Keywords
Aneurysm, False; Pancreas; Pancreatectomy; Portal vein
INTRODUCTION
Despite declining mortality rates after pancreatic
surgery, postoperative bleeding remains one of the most
serious complications, particularly in high-volume centers
[1, 2, 3]. Bleeding occurs in 1-8% of cases, but accounts for
11-38% of mortality [4, 5, 6]. The peripancreatic vascular
structures that may be sources of bleeding are mainly the
stump of the gastroduodenal artery, hepatic artery, splenic
artery, or a branch of the superior mesenteric artery [1, 3, 4, 5, 6]. Although quite a rare occurrence, the portal venous
system can also be a source of postoperative bleeding. The
frequency of portal vein bleeding after pancreatectomy is
reportedly <1% (0.1-0.7%) [7, 8, 9]. Like arterial bleeding,
portal vein bleeding also can cause morbidity [7].
With recent advances in interventional procedures,
embolization and stent grafts have been widely
used, gaining acceptance for the treatment of arterial bleeding after pancreatectomy. Systematic reviews
comparing endovascular therapy and laparotomy for
postpancreatectomy bleeding have revealed that hemostasis
stays about the same (endovascular therapy, 76-80%;
laparotomy, 73-76%). However, the mortality rate associated
with endovascular therapy appears lower than that with
laparotomy (20-22% vs. 43-47%, respectively) [10, 11].
As to bleeding from the portal vein, no case series
appear to have been reported. We describe herein the five
consecutive patients with intra-abdominal bleeding from
the portal vein after pancreatectomy in which stent graft
repair was performed.
MATERIALS AND METHODS
Patients
Our institutional review board approved the
retrospective collection of data and data analysis for this
study, and the requirement for informed consent from the
patients was waived. Between November 2013 and August
2016, five consecutive patients (three males, two females;
median age, 75 years; age range, 66-78 years) with portal
vein bleeding after pancreatic surgery underwent placement
of a stent graft at the portal vein. The primary tumor was bile
duct carcinoma in two patients, and gall bladder carcinoma,
ampullary carcinoma, and metastatic pancreatic tumor from
renal cell carcinoma in one patient each.
The resection procedure for the tumor was
pancreaticoduodenectomy in three patients, extrahepatic
bile duct resection and partial resection of the pancreatic
head in one patient, and distal pancreatectomy in one
patient. Two patients also underwent right hepatectomy
and caudate lobectomy combined with resection and
reconstruction of the portal vein.
Stent Graft Procedures
Placement of a stent graft was performed as follows. In
the first patient, definitive surgical repair for portal vein
bleeding was attempted at the start. However, surgical
repair was difficult because of severe postoperative intraabdominal
adhesions. The therapeutic strategy was thus
changed intraoperatively to stent graft deployment. The
portal venous system was accessed by an ultrasoundguided
transhepatic approach. An 18-gauge Cliny
ultrasound puncture needle (Create Medic, Yokohama,
Japan) was placed into a peripheral portal vein branch
of the left lateral segment of the liver. The Seldinger
technique was used to place a 5-Fr sheath into the main
portal vein. Direct portography was then performed using
a 4-Fr catheter. The diameter and length of the portal vein
and the superior mesenteric vein were measured. The 5-Fr
sheath was exchanged for a 12-Fr sheath over a guidewire.
Then, a stent graft was deployed from the superior
mesenteric vein to the main portal vein. Post-dilatation
was performed with a balloon catheter. At the end of the
procedure, the punctured hepatic tract was closed with
0.035-inch coils.
In the remaining four patients, stent graft repair was
planned from the start. The portal venous system was
accessed by a transileocolic approach. The ileocolic
vein was punctured with an 18-gauge needle under
laparotomy. And, a 12-Fr sheath (n=2), 14-Fr sheath
(n=1), or 10-Fr sheath (n=1) was inserted to the superior
mesenteric vein over a guidewire. Direct portography was
then performed using a 4-Fr catheter, and the diameter
and length of the portal vein and superior mesenteric vein
were measured. A stent graft was then deployed. Postdilatation
was performed with a balloon catheter.
The stent graft was selected based on the diameters
of the portal vein and superior mesenteric vein. A Gore
Excluder contralateral leg endoprosthesis (W. L. Gore &
Associates, Flagstaff, AZ) was used in four patients, and
a Fluency stent graft (Bard, Tempe, AZ) was used in one
patient.
