Sandeep Kumar Kar1, Tanmoy Ganguly1, Swarnali Dasgupta2, Manasij Mitra3, Riju Bhattacharya4
1Department of Cardiac Anesthesiology, Institute of Post Graduate Medical Education and Research, Kolkata, India
2Department of Anesthesiology, Institute of Post Graduate Medical Education and Research, Kolkata, India
3Department of Anaesthesiology, MGM Medical College, Kishanganj, India
4Department of Pathology, Institute of Post Graduate Medical Education and Research, Kolkata, India
*Corresponding Author:
Sandeep Kumar Kar
Assistant Professor, Department of Cardiac Anesthesiology, Institute of Post Graduate Medical Education and Research, Kolkata, India.
Tel: +919477234900
E-mail: sndpkar@yahoo.co.in
Received Date: October 16, 2015 Accepted Date: December 24, 2015 Published Date:December 30, 2015
Introduction
Cystic lesions within the pericardial space are a rare entity and comprise 7% of the mediastinal masses and 33% of mediastinal cysts [1,2]. The reported incidence of pericardial cyst is 1 in 1, 00,000 population and most cases are detected incidentally [3-6]. They are usually found in third or fourth decade of life and male and the females are affected equally [5]. Most cases are congenital and asymptomatic but life threatening complications may occur in the course of disease. They are found in the literature under various names: le kyste pleuropericardique (Jeaubert de Beaujeu, 1945; Roche, 1954), pleural cyst, pericardial cyst, pericardial coelomic cyst (Lambert, 1940), springwater cyst (Greenfield, Steinberg, and Touroff, 1943), mesothelial cyst (Churchill and Mallory, 1937), and thin-walled cyst [7].
History
(Table 1) Preliminary reports of pericardial cysts date back to middle of 19th century when the pathologists encountered the initial cases on post mortem examination [8]. Advances in radiographic imaging made antemortem diagnosis possible and Le Roux reported three cases out of 300,000 people in a mass x-ray campaign in Edinburgh in 1958 [9]. Progress in thoracic surgery ushered a new era in management of these lesions and Otto Pickhardt from Lenox Hill Hospital performed the first resection of pericardial cyst in New York in 1931 [10] in a 53 year old woman. The first reported incidence of pericardial diverticulum was presented by T. Hart of the Park Street School of Medicine in Dublin, in 1837 [11]. Later it was found pericardial cysts and diverticula represent different stages of a lesion with a common embryogenesis. Till then multiple cases of pericardial cysts had been reported as pericardial diverticula and vice versa. Greenfield et al., coined the term ‘springwater cysts’ because of their thin, transparent wall and crystal clear fluid content [12]. Surgical approach to pericardial cyst has undergone several modifications since then and currently video assisted thoracoscopic surgery is considered as the most promising technique in diagnosis and management of pericardial cysts [13- 15].
| Year |
Events |
| 1837 |
First description of a pericardial diverticulum by T. Hart of the Park Street School of Medicine in Dublin on autopsy [11]. |
| 1903 |
First pathoanatomic autopsy case series comprising 4 diverticula and 1 cyst was published by Rohn, from the Charles University of Prague [13]. First recognition of the transformational relationship between pericardial diverticulum and cyst. |
| 1931 |
Description of radiological appearance and differential diagnosis of pericardial cysts by Wallace Yater (Georgetown University) [14]. |
| 1931 |
First surgical removal of pericardial cyst by Otto Pickhardt, at Lenox Hill Hospital in New York10 |
| 1937 |
First pneumogram of pericardial cyst performed by E. H. Cushing [15]. |
| 1940 |
Adrian Lambert first suggested similar embryological origin of pericardial cyst and diverticula from disconnected mesenchymal lacunae, which later unite to form the pericardial celom [16]. |
| 1943 |
First resection of a pericardial diverticulum by Richard Sweet at Massachusetts General Hospital in Boston [17]. |
| 1943 |
Greenfield and colleagues introduced the term ‘Springwater cyst’ [12]. |
| 1958 |
Le Roux reported three cases out of 300,000 people in a mass x-ray campaign in Edinburgh [9]. |
Table 1: A brief chronology of advances in diagnosis and management of pericardial cyst and diverticulum.
