Keywords
Ampulla of Vater; Carcinoma, Signet Ring Cell; Pancreas
Abbreviations
SRCC: signet-ring cell carcinoma
INTRODUCTION
Most tumours of the ampulla of Vater are welldifferentiated adenocarcinomas. Signet-ring cell carcinoma (SRCC) is a very rare histological variant found at this site, being more common in the stomach than elsewhere in the digestive system [1]. Including the original report by Sekoguchi et al. in 1979 [2], 31 previous cases of ampullary SRCC have been mentioned in medical literature. We here present an elderly patient who underwent Whipple’s procedure, in whom poorly-differentiated ampullary SRCC without nodal metastasis was confirmed on histological examination of the resected specimen.
CASE REPORT
A 78-year-old woman presented to our institution with a three-week history of tiredness, postprandial vomiting, jaundice and pruritus. She additionally reported oily stools. Her past medical history included hypothyroidism, chronic cystitis and a left knee replacement. She was visibly icteric, but physical examination was otherwise unremarkable, without any abdominal tenderness or palpable breast masses. Routine laboratory investigations revealed elevated alanine transaminase 106 IU/L (reference range: 0-40 IU/L), alkaline phosphatase 730 IU/L (reference range: 30-130 IU/L), and bilirubin 182 μmol/L (reference range: 0-17 μmol/L), with normal inflammatory markers.
Abdominal ultrasound demonstrated gross dilatation of the common bile and pancreatic ducts, and gallbladder, the latter containing several small calculi. A 2 cm soft tissue mass was suggested at the level of the ampulla of Vater. Subsequent staging CT scan confirmed the marked common bile and pancreatic duct dilatation. However, no definite ampullary mass lesion was identified; a bulky pancreatic head was noted, with a homogenous texture similar to the rest of the pancreas. There was no ultrasound or CT evidence of local spread, vascular encasement or distant metastatic disease. Endoscopic retrograde cholangiopancreatography (ERCP) suggested a duodenal tumour at the ampulla, but a stent could not be placed across the stricture and biopsy was not taken.
The patient underwent Whipple’s resection and cholecystectomy. At operation, a large mass was found at the head of the pancreas, involving the first and second parts of the duodenum, and invading into the hepatic aspect of the transverse colonic mesentery. Following an uncomplicated post-operative course, the patient was discharged home. She did not receive adjuvant chemoradiotherapy, and had no evidence of recurrence at six-month follow-up.
On histological analysis, an ill-defined lesion measuring 12 mm in maximum dimension was noted near the ampulla, extending to its anterior margin (Figure 1). The tumour measured 30 mm in maximum dimension within the duodenal submucosa, from where it ulcerated into the duodenal mucosa, surrounding blood vessels, the ampullary duct and the common bile duct (Figure 2). It infiltrated the duodenal muscularis propria and extended into the pancreatic parenchyma, reaching 16 mm from the superior mesenteric vein. Although there was extensive perineural invasion with infiltration of the duodenal mucosal and submucosal lymphatics, the pancreatic resection margin was not involved, and 0/13 peripancreatic and 0/10 greater curve lymph nodes were all free of tumour (T3N0M0). Microscopic appearances showed a poorlydifferentiated signet-ring cell carcinoma, composed entirely of round cells containing intra-cytoplasmic mucin (Figure 3). Immunohistochemical staining was strongly positive for cytokeratin (CK) 7, CK20, CK8/18, CK19, CEA mono, CA 19-9, CA 125, MUC1 and MUC5AC. Tumour cells showed no expression for MUC2, MUC6, SMAD4, CDX2, ER and PgR. This immunohistochemical staining pattern is highly suggestive of signet-ring cell carcinoma of pancreatobiliary origin [3].
Figure 1. Axial slice of the head of the pancreas demonstrating
marked narrowing of the duodenum by peri-ampullary polypoid
tumour nodules (arrow). A scale with 1 cm intervals is shown.
Figure 2. Histological section (H&E, x20) showing a diffuse tumour
(arrow) located mainly within the duodenal mucosa, encircling the
ampullary duct and extending into the pancreatic parenchyma.
Figure 3. Higher magnification (DPAS, x200) reveals poorlydifferentiated
signet-ring cell carcinoma composed of single, noncohesive,
round and vacuolated cells containing intra-cytoplasmic
mucin.