In two patients, the bleeding site was near the
confluence of the splenic vein and superior mesenteric
vein. The splenic vein and inferior mesenteric vein were
thus embolized with 0.035-inch coils and/or Amplatzer
vascular plug (St Jude Medical, St Paul, MN) before stent
graft deployment.
Assessments
Patients were analyzed with regard to clinical findings,
diagnosis of portal vein bleeding, stent graft deployment, and clinical outcome. To clarify the effects of stent graft
repair, results were assessed with regard to technical
success and clinical efficacy. Technical success was
defined as exact deployment of the stent graft to cover
the site of portal venous injury without complication, and
preservation of portal flow at final angiography. Clinical
efficacy was defined as freedom from portal vein bleeding
after stent graft deployment.
RESULTS
Clinical and Radiological Findings
Clinical and radiological findings are summarized in Table 1. All five patients developed pancreatic leakage
after pancreatectomy. According to the International Study
Group on Pancreatic Fistula grading [12], four patients
suffered grade B pancreatic leakage and one patient
suffered grade C pancreatic leakage.
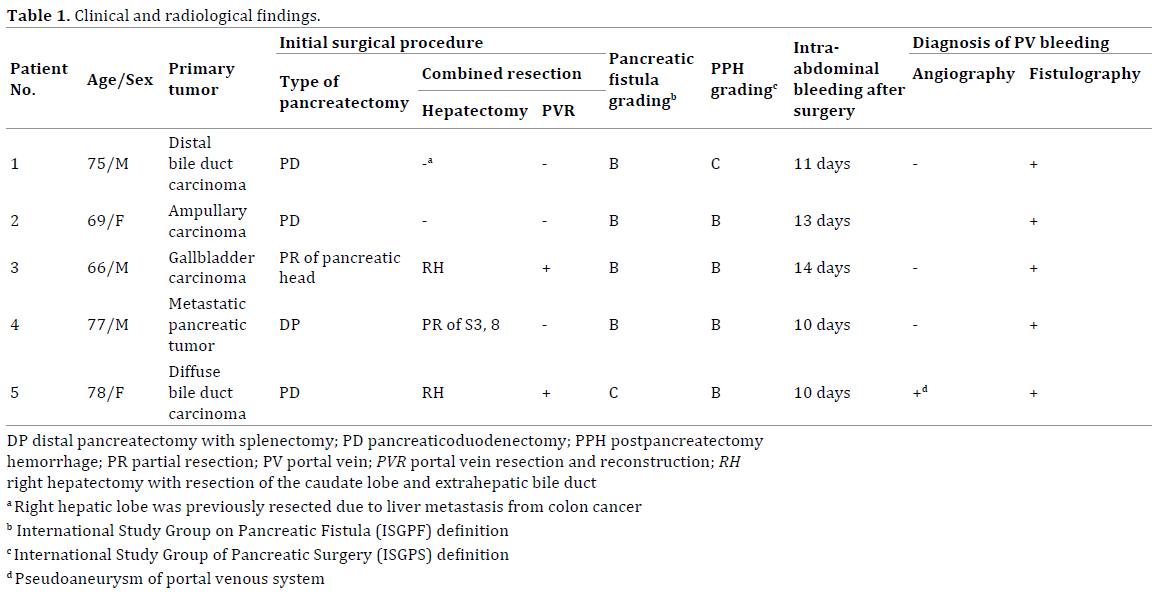
Intra-abdominal bleeding through the intraoperatively
placed drains was identified 10-14 days (median, 11
days) after initial surgery. All patients were managed by
transfusion of red blood cell and/or intravenous fluids.
According to the International Study Group of Pancreatic
Surgery grading [13], four patients suffered grade B
bleeding and one patient suffered grade C bleeding.
Emergency angiography was performed as the initial
management tool for intra-abdominal bleeding in four
patients. Selective angiography of the celiac, common
hepatic, and superior mesenteric artery demonstrated
no evidence of arterial bleeding. Venous-phase selective
angiography was also acquired as indirect portography.
Indirect portography demonstrated no evidence of venous
leakage. However, one patient showed pseudoaneurysm
at the splenic vein near the confluence with the superior
mesenteric vein (Figure 1a, b).
Figure 1. Patient No. 5: (a). Indirect portography after selective celiac arteriography and (b). 3-dimensional CT angiography show pseudoaneurysm of
the splenic vein near the confluence (arrow). (c). Portography after stent graft deployment (arrowhead) shows good portal flow. The splenic vein (white
arrow) and inferior mesenteric vein (black arrow) are embolized with a vascular plug and coils, respectively.
