Nalini Sharma*, Dina Aisha Khan, Roma Jethani, Surjit Baruah and Biswajit Dey
Department of Obstetrics and Gynaecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India
*Corresponding Author:
Nalini Sharma
Department of Obstetrics and Gynaecology
North Eastern Indira Gandhi Regional
Institute of Health and Medical Sciences Shillong, Meghalaya, India
Tel: 0364-2538022
E-mail: nalinisharma100@rediffmail.com
Received date: May 31, 2018; Accepted date: July 05, 2018; Published date: July 10,2018
Citation: Sharma N, Khan DA, Jethani R, Baruah S, Dey B (2018) Perineal Endometriosis in an Episiotomy scar: A Case Report and Review of Literature. Gynecol Obstet Case Rep Vol.4:No.2:66.. doi:10.21767/2471-8165.1000066
Keywords
Endometriosis; Scar endometriosis; Perineal endometriosis; Endoanal ultrasonography
Introduction
Endometriosis is defined as the presence of functional endometrial tissue outside the uterine cavity [1]. It is mostly an endopelvic disease and commonly occurs in the ovaries, uterosacral ligaments, fallopian tubes, pelvic peritoneum, vagina, pouch of Douglas, gastrointestinal tract, Extra pelvic endometriosis like in inguinal hernia sac, incisional scars after gynaecological surgery and caesarean section is a relatively uncommon disease, accounting for approximately 1% of all cases [2,3] out of which perineal scar endometriosis incidence is reported to be 0.3% to 1% [1]. Endometriosis in an episiotomy scar is very rare (occurring in only 0.00007% of births) [4] Despite numerous studies, considerable controversy remains regarding the pathogenesis, natural history, and optimal treatment of this disorder [1]. The treatment of choice is total wide excision, which is diagnostic and therapeutic. Medical treatment with progestogens, oral contraceptive pills, and danazol provides only partial relief and does not ablate the lesion [5]. As episiotomy is very frequently performed at the time of vaginal delivery one should know about this rare entity, various measures to prevent its occurrence, early diagnosis and management options. We present a case of episiotomy endometriosis which present 9-years of last delivery.
Case Report
A 37-year-old P2L2 lady after 9 years of her last delivery presented with cyclical pain in the perineum for past 1 year. Pain started just before onset of menstruation and lasted through out her period. Pain was moderate and localized and progressive. Patient had to take analgesics for pain relief. She didn’t notice any swelling at perineum. She also had history of itching at the same site. The patient was continent and there was no history of difficulty in passing stool or urine or painful coitus. She had her first delivery 15-year back and second delivery was 10 years back.
Both were normal vaginal delivery with episiotomy. There was no intrauterine manipulation in both the deliveries. There was no personal or family history of endometriosis. Her menstrual cycles were regular; flow was normal and had mild pain in the abdomen as well as episiotomy scar. On examination her vital were stable and systemic examination revealed no abnormality. On local examination of perineum: overlying skin was healthy; an old healed right medio-lateral episiotomy scar was seen. Examination during menstruation revealed reddish brown spots with blood oozing from the spots (Figure 1).
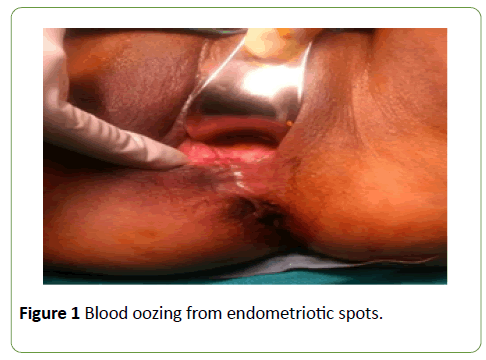
Figure 1: Blood oozing from endometriotic spots.
On palpation, a 2 × 2 cm indurated tender, firm mass was felt over the episiotomy scar. Per speculum and prevaginal examination were within normal limits. Anal sphincter and rectal mucosa were found to be uninvolved on per rectal examination. A provisional diagnosis of episiotomy scar endometriosis was made which was subjected to FNAC. FNAC report confirmed the diagnosis of endometriosis with inflammatory cell reaction. Whole abdomen ultrasonography was within normal limit.
As clinically there was no anorectal involvement and patient denied any history of anorectal complaint, endoanal ultrasonography was not performed. Incision was given on the skin overlying the mass. 4 × 4 Mass was infiltrated into elevator ani muscle. It was separated from surrounding tissue by sharp dissection.