DISCUSSION
Adenocarcinoma of the ampulla of Vater is a rare clinical entity, occurring in less than six cases per million people annually [4]. It accounts for 0.2% of all gastrointestinal and 6% of periampullary malignancies [4, 5]. SRCC represents a variant of adenocarcinoma, characterised by the presence of greater than 50% signet-ring cells with intra-cytoplasmic mucin, and typically eccentrically-located crescent-shaped nuclei [4]. It may arise in any organ, especially in the stomach where it comprises 15-30% of all gastric cancers [5].
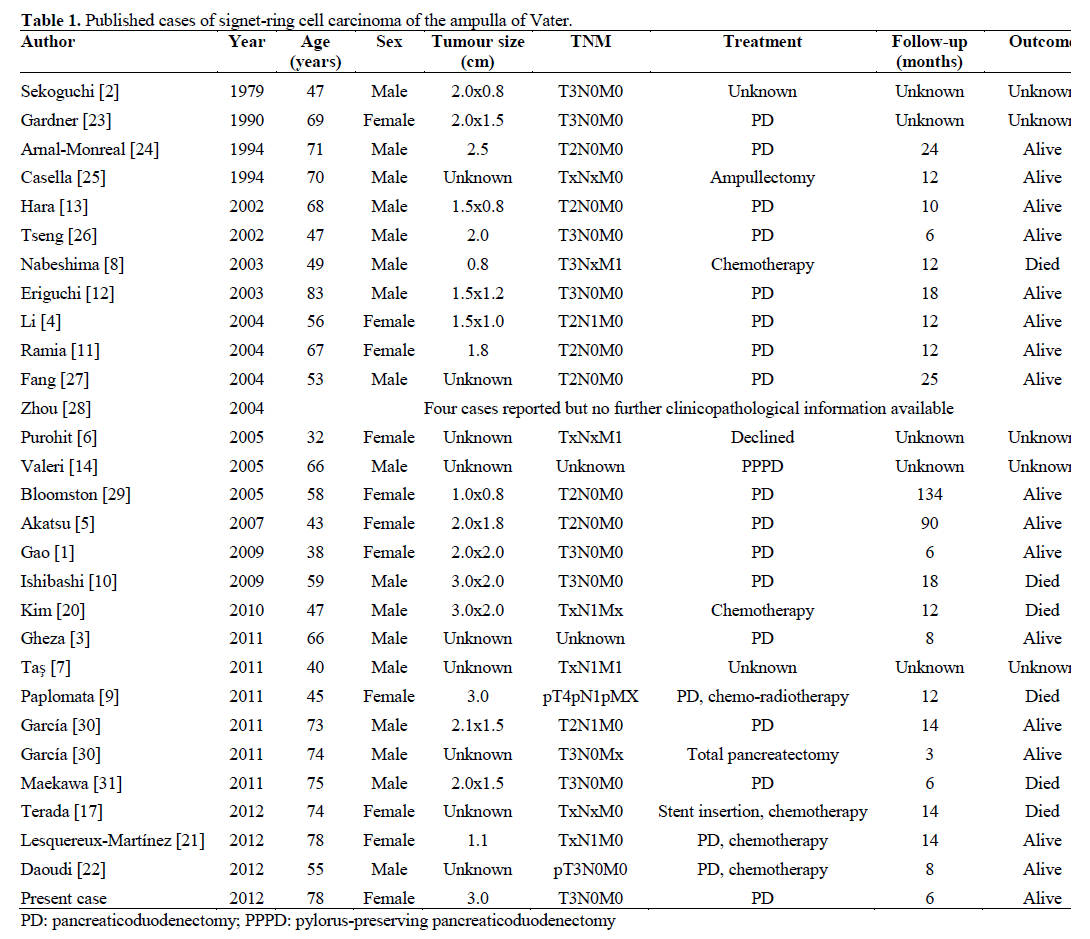
We here present the 32nd report of SRCC of the ampulla of Vater in medical literature (Table 1). From available demographic information, the 30 preceding cases included 16 males and 9 females aged between 32 and 83 years of age. One patient presented with T4 disease, ten patients with T3 disease and eight with T2 disease. Diagnostic imaging detected metastatic lung, liver and bone disease in one patient [6], and multiple pulmonary metastatic deposits in another [7]. Disseminated carcinomatosis was noted on presentation in a Japanese patient [8], whilst leptomeningeal metastases were detected in another patient following adjuvant chemotherapy for ampullary SRCC [9].