Following angiography to reposition and/or exchange
the peripancreatic drain, traction was placed on the drains
and contrast medium was injected via the drains in four
patients. In three of these four patients, this contrast
study showed communication between the peritoneal
cavity and portal venous system, indicating portal vein
bleeding (Figure 2a, b). In the other patient, no bleeding
site was identified at that time and tentative bleeding
repeated during follow-up. At 15 days after first bleeding,
fistulography showed the portal vein and re-bleeding was
present. In the remaining patient without angiography,
bleeding occurred during fistulography, and the portal
vein was demonstrated on fistulography. Finally, portal
vein bleeding was diagnosed by fistulography in all
patients. After fistulography, no patients developed severe
infections such as bacteremia.
Figure 2. Patient No. 3: (a). Fistulography from the drain shows the cavity of the pancreatic leakage that communicates with the portal venous system. (b).
Direct portography from the superior mesenteric vein shows contrast extravasation into the tract of the drain. (c). Portography after stent graft deployment
shows no contrast extravasation and good portal flow.
The bleeding site of the portal venous system was the
main portal vein in two patients, the confluence of the
superior mesenteric vein and portal vein in one patient,
the stump of the splenic vein in one patient, and the splenic
vein near the confluence in one patient. In four patients,
the bleeding site was where the operatively placed peripancreatic drain crossed on both fistulography and
computed tomography (CT) scan. In one patient with portal
vein pseudoaneurysm, the bleeding site was separate from
the drain, but was enclosed by pancreatic leakage.
Stent Graft Repair
The results of stent graft repair are summarized in Table 2. The interval between primary surgery and stent
graft deployment was 10-25 days (median, 13 days). In all
patients, stent grafts were successfully deployed to cover
the site of portal venous injury. And, final portography
after stent graft deployment showed good portal flow
(Figure 1c, 2c). Thus, clinical efficacy was achieved in all
five patients.

Clinical Course
Clinical courses after stent graft placement are
summarized in Table 3. The follow-up period was 2-23
months (median, 9 months). After the procedure, the
patients remained free of further portal vein bleeding.
Thus, clinical efficacy was achieved in all five patients.
Four patients were discharge in good health, but the
remaining patient died of multiorgan failure two months
after placement of a stent graft.
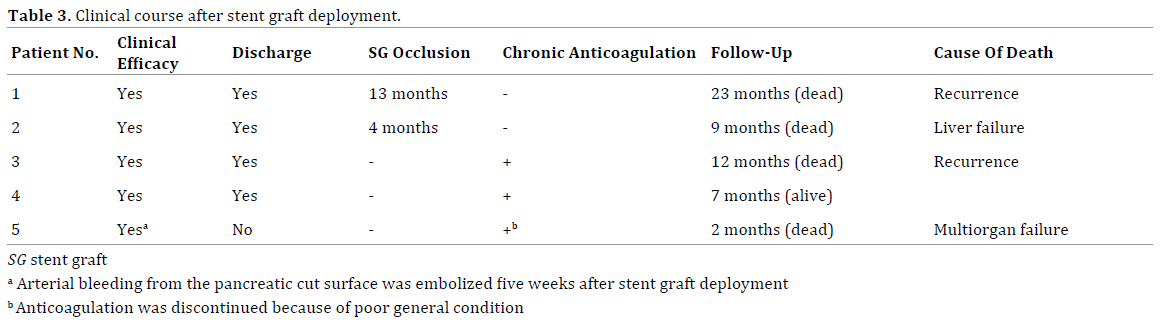
During follow-up, patency of the stent graft was
assessed by Doppler ultrasonography and/or contrastenhanced
CT scan every three-six months. The stent
graft was occluded with thrombus after 13 months in
the first patient, and after four months in the second
patient. The two earliest patients had not been receiving
chronic anticoagulation therapy. Systemic anticoagulation
therapy was initiated after stent graft occlusion. However,
recanalization of portal flow was not achieved. The last
three patients therefore received chronic anticoagulation therapy using warfarin after placement of a stent graft.
However, anticoagulation therapy was immediately
discontinued in one of the three patients because of poor
general condition. All three patients remained free of stent
graft thrombus during follow-up.
DISCUSSION
Although the exact mechanisms underlying
postpancreatectomy bleeding remain elusive, pancreatic
leakage and localized infection are thought to represent
major contributors [5, 14]. The effects of localized infection
and pancreatic juices likely weaken and erode the blood
vessel walls. Mechanical irritation by the drain is another
cause of bleeding [15]. In our series, pancreatic leakage
occurred in all patients, and the drain was in contact with
the bleeding site in four of the five patients. Previous
articles of portal vein bleeding have also reported bleeding
sites in proximity to the drain [16, 17].