Wide local excision of mass with 1 cm margin was done to prevent reoccurrence under spinal anaesthesia (Figure 2) and excised mass (Figure 3) sent for histopathological examination. Reconstruction of perineum was done in layers. Post operatively injection Leuprolide 3.75 mg intramuscular was given to prevent recurrence. HPE report confirmed endometriotic glands in proliferative phase. (Figure 4) Patient was followed up after 6 months with no signs symptoms of recurrence.
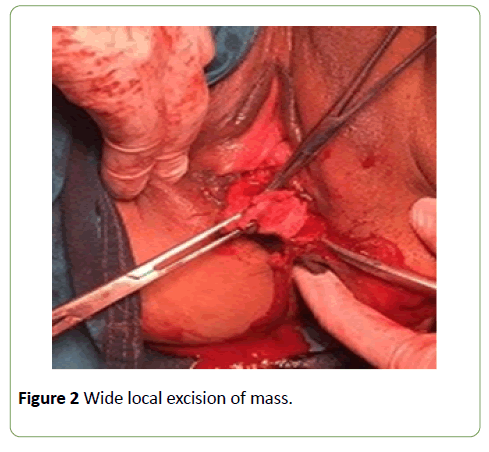
Figure 2:Wide local excision of mass.
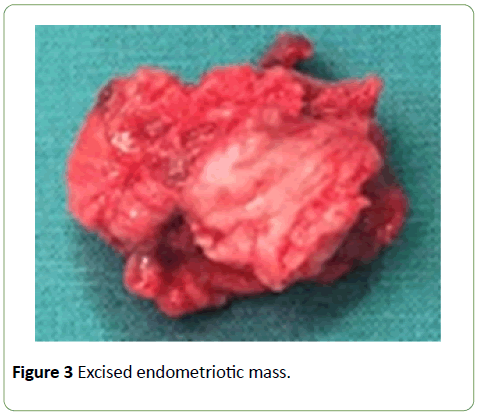
Figure 3:Excised endometriotic mass.
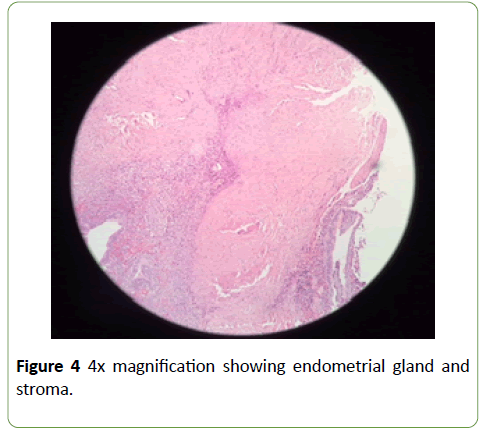
Figure 4: 4x magnification showing endometrial gland and stroma.
Discussion
First description of endometriosis in literature goes 150 years back in history by Rokitansky as presence of epithelial glands and stroma outside the uterine cavity. Extra-genital endometriosis was described in 1896 by Allen [5]. Perineal endometriosis was first reported in 1923 Scheckele, and first case of ano-perineal endometriosis of anal canal by De La Cruz in 1968 [6]. Although most cases of perineal endometriosis reported have occurred following obstetric procedures such as episiotomy [5], a rare case has been reported after ten years of Miles’ procedure for rectal cancer [7].
Out of the many theories proposed for the etiopathogenetic of endometriosis (direct implantation, lymphatic dissemination, coelomic metaplasia, or hematogenous spread), perineal endometriosis can be attributed to autologous transplantation of viable endometrial cells on episiotomy wounds after vaginal delivery, the risk is increased when manual uterine exploration or postpartum curettage are done [8,9].
Usually a classical triad of cyclic pain, perineal mass and previous episiotomy or tear is sufficient to clinch the diagnosis in scar endometriosis. Differential diagnosis of this entity includes suture granulomas, abscesses, hematomas, chelodid, lipomas, sebaceous cysts, desmoids or malignant tumour [10]. Fine needle aspiration (FNA) provides a rapid, inexpensive and accurate diagnosis and rules out other differentials; [11,12] but is stated as controversial by some authors as it might result in new endometriotic implants [4]. Imaging modalities such as ultrasound and MRI are indicated in case of large lesions, anal involvement and surgical planning. MRI is also useful to differentiate it from another lesion like lipoma, abscess. The endo-anal ultrasonography is particularly reliable for visualizing anal sphincter involvement [8]. Endo anal ultrasonography preferred over perineal ultrasonography as it can reveal anal sphincter involvement more clearly and informed the surgeon to decide surgical approach and to elucidate the potential complication of sphincteroplasty to the patient. CT-scan lacks resolution and has radiation hazard so is rarely advised [4]. For cytological diagnosis of endometriosis there must be presence of any two of three features on cytological smears -endometrial glands, stromal cells and hemosiderin laden macrophages [10].