The rarity of ampullary SRCC is compounded by its unclear histological genesis. Since SRCC is more frequently encountered within gastric epithelium, it has been suggested that this tumour may arise from ectopic gastric mucosa situated at the ampulla [10, 11]. Another theory proposes that SRCC originates from gastric-type metaplasia occurring as a protective response to increased acidity, a recognised phenomenon in peptic ulcer disease [10, 11]. Although peri-tumoural ectopic gastric mucosa was found in two previous patients with SRCC, none was found in our patient, who also did not suffer peptic ulcer disease.
Immunohistochemical staining patterns allowing further classification of ampullary SRCC to a pancreatobiliary- or intestinal-type have been described [3]. Expression of CK7, along with negativity for CK20, CDX-2 and MUC2 signifies pancreatobiliarytype SRCC, and vice-versa. Based on these staining patterns, tumour cells in the present case were suggestive of a pancreatobiliary-type origin, which is associated with a less favourable outcome [3, 12].
It is known that SRCC elsewhere in the gastrointestinal tract has a poor prognosis [1, 3, 5]. Similarly, poorlydifferentiated ampullary adenocarcinoma usually signifies advanced-stage disease, with the occurrence of nodal metastasis and pancreatic invasion [5]. Although our patient’s tumour featured poorlydifferentiated signet-ring cells, there was no lymph node involvement at presentation. Indeed, prognosis seems closely related to the extent of neural invasion and nodal metastasis at the time of surgery [3]. Nevertheless, prognosis is difficult to ascertain in ampullary SRCC, compared to ampullary adenocarcinoma, owing to the limited number of reports so far.
The majority of patients in previous cases of ampullary SRCC underwent pancreaticoduodenectomy, occasionally with extended lymphadenectomy and/or partial gastrectomy. This radical approach facilitates lymph node dissection in advanced disease states, but a pylorus-preserving technique, which has been utilised in three previous cases of ampullary SRCC [9, 13, 14], may be more applicable in early disease, where curability is balanced by a more moderate resection. Although currently a controversial strategy, pyloruspreserving pancreaticoduodenectomy for suspected peri-ampullary malignancy has been shown to be comparable to classical Whipple’s operation, in terms of operating time, intra-operative blood loss, complications such as delayed gastric emptying, as well as disease-free survival [15, 16]. Nevertheless, our patient recovered in an uneventful manner following Whipple’s resection. Interestingly, one group successfully performed ampullectomy using a transduodenal approach for ampullary SRCC, with no evidence of disease at twelve month follow-up; this technique has not been utilised since. Endoscopic stent insertion has also been reported as a conservative treatment [17].
We performed a classical Whipple’s procedure to maximise curative potential, since pre-operative histological diagnosis was not available. On account of negative resection margins and absence of nodal involvement, post-operative chemotherapy was not deemed necessary.
Chemoradiotherapy based on 5-fluorouracil has been employed as an adjunctive treatment modality following curative resection of ampullary adenocarcinomas. However, there is debate as to whether this actually affords a statistically significant survival benefit, since many patients develop metastatic disease [18, 19]. Presently, no established adjuvant chemotherapeutic regimen exists specifically for ampullary SRCC, although documented antineoplastic agents have been used in five cases.
Nabeshima et al. treated a 49-year-old male patient with ampullary SRCC and secondary bone metastasis (pT3NxM1) with 5-fluorouracil and leucovorin, reporting increased survival and quality of life [8]. Another 45-year-old male patient with pT4pN1pMX ampullary SRCC received six months of adjuvant gemcitabine and oxaliplatin, but three months subsequently developed leptomeningeal metastases, with a poor response to intrathecal methotrexate [9]. In Kim et al.’s report, a 47-year-old male patient, found to have multiple nodal metastases at operation, was conservatively managed with biliary stenting and titanium silicate/cisplatin chemotherapy, but died one year post-diagnosis [20]. In contrast, Lesquereux- Martínez et al. treated a 78-year-old female patient with ampullary SRCC and minimal neoplastic nodal infiltration (1/21 lymph nodes) with adjuvant gemcitabine, finding her disease-free at 14 months [21]. In Douadi et al.’s report, a 55-year-old male patient with pT3N0M0 disease received six cycles of adjuvant gemcitabine/cisplatin, without disease recurrence at eight months [22].