Indirect portography following selective arteriography
could not detect a bleeding source in three of the four
patients. Previous article has also reported postulated
causes of false-negative angiography, including pauses in
intermittent bleeding or a venous origin of bleeding, which
is difficult to identify after arteriography [2]. In one patient,
indirect portography could demonstrate pseudoaneurysm
at the splenic vein. Burke et al. [17] reported a similar case
in which portal vein pseudoaneurysm was diagnosed by
indirect portography. When arteriography fails to identify
a bleeding source, consideration of the possibility of
bleeding from the portal venous system is also important.
On the other hand, fistulography was helpful to identify
bleeding sites involving the portal venous system in all five
patients. Fistulography demonstrated not only a cavity associated with leakage, but also the portal vein, indicating
portal vein bleeding. Yoshida et al. [8] and Ginsburg et al.
[16] also described the utility of fistulography to diagnose
portal vein bleeding. Our study agrees with previous
reports, and fistulography seems to offer the valuable
modality to elucidate bleeding sites of the portal vein.
Choice of treatment for portal vein bleeding after
pancreatectomy may depend on the clinical presentation.
Reported approaches to treatment include surgical
repair [9, 17], stent grafting [16], and temporary balloon
occlusion and conservation [8]. In our first patient, we
abandoned definitive surgical repair because of severe
intra-abdominal adhesions. The treatment strategy was
therefore changed to stent graft repair intraoperatively.
Our experience with this patient led us to select stent
grafts as the first-line treatment in the next four patients.
The use of stent grafts in the treatment of postoperative
arterial bleeding appears feasible, effective, and safe [18, 19]. Stent grafts are now considered the first-line treatment
for arterial bleeding under critical condition in which the
consequences of hepatic artery or superior mesenteric
artery occlusion may be disastrous. In the same manner
as for arterial bleeding, the use of stent grafts for portal
vein bleeding offers a reliable treatment option. In our
series, all patients achieved hemostasis and avoided rebleeding
from the portal vein. However, surgery remains a
therapeutic option when endovascular procedures are not
available.
To deploy a stent graft at the portal vein, either a
transhepatic or a transileocolic approach can be applied.
Other reports [16, 20, 21] have selected the percutaneous
transhepatic approach. The merit of that approach is the
reduced invasiveness compared to the transileocolic
approach, because the transileocolic approach requires
laparotomy. However, a transileocolic approach also has
some advantages in patients with postsurgical bleeding.
Laparotomy allows the treatment of factors that contribute
to bleeding, such as anastomotic disruption or intraabdominal
collections.
The necessity of anticoagulation therapy after stent
graft deployment at the portal vein remains unclear.
Our first two patients were followed without chronic
anticoagulation therapy, but the stent grafts were
thrombosed after 13 months and 4 months, respectively.
Later patients were therefore administered warfarin just
in case. Although the follow-up periods were very short,
the patency of the stent grafts has been preserved without
thrombus. Further studies are required to evaluate
the necessity of prophylactic anticoagulation therapy
following stent graft deployment.
The present study showed limitations related to
the retrospective design and small cohort size. This is
because portal vein bleeding after pancreatectomy is
quite a rare complication compared with arterial bleeding.
Accumulation of further cases is thus necessary to assess
the clinical features and efficacy of stent graft repair.
CONCLUSION
In conclusion, the portal vein has the potential to
cause intra-abdominal bleeding after pancreatic surgery.
Fistulography appears useful in diagnosing portal vein
bleeding, and placement of a stent graft is available
as a therapeutic option for portal vein bleeding after
pancreatectomy.