The treatment of choice is wide resection of the lesion with 1 cm margin on all sides along with a sphincteroplasty (cases where anal sphincter is involved) [13]. Incomplete excision can lead to recurrence. Surgical method has an advantage of providing sample for biopsy to confirm diagnosis and rule out malignancy [8]. While malignant transformation is rare, few cases have been reported [14]. To prevent progressive involvement of the anal sphincter, early diagnosis and treatment is imperative [15]. Being a rare entity high index of suspicion should be kept diagnosing this entity. As episiotomy is very frequently performed at the time of vaginal delivery, incidence of perineal endometriosis can be reduced by washing the episiotomy wound with normal saline before suturing, avoiding manual uterine exploration and postpartum curettage [2,3].
Conclusion
Episiotomy scar endometriosis is essentially a clinical diagnosis. One should keep high index of suspicion when a woman in reproductive age group presents a mass and pain in scar region following an episiotomy. It is best treated with wide local excision. Involvement of anal sphincter should be carefully evaluated (clinically and endo-anal ultrasound) and ruled out before proceeding for surgical treatment. Timely treatment can prevent progressive invasion of anal sphincter and subsequent morbidity. Follow up is essential as recurrence is not uncommon.
References
- Gauna BRD, Rodriguez D, Cabre S, Callejo J (2011) A Case of Endometriosis in episiotomy scar with anal sphincter involvement. International Journal of Clinical Medicine 2: 624-626.
- Goel P, Sood SS, Dalal A, Romilla (2005) Caesarean scar endometriosis: Report of two cases. Indian Journal of Medical Sciences 59: 495-498.
- Sharma N, Thiek JL, Rituparna D, Mishra J, Singh AS (2017) Incisional endometriosis: A rare case of painful scar. Journal of Midwifery and Reproductive Health 5: 927-929.
- Vellido-Cotelo R, Muñoz-González JL, Oliver-Pérez MR, Hera-Lázaro CDL, Almansa-González C, et al. (2015) Endometriosis node in gynaecologic scars: A study of 17 patients and the diagnostic considerations in clinical experience in tertiary care center. BMC Women’s Health 15:13.
- Al-Jabri K (2009) Endometriosis at caesarian section scar. OMJ 24: 294-295.
- Laadioui M, Alaoui F, Jayi S, Bouguern H, Chaara H, et al. (2013) L’endometriose perineale profonde surcicatriced’episiotomie: A propos d’un cas rare. Pan African Medical Journal 16: 112.
- Cinardi N, Franco S, Centonze D, Giannone G (2011) Perineal scar endometriosis ten years after Miles’ procedure for rectal cancer: Case report and review of the literature. International Journal of Surgery Case Reports 2 :150–153.
- Demir M, Yildiz A, Ocal I, Yetimalar MH, Kilic D, et al. (2014) Endometriosis in episiotomy scar: A case report. J Cases Obstet Gynecol 1 :8-10.
- Paull T, Tedischi LG (1972) Perineal endometriosis at the site of episiotomy scar. Obstet Gynecol 40:28–34.
- Andola US, Andola SK, Sanghvi KJ (2012) FNAC diagnosis of Scar endometriosis: A report of 3 cases with review of literature. J Basic Clin Reprod Sci 1:62-64.
- Schoelefield HJ, Sajjad Y, Morgan PR (2002) Cutaneous endometriosis and its association with caesarean section and gynaecological procedures. J Obstet Gynaecol. 22: 553-554.
- Medeiros FC, Calvalcante DM (2011) Fine needle aspiration cytology of scar endometriosis: A study of seven cases and literature review. Diagnostic Cytopathology 39:18-21.
- Kang SK, Lee MW, Choi JH, Sung KJ, Moon KC, et al. (2002) Cutaneous endometriosis: A combination of medical and surgical treatment. J Dermatolog Treat. 13: 189-192.
- Hitti IF, Glasberg SS, Lubicz S (1990) Clear cell carcinoma arising in extraovarian endometriosis: Report of three cases and review of the literature. Gynecol Oncol. 39: 314-320.
- Jain D (2013) Perineal scar endometriosis: A comparison of two cases. BMJ Case Rep. 29:1.

