Keywords
Pancreatic Neoplasms; Positron-Emission Tomography
Abbreviations
SBRT: stereotactic body radiotherapy
INTRODUCTION
For the past decades, computed tomography (CT) has been the gold standard imaging method in pancreatic cancer. It has been used for initial staging, tumor evaluation after treatment, and follow-up of patients with pancreatic cancer. However, this conventional imaging technique is not always efficient in the differentiation between benign and malignant lesions. Positron emission tomography (PET), on the other hand, is a noninvasive molecular imaging technique that uses various radiolabeled compounds and visualizes metabolic differences between tissues, thus depicting the functional status of a suspicious lesion. Data on the use of PET-CT in the staging of patients with pancreatic cancer are scarce.
What We Knew Before the 2014 ASCO Gastrointestinal Cancers Symposium
Pancreatic cancer remains the 5th leading cause of cancer related death with a 5-year survival of under 5% [1]. The best prognosis is in patients who have early disease, are treated surgically, and have negative margins on histopathology. As newer treatment options emerge, we need to determine if imaging techniques hold prognostic information and can actually assess response. As the limitations of Response Evaluation Criteria In Solid Tumors (RECIST) continue to become evident, using 18Ffluorodeoxyglucose positron emission tomography (FDG-PET), which may identify changes in the metabolic activity within pancreatic adenocarcinoma, is under evaluation to determine if it can hold prognostic value.
What We Learned at the 2014 ASCO Gastrointestinal Cancers Symposium
This paper summarizes the abstract presentations of PET scan in patients with pancreatic cancer at the 2014 ASCO Gastrointestinal Cancers Symposium held in San Francisco (Table 1).
Utility of PET/CT as Initial Staging Work-up for Early Pancreatic Cancer (Abstract #183 [2])
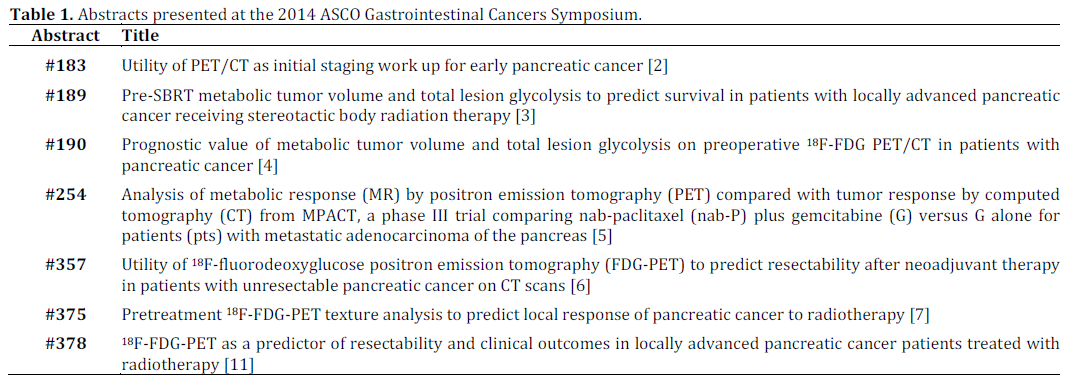
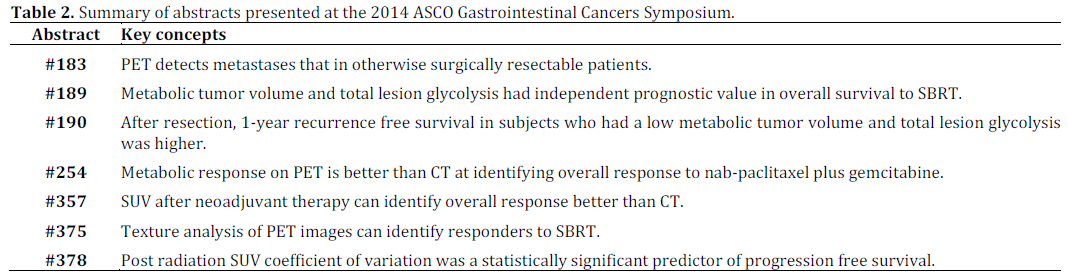
To assess if FDG-PET-CT can identify metastasis that would avoid unnecessary laparotomy in a patient with resectable or borderline resectable cancer, the authors performed a retrospective analysis of the data from 287 patients with early disease. In 11.9% of subjects, the PET-CT changed the stage, with the disease in 33/34 of these subjects being upstaged to stage 4 and 1/34 upstaged to stage 3. As expected, borderline resectable patients had the highest rate of upstaginig.