Thus, adjuvant chemotherapy may be appropriate in the treatment of ampullary SRCC associated with locoregional metastasis. However, its role in node-negative and distant metastatic disease remains as yet undetermined and, from the case reports evaluated, consensus regarding the optimum chemotherapeutic regimen is lacking.
In conclusion, we here report a very rare case of poorly-differentiated ampullary carcinoma with signetring features, but without distant metastatic disease. We believe the tumour arose from pancreatobiliary epithelium, according to immunohistochemical staining patterns. Whilst pancreaticoduodenectomy can afford a good outcome in early, node-negative SRCC, the longterm prognosis remains uncertain.
Conflicts of interest
The authors declare they have no conflicts of interest to disclose
Source of funding
No external sources of funding
References
- Gao JM, Tang SS, Fu W, Fan R. Signet-ring cell carcinoma of the ampulla of Vater: contrast-enhanced ultrasound findings. World J Gastroenterol. 2009;15:888-91. [PMID: 19230055]
- Sekoguchi T, Mizumoto R. Clinicopathological study of papilla of Vater. GekaChiryo. 1979;41:1-5.
- Gheza F, Ceryi E, Pulcini G, Villanacci V, Giulini SM, Schiavo- Lena M, Ferrari AB, et al. Signet ring cell carcinoma of the ampulla of Vater: demonstration of pancreatobiliary origin. Pancreas. 2011;40:791-3. [PMID: 21673543]
- Li L, Chen QH, Sullivan JD, Breuer FU. Signet-ring cell carcinoma of the ampulla of Vater. Ann Clin Lab Sci. 2004;34:471- 5. [PMID: 15648791]
- Akatsu T, Aiura K, Takahashi S, Kameyama K, Kitajima M, Kitagawa Y. Signet-ring cell carcinoma of the ampulla of Vater : report of a case. Surg Today. 2007;37:1110-4. [PMID: 18030577]
- Purohit RC, Kant K, Bhargava N, Kothari N, Purohit V. Signet ring cell carcinoma of ampulla of Vater in a young adult. Indian J Gastroenterol. 2005;24:222-3. [PMID: 16361773]
- TasA, Ozer E, Köklü S, Kocak E. Signet ring cell carcinoma of the ampulla of vater: rare cause of acute pancreatitis. Scand J Gastroenterol. 2011;46:126-7. [PMID: 20950208]
- Nabeshima S, Kishihara Y, Nabeshima A, Yamaga S, Kinjo M, Kashiwagi S, Hayashi J. Poorly differentiated adenocarcinoma with signet-ring cells of the Vater’s ampulla, without jaundice but with disseminated carcinomatosis. Fukuoka IgakuZasshi. 2003;94:235- 40. [PMID: 14509231]
- Paplomata E, Wilfong L. Signet ring cell carcinoma of the ampulla of Vater with leptomeningeal metastases: a case report. J ClinOncol. 2011;29:e627-9. [PMID: 21606434]
- Ishibashi Y, Ito Y, Omori K, Wakabayashi K. Signet ring cell carcinoma of the ampulla of Vater. A case report. JOP. 2009;10:690- 3. [PMID: 19890196]
- Ramia JM, Mansilla A, Villar J, Muffak K, Garrote D, Ferron JA. Signet-ring cell carcinoma of the Vater’s ampulla. JOP. 2004;5:495-7. [PMID: 15536289]
- Eriguchi N, Aoyagi S, Jimi A. Signet-ring cell carcinoma of the ampulla of Vater: report of a case. Surg Today. 2003;33:467-9. [PMID: 12768376]
- Hara T, Kawashima H, Ishigooka M, Kashiyama M, Takanahi S, Hosokawa Y. Signet-ring-cell carcinoma of the ampulla of Vater: a case report. Hepatogastroenterology. 2002;49:561-3. [PMID:11995497
- Valeri S, Caricato M, Ripetti V, Crucitti P, Ausania F, Garberini A, et al. Signet-ring cell carcinoma of the Vater’s ampulla: report of a clinical case. SupplTumori. 2005;4:S61. [PMID: 16437905]