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Correa-Gallego C, BrennanMF, D'Angelica MI, Dematteo RP, Fong Y,
Kingham TP, et al. Contemporary experience with postpancreatectomy
hemorrhage: results of 1,122 patients resected between 2006 and 2011. J
Am Coll Surg 2012; 215:616-21. [PMID: 22921325]
- Wellner UF, Kulemann B, Lapshyn H, Hoeppner J, Sick O, Makowiec
F, et al. Postpancreatectomy hemorrhage-incidence, treatment, and risk
factors in over 1,000 pancreatic resections. J Gastrointest Surg 2014;
18:464-75. [PMID: 24448997]
- Yekebas EF, Wolfram L, Cataldegirmen G, Habermann CR, Bogoevski
D, Koenig AM, et al. Postpancreatectomy hemorrhage: diagnosis and
treatment: an analysis in 1669 consecutive pancreatic resections. Ann
Surg 2007; 246:269-80. [PMID: 17667506]
- van Berge Henegouwen MI, Allema JH, van Gulik TM, Verbeek PC,
Obertop H, Gouma DJ. Delayed massive haemorrhage after pancreatic and
biliary surgery. Br J Surg 1995; 82:1527-31. [PMID: 8535810]
- Tien YW, Lee PH, Yang CY, Ho MC, Chiu YF. Risk factors of massive
bleeding related to pancreatic leak after pancreaticoduodenectomy. J Am
Coll Surg 2005; 201:554-9. [PMID: 16183493]
- Trede M, Schwall G. The complications of pancreatectomy. Ann Surg
1988; 207:39-47. [PMID: 3276272]
- Treckmann J, Paul A, Sotiropoulos GC, Lang H, Ozcelik A, Saner F, et
al. Sentinel bleeding after pancreaticoduodenectomy: a disregarded sign.
J Gastrointest Surg 2008; 12:313-8. [PMID: 17952516]
- Yoshida T, Matsumoto T, Morii Y, Aramaki M, Bandoh T,
Kawano K, et al. Delayed massive intraperitoneal hemorrhage after
pancreatoduodenectomy. Int Surg 1998; 83:131-5. [PMID: 9851330]
- Boggi U, Del Chiaro M, Croce C, Amorese G, Signori S, Vistoli F, et al.
Vascular complications of pancreatectomy. JOP. J Pancreas 2007; 8:102-
13. [PMID: 17228142]
- Limongelli P, Khorsandi SE, Pai M, Jackson JE, Tait P, Tierris
J, et al. Management of delayed postoperative hemorrhage after
pancreaticoduodenectomy: a meta-analysis. Arch Surg 2008; 143:1001-
7. [ PMID: 18936380]
- Roulin D, Cerantola Y, Demartines N, Schäfer M. Systematic review
of delayed postoperative hemorrhage after pancreatic resection. J
Gastrointest Surg 2011; 15:1055-62. [PMID: 21267670]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J,et al.
Postoperative pancreatic fistula: an international study group (ISGPF)
definition. Surgery 2005; 138:8-13. [PMID: 16003309]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ,
et al. Postpancreatectomy hemorrhage (PPH): an International Study
Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20-5.
[PMID: 17629996]
- Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI. Delayed hemorrhage
after pancreaticoduodenectomy. J Am Coll Surg 2004; 199:186-91.
[PMID: 15275871]
- Suzuki K, Mori Y, Komada T, Matsushima M, Ota T, Naganawa S. Stentgraft
treatment for bleeding superior mesenteric artery pseudoaneurysm
after pancreaticoduodenectomy. Cardiovasc Intervent Radiol 2009;
32:762-6. [PMID: 19184196]
- Ginsburg M, Ferral H, Alonzo MJ, Talamonti MS. Percutaneous
transhepatic placement of a stent-graft to treat a delayed mesoportal
hemorrhage after pancreaticoduodenectomy. World J Surg Oncol 2014;
12:315. [PMID: 25315011]
- Burke CT, Park J. Portal vein pseudoaneurysm with portoenteric
fistula: an unusual cause for massive gastrointestinal hemorrhage. Semin
Intervent Radiol 2007; 24:341-5. [PMID: 21326482]
- Lim SJ, Park KB, Hyun DH, Hyun DH, Do YS, Park HS, et al. Stent
graft placement for postsurgical hemorrhage from the hepatic artery:
clinical outcome and CT findings. J Vasc Interv Radiol 2014; 25:1539-48.
[PMID: 25149115]
- Bellemann N, Sommer CM, Mokry T, Kortes N, Gnutzmann D, Gockner
T, et al. Hepatic artery stent-grafts for the emergency treatment of acute
bleeding. Eur J Radiol 2014; 83:1799-803. [PMID: 25059599]
- Charvat F, Maskova J, Belina F, Buric I, Lacman J, Fuksa Z, et al. Portal
vein erosion: a rare hemorrhagic complication of acute pancreatitis
treated by percutaneous stent-graft placement. J Vasc Interv Radiol 2010;
21:411-2. [PMID: 20171562]
- Ierardi AM, Berselli M, Cuffari S, Castelli P, Cocozza E, Carrafiello G.
Uncommon case of a post-traumatic portal vein pseudoaneurysm treated
with percutaneous transhepatic stent grafting. Cardiovasc Intervent
Radiol 2016; 39:1506-1509. [PMID: 27230514]