Pre-SBRT Metabolic Tumor Volume and Total Lesion Glycolysis to Predict Survival in Patients with Locally Advanced Pancreatic Cancer Receiving Stereotactic Body Radiation Therapy (Abstract #189 [3])
As the role of radiation therapy grows, the ability to identify patients who will benefit is important. The authors in this study reviewed data from a prospective study of 32 subjects with locally advanced disease. They had a FDG-PET-CT before and one after fractionated stereotactic body radiotherapy (SBRT). Prior to SBRT, 85% of the subjects received gemcitabine. On the pre-SBRT PET, metabolic tumor volume and total lesion glycolysis had independent prognostic value in overall survival, with metabolic tumor volume of 26.8 cm3 or greater and total lesion glycolysis of 70.9 cm3 or greater. Median survival for the subjects was 18.8 months and therefore, this study may have a bias for less aggressive disease.
Prognostic Value of Metabolic Tumor Volume and Total Lesion Glycolysis on Preoperative 18F-FDG-PETCT in Patients with Pancreatic Cancer (Abstract #190 [4])
This study is a retrospective analysis of 87 subjects who were treated with surgical resection, in which 30 subjects received neoadjuvant therapy. On follow-up, 64% of subjects developed recurrence. The authors found statistically higher 1-year recurrence free survival in subjects who had a low metabolic tumor volume and total lesion glycolysis. In the subjects who did not receive neoadjuvant therapy, which was the majority, metabolic tumor volume and total lesion glycolysis were still statistically significant factors for recurrence.
Analysis of Metabolic Response (MR) by Positron Emission Tomography (PET) Compared with Tumor Response by Computed Tomography (CT) from MPACT, a Phase III Trial Comparing Nab-Paclitaxel (nab-P) plus Gemcitabine (G) versus G alone for Patients with Metastatic Adenocarcinoma of the Pancreas (Abstract #254 [5])
In this study, the authors retrospectively analyzed the PET and CT features of tumors in patients who were prospectively enrolled in the phase III trial (MPACT) that compared nab-paclitaxel plus gemcitabine to gemcitabine alone in patients with previously untreated metastatic disease. Of the 861 subjects, 257 subjects had a baseline FDG-PET; 98% of these scans showed at least 2 FDG avid lesions. Metabolic response, consisting of complete and partial, was statistically higher in the combination drug group (63% vs. 38%). The overall response based on CT, composed of partial and complete response, was 31% for the combo group and 11% for gemcitabine alone. When evaluating subjects without overall response, the median survival of subjects with metabolic response by PET was longer than those without metabolic response.
Utility of 18F-Flourodeoxyglucose Positron Emission Tomography (FDG-PET) to Predict Resectability After Neoadjuvant Therapy in Patients with Unresectable Pancreatic Cancer on CT Scans (Abstract #357 [6])
In this retrospective review, the authors analyzed the data from FDG-PET-CT before and/or after neoadjuvant therapy in subjects with locally advanced or borderline resectable disease. This study used a SUV cutoff of 3.0 or background, defining complete response as a SUV at or below those levels and partial response as a decrease in SUV but above 3.0. In 4 of the 13 subjects, the PET findings met the criteria for overall response (complete response or partial response) despite having unresectable disease on CT. The histopathological evaluation of the resection specimen showed a negative resection margin.
Pretreatment 18F-FDG-PET Texture Analysis to Predict Local Response of Pancreatic Cancer to Radiotherapy (Abstract #375 [7])
In this retrospective review of FDG-PET-CT data, the authors included 10 subjects with locally advanced disease who were treated with SBRT. PET-CT was performed 2 weeks before and 6 weeks after SBRT. Texture analysis, consisting of 6 features [8] (energy [9], correlation, variance, sum mean, cluster tendency [10], inverse variance), was performed and found to be statistically significant in predicting response to SBRT.
18F-FDG-PET as a Predictor of Resectability and Clinical Outcomes in Locally Advanced Pancreatic Cancer Patients Treated with Radiotherapy (Abstract #378 [11])
Subjects with locally advanced disease who underwent radiation therapy were included in this study. Of the 18 subjects, 9 were resectable: 1 subject refused surgery, 6 had negative margins on histopathological analysis of the resection specimen, and 2 developed metastasis and therefore did not undergo surgery. Post radiation PET SUV coefficient of variation [12] was a statistically significant predictor of progression free survival.