- Tran KT, Smeenk HG, van Eijck CH, Kazemier G, Hop WC, Greve JC, Terpstra OT et al. Pylorus-preserving pancreaticoduodenectomy versus standard Whipple procedure: a prospective, randomized, multicenter analysis of 170 patients with pancreatic and periampullarytumours. Ann Surg. 2004;240:738-45. [PMID: 15492552]
- Diener MK, Fitzmaurice C, Schwarzer G, Seiler CM, Antes G, Knaebel HP, Büchler MW. Pylorus-preserving pancreaticoduodenectomy (ppWhiple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma. Cochrane Database Syst Rev. 2011 May 11;(5):CD006053. [PMID 21563148]
- Terada T. Primary signet-ring cell carcinoma of the ampulla of Vater: a case report with an immunohistochemical study. ApplImmunohistochemMolMorphol. 2012;20:427-8. [PMID 22710820]
- Zhou J, Hsu CC, Winter JM, Pawlik TM, Laheru D, Hughes MA, et al. Adjuvant chemoradiation versus surgery alone for adenocarcinoma of the ampulla of Vater. RadiotherOncol. 2009;92:244-8. [PMID 19541379]
- Narang AK, Miller RC, Hsu CC, Bhatia S, Pawlik TM, Laheru D, et al. Evaluation of adjuvant chemoradiation therapy for ampullary adenocarcinoma: the Johns Hopkins Hospital-Mayo Clinic collaborative study. RadiatOncol. 2011;28:126. [PMID 21951377]
- Kim DI, Park SW, Lee GS, Jung GY, Jung HJ, Moon HC, et al. A Case of Signet-ring Cell Carcinoma of the Ampulla of Vater. Korean J GastrointEndosc. 2010;41:251-4.
- Lesquereux-Martínez L, Fernández-Pérez A, Bustamante- Montalvo M. Signet ring cell adenocarcinoma of the ampulla of Vater: A rare pathology. Rev EspEnferm Dig. 2012;104:501-2. [PMID 23130863]
- Daoudi K, El Haoudi K, Bouyahia N, Benlemlih A, Arifi S, Mellas N, et al. Signet Ring Cell Carcinoma of the Vater's Ampulla: A Very Rare Malignancy. Case Rep Oncol Med. 2012;2012:402798. [PMID 23056971]
- Gardner HA, Matthews J, Ciano PS. A signet-ring cell carcinoma of the ampulla of Vater. Arch Pathol Lab Med. 1990;114:1071-2. [PMID 2171451]
- ArnalMonreal FM, Lorenzo Patiño MJ, Sacristán F, Ghanimé Saide G. Signet ring cell carcinoma of the Vater's ampulla. Rev EspEnferm Dig. 1994;85:391-3. [PMID 8049111]
- Casella R, Rittmann WW, Meier R, Wegmann W, Widmer MK, Hunger T. Signet ring cell carcinoma of Vater's papilla: a very rare malignancy. HelvChirActa. 1994;60:987-90. [PMID 7876027]
- Tseng LJ, Jao YT, Mo LR. Signet ring cell carcinoma of major papilla. GastrointestEndosc. 2002;56:733. [PMID 12397285]
- Fang CL, Chu JS, Hsieh MC, Wu MS. Signet-ring cell carcinoma of the ampulla of Vater. J Formos Med Assoc. 2004;103:793-6. [PMID 15490032]
- Zhou H, Schaefer N, Wolff M, Fischer HP. Carcinoma of the ampulla of Vater: comparative histologic/immunohistochemical classification and follow-up. Am J SurgPathol. 2004;28:875-82. [PMID 15223956]
- Bloomston M, Walker M, Frankel WL. Radical resection in signet ring carcinoma of the ampulla of Vater: report of an 11-year survivor. Am Surg. 2006;72:193-5. [PMID 16536256]
- García AB, Arranz EM, Sanz RR, Serrano EM, Arranz MD, Sanz-Agero PG, et al. Signet ring cell carcinoma of the ampulla of Vater. GastroenterolHepatol. 2011;34:141-6. [PMID 21376425]
- Maekawa H, Sakurada M, Orita H, Sato K. Signet-ring cell carcinoma co-existing with adenocarcinoma of the ampulla of vater. A case report. JOP. 2011;12:162-6. [PMID 23186645]




