Norkus EP, Morrow JD, Hudes M, Caan B, et al.
Factors associated with oxidative stress in human populations. Am J
Epidemiol 2002; 156:274-285. [PMID: 12142263]
- Wu D, Cederbaum AI. Alcohol, oxidative stress and free radical
damage. Alcohol Res and Health 2003; 27:277-284. [PMID: 15540798]
- Friedrich MJ. To “E” or not to “E”, vitamin E’s role in health and
disease is the question. JAMA 2004; 292:671-673. [PMID: 15304447]
- Watson WC. Direct vision of the ampulla of Vater with the
gastroduodenal fiberscope. Lancet 1966; 1:902-903. [PMID: 4159621]
- Classen M, Safrany L. Endoscopic papillotomy and removal of
gallstones. Br Med J 1975; 4:371-374. [PMID: 125]
- Goldenberg I, Matetzky S. Nephropathy induced by contrast media:
pathogenesis, risk factors and preventive strategies. CMAJ 2005;
172:1461-1471. [PMID: 15911862]
- Haeussler U, Riedel M, Keller F. Free reactive oxygen species and
nephrotoxicity of contrast agents. Kidney Blood Press Res 2004; 27:167-
171. [PMID: 15256812]
- Mashiach E, Sela S, Weinstein T, Cohen HI, Shasha SM, Kristal B.
Mesna: A novel renoprotective antioxidant in ischemic acute renal failure.
Nephrol Dial Transplant 2001; 16:542-551. [PMID: 11239029]
- Bakris GL, Lass N, Gaber AO, Jones JD, Burnett JC. Radiocontrast
medium-induced declines in renal function: a role for oxygen free
radicals. Am J Physiol 1990; 258:F115-120. [PMID: 2301588]
- Freeman ML, Guda NM. Prevention of post ERCP pancreatitis: A
comprehensive 25 review. Gastrointes Endosc 2004; 59:845-864. [PMID:
15173799]
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman
DJ, et al. Risk factors for post ERCP pancreatitis: A prospective, multicenter
study. Gastrointest Endosc 2001; 54:425-434. [PMID: 11577302]
- Testoni PA. Unresolved issues about post ERCP pancreatitis: an
overview. J Pancreas (online) 2002; 3:156-161. [PMID: 12432181]
- Dziurkowska-Marek A, Marek TA, Nowak A, Kacperek-Hartleb T,
Sierka E, Nowakowska-Duława E. The dynamics of oxidant-antioxida
balance in the early phase of human acute biliary pancreatitis.
Pancreatology 2004; 4:215-222. [PMID: 15148440]
- Winterbourn CC, Bonham MJD, Buss H, Abu-Zidan FM, Windsor JA.
Elevated protein carbonyls as Plasma markers of oxidative stress in acute
pancreatitis. Pancreatology 2003; 3:375-382. [PMID: 14526146]
- Hartleb TK, Nowak A, Hartleb M. Peak plasma fibrinogen as the
predictor of the severity of acute biliary pancreatitis. POL Arch Med
Wewn 1994; 91:257-262.
- Tsai K, Wang SS, Chen TS, Kong CW, Chang FY, Lee SD, et al. Oxidative
stress: an important phenomenon with pathogenetic significance in the
progression of acute pancreatits. Gut 1998; 42:850-855. [PMID: 9691925]
- Morel DW, DiCorleto PE, Chisolm GM. Endothelial and smooth muscle
cells alter low- density lipoprotein in vitro by free radical oxidation.
Arterioscler 1984; 4:357-364. [PMID: 6466193]
- Kristal B, Shurtz-Swirski R, Shapiro G, Chezar J, Manaster J, Shasha
SM, et al. Participation of peripheral polymorphonuclear leukocytes
in the oxidative stress and inflammation in patients with essential
hypertension. Am J Hypertens 1998; 11:921-928. [PMID: 9715783]
- Witko-Sarsat V, Friedlander M, Capeillère-Blandin C, Nguyen-Khoa
T, Nguyen AT, Zingraff J, et al. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int 1996; 1303-13.
[PMID: 8731095]
- Armstrong JA, Cash N, Soares PM, Souza MH, Sutton R, Criddle DN.
Oxidative stress in acute pancreatitis: lost in translation? Free Radic Res
2013; 47:917-933. [PMID: 23952531]
- Esrefoglu M. Experimental and clinical evidence of antioxidant
therapy in acute pancreatitis. World J Gastroenterol 2012; 18:5533-5541.
[PMID: 23112545]
- Wong LL, Tsai HH. Prevention of post-ERCP pancreatitis. World J
Gastrointest Pathophysiol 2014; 5:1-10. [PMID: 24891970]
- Fuentes-Orozco C, Dávalos-Cobián C, García-Correa J, Ambriz-
González G, Macías-Amezcua MD, García-Rentería J, et al. Antioxidant
drugs to prevent post-endoscopic retrograde cholangiopancreatography
pancreatitis: What does evidence suggest? World J Gastroenterol 2015;
21:6745-6753. [PMID: 26074713]