Discussion
At the 2014 ASCO Gastrointestinal Cancers Symposium, a total of seven studies related to the prognostic value of FDG-PET were presented. Most of these studies were retrospective and/or included a very small number of patients, making any conclusions difficult. Prithviraj et al. (Abstract #183 [2]) found that PET-CT can be helpful to find metastases in patients who would otherwise be considered resectable. This study forms the basis for a prospective study. Since 18F-fluoroazomycin arabinoside (18F-FAZA)-PET and pimonidazole have shown promise as a marker of hypoxia in pancreatic adenocarcinoma [13], a prospective study comparing it to FDG may be useful.
Medical image diagnosis by radiologists is based on their training, experience and individual judgment to visually identify key image features, which aid them in making decisions. Texture analysis is a wide range of methods incorporating image filtering techniques (wavelets, Gabor, grey level cooccurrence matrix, etc.) that can be used to describe variations in image intensity or patterns. Some of these patterns or differences might be imperceptible to the naked eye but texture analysis with statistical pattern recognition techniques can be used to evaluate texture pattern differences in images. A basic routinely used feature, for example, is size. Texture feature analysis of CT images has shown promise in pancreatic cancer [14]. Similarly, work has been done to identify features on FDGPET images in other tumors, such as esophageal, [15]. Tuli et al. [7] found texture features of the FDG-PET images in a small sample of subjects that correlated with response to SBRT. By using this pilot data and incorporating knowledge gained from work in esophageal cancer, a prospective study would be helpful for further assessment. In addition, some centers routinely use MRI (Figure 1) for staging of pancreatic adenocarcinoma. Feature analysis of MRI images may hold more information [16]. Since gemcitabine interferes with DNA synthesis, MRI techniques like diffusion weighted imaging may be helpful since diffusion weighted imaging is affected by changes in cellular density.
Figure 1. A 76-year male with poorly differentiated ductal
adenocarcinoma in the tail with perineural invasion and
lymphovascular invasion on the resection specimen Total of
4/15 positive lymph nodes were found. Genetic testing was
negative for EGFR, KRAS, and BRAF mutations. MRI before
surgery shows: a. restricted diffusion on diffusion weighted
imaging; b. little to no enhancement two minutes post-contrast
injection. c. Follow-up FDG-PET-CT two months later showed
multiple metastases in the liver with SUV up to 9.8.
Aside from texture analysis, several studies reviewed here demonstrated that measures of metabolic or glycolic activity on FDG-PET may hold prognostic value for subjects with early pancreatic adenocarcinoma. Since radiation therapy disrupts DNA and microvessels, imaging techniques like diffusion weighted imaging and dynamic contrast enhanced MRI may correlate with changes in FDGPET. In a preliminary retrospective study of subjects with hepatocellular carcinoma, Ahn et al. found that SUV on the FDG-PET was inversely related to the dynamic contrast enhanced MRI parameter of perfusion [17]. The PET-MRI systems under development may allow for simultaneous assessment of tumor and identification of prognostic imaging features [18].
Summary
The key concepts of the seven studies presented at the 2014 ASCO Gastrointestinal Cancers Symposium are summarized in Table 2.
Conflict of interest
The authors have no potential conflicts of interest
References
- Siegel R, Ma J, Zou Z, Jamal A. Cancer Statistics 2014. CA Cancer J Clin 2014;64(1):9-29.
- Prithviraj GK, Kothari N, Yue B, Kim J, Springett GM, Malafa MP, Hodul PJ, Kim RD. Utility of PET/CT as initial staging work up for early pancreatic cancer. J Clin Oncol 32, 2014 (suppl 3; abstr 183)
- Dholakia AS, Chaudhry MA, Leal JP, Chang DT, Raman SP, SU Z, Hacker-Prietz A, Pai J, Griffith ME, Wahl RL, Tryggestad E, Pawlik TM, Laheru DA, Wolfgang CL, Koong A, Hermman JM. Pre-SBRT metabolic tumor volume and total lesion glycolysis to predict survival in patients with locally advanced pancreatic cancer receiving stereotactic body radiation therapy. J Clin Oncol 32, 2014 (suppl 3; abstr 189)
- Lee JW, Kang CM, Lee SM, Lee J, Lee JD. Prognostic value of metabolic tumor volume and total lesion glycolysis on preoperative 18F-FDG PET/CT in patients with pancreatic cancer. J Clin Oncol 32, 2014 (suppl 3; abstr 190)
- Ramanathan RK, Von Hoff DD, Moore MJ, Teixeira L, Siena S, Tabernero J, Goldstein D, Wei X, Lu B. Analysis of metabolic response (MR) by positron emission tomography (PET) compared with tumor response by computed tomography (CT) from MPACT, a phase III trial comparing nab-paclitaxel (nab-P) plus gemcitabine (G) versus G alone for patients (pts) with metastatic adenocarcinoma of the pancreas. J Clin Oncol 32, 2014 (suppl 3; abstr 254)
- Khawandanah MO, Kurkjian C, Penaroza S, Arnold C, Herman TS, Talbert M, Postier R, Pant S. Utility of 18F-flourodeoxyglucose positron emission tomography (FDG-PET) to predict resectability after neoadjuvant therapy in patients with unresectable pancreatic cancer on CT scans. J Clin Oncol 32, 2014 (suppl 3; abstr 357)
- Tuli R, Fraass B, Yang W, Sandler HM, Hendifar A, Nissen NN, Yue Y, Oschin S. Pretreatment 18F-FDG-PET texture analysis to predict local response of pancreatic cancer to radiotherapy. J Clin Oncol 32, 2014 (suppl 3; abstr 375).
- Galavis PE, Hollensen C, Jallow N, Paliwal B, Jeraj R. Variability of textural features in FDG PET images due to different acquisition modes and reconstruction parameters. Acta Oncol. 2010 Oct;49(7):1012-6.
- Dong X, Xing L, Wu P, Fu Z, Wan H, Li D, Yin Y, Sun X, Yu J. Three-dimensional positron emission tomography image texture analysis of esophageal squamous cell carcinoma: relationship between tumor 18F-fluorodeoxyglucose uptake heterogeneity, maximum standardized uptake value, and tumor stage. Nucl Med Commun. 2013 Jan;34(1):40-6.
- Bagci U, Yao J, Miller-Jaster K, Chen X, Mollura DJ. Predicting future morphological changes of lesions from radiotracer uptake in 18F-FDG-PET images. PLoS One. 2013;8(2):e57105.
- Tuli R, Yang W, Tighiouart M, Yue Y, Fraass B, Sandler HM Hendifar AE, Nissen NN, Oschin S. 18F-FDG PET as a predictor of resectability and clinical outcomes in locally advanced pancreatic cancer patients treated with radiotherapy. J Clin Oncol 32, 2014 (suppl 3; abstr 378)
- Vanderhoek M, Perlman SB, Jeraj R. Impact of the definition of peak standardized uptake value on quantification of treatment response. J Nucl Med. 2012 Jan;53(1):4-11.
- Nascente CM, Dhani NC, Vines D, Yeung I, Metser U, Serra S, et al. Clinical characterization of hypoxia in pancreatic ductal adenocarcinoma (PDAC) by 18F-FAZA PET and pimonidazole. J Clin Oncol 31, 2013 (Suppl.): Abstract #4049.
- Vecchiarelli S, Macchini M, Grassi E, Ferroni F, Ciccarese F, Calculli L, et al. Comparing RECIST and Choi’s criteria to evaluate radiological response to chemotherapy in patients with advanced pancreatic cancer. J Clin Oncol 31, 2013 (Suppl.): Abstract #e15069.
- Tixier F, Le Rest CC, Hatt M, Albarghach N, Pradier O, Metges JP, Corcos L, Visvikis D. Intratumor heterogeneity characterized by textural features on baseline 18F-FDG PET images predicts response to concomitant radiochemotherapy in esophageal cancer. J Nucl Med. 2011 Mar;52(3):369-78.
- Viswanath SE, Bloch NB, Chappelow JC, Toth R, Rofsky NM, Genega EM, Lenkinski RE, Madabhushi A. Central gland and peripheral zone prostate tumors have significantly different quantitative imaging signatures on 3 Tesla endorectal, in vivo T2-weighted MR imagery. J Magn Reson Imaging. 2012 Jul;36(1):213-24.
- Ahn SJ, Park MS, Kim KA, Park JY, Kim I, Kang WJ, Lee SK, Kim MJ. ¹8F-FDG PET metabolic parameters and MRI perfusion and diffusion parameters in hepatocellular carcinoma: a preliminary study. PLoS One. 2013 Aug 5;8(8):e71571.
- Heusch P, Köhler J, Wittsack HJ, Heusner TA, Buchbender C, Poeppel TD, Nensa F, Wetter A, Gauler T, Hartung V, Lanzman RS. Hybrid ¹8F-FDG PET/MRI including non-Gaussian diffusion-weighted imaging (DWI): preliminary results in non-small cell lung cancer (NSCLC). Eur J Radiol. 2013 Nov;82(11):2055-60.