Origin
Pericardial cysts are commonly congenital in origin but other causes also have been described in literature (Table 2). They usually arise from failure of fusion of one of the mesenchymal lacunae that form the pericardial sac [5]. Adrian Lambert suggested that the cyst as well as the diverticulum derive from the disconnected mesenchymal lacunae which later unite to form the pericardial celom [16,17]. Lillie et al., suggested that both pericardial cyst and diverticula both originate from the ventral recess of the pericardial coelom. Persistence of the recess forms the diverticulum, constriction of the proximal part of the persistent recess accounts for either a diverticulum with a narrow neck or a cyst in communication with the pericardial cavity and complete closure of the proximal recess forms the pericardial cyst [18]. Prenatal diagnosis of pericardial cyst is possible with ultrasound examination beyond 14th week [19] and cases of spontaneous regression have also been described in literature [20]. Inflammatory cysts and pseudocysts appear due to loculated pericardial effusion6. Isolated hydatid cyst of pericardium is extremely rare and they are usually found in association with myocardial cyst or cyst elsewhere in the body [21,22].
| Etiology of pericardial cyst6 |
| 1.Congenital |
| 2.Inflammatory: Rheumatic pericarditis, Bacterial infection particularly tuberculosis, Echinococcosis |
| 3.Traumatic |
| 4.Post cardiac surgery |
Table 2: Etiology of pericardial cyst6.
Clinical presentation
Patients with pericardial cysts are usually asymptomatic (up to 60-75% cases [5,23]) and the diagnosis is usually an incidental finding in chest xray. Symptoms usually appear when the cyst compresses on a nearby structure [24-26]. Common symptoms include [24,25] chronic cough, chest pain, dyspnea and a feeling of retrosternal pressure. Abdul-Mannan Masood and co-workers described a case of large pericardial cyst (11cm x 11cm) complaining of right shoulder discomfort radiating to the left shoulder, culminating in the substernal area along with shortness of breath [27]. Recurrent attacks of palpitation due to cardiac dysrrhythmias and frequent lower respiratory tract infections have also been described in literature [5]. Unusual presentation of pericardial cyst includes recurrent syncope [28], pneumonia [29], congestive heart failure and sudden cardiac death.
Diagnosis
For diagnosis of pericardial cyst and differentiate it from other diseases presenting as an isolated cystic shadow adjacent to the heart in chest x-ray (Figure 1) further imaging is necessary. Findings of different imaging modalities are depicted in Table 3. Computerised tomography scan (CT scan) (Figures 2A and Figure 2B) is considered as best modality for diagnosis and follow up as it provide excellent delineation of the pericardial anatomy and can aid in the precise localization and characterization of various pericardial lesions, including effusion, pericardial thickening, pericardial masses, and congenital anomalies [4,30,31]. Inaccuracies arise when the cyst is in an unusual location or the protein content of the cyst fluid is high [32]. It cannot distinguish malignant tissue from non-malignant fluid-filled cysts with a great degree of confidence [33]. Magnetic resonance imaging is another useful imaging modality and the fluid in the pericardial cyst produce hyperintense signal on T2-weighted MRI images and hypointense signals on T1-weighted images [32]. Elevated protein content may also distort MRI imagery as they decrease T2-weighted MRI signals and increase T1-weighted signals [32]. As a result, differentiating these lesions from hematomas or neoplasms can be quite challenging. Diffusion weighted MRI may be helpful in some cases. Echocardiography and ultrasound are also useful for assessment of functional status of the heart and follow up. Echocardiography is not preferred as primary diagnostic modality because of narrow window of visualisation and cysts at unusual sites may be missed in this technique. Characteristic features of pericardial cyst in different imaging modalities along with their advantages and disadvantages are described in Table 3 and differential diagnosis is described in Table 4 [34-37].
| CTscan [5,31,34,35] |
Characteristics: Single thin-walled, sharply defined, oval homogeneous masses without septation or solid component. No enhancement with intravenous contrast
Advantage:
Lack of motion artefact- clear and sharp image
Short acquisition time
Disadvantage:
Erroneous reporting if protein content of fluid is increased. E.g., Infection, hemorrhage
Radiation
Lack of functional assessment
Iodinated contrast
Need for breath hold
Remarks: Best diagnostic modality |
| Cardiac MRI [31,36] |
Characteristics: Intermediate- to low-intensity signal on T1-weighted sequences and high-signal intensity on T2-weighted sequences. No enhancement with intravenous contrast
Advantage:
Excellent soft tissue architecture
Disadvantage:
Time consuming
High cost
Altered signalling if cyst protein content is high
Calcification less well visualised
Stable patient only
Remarks: Best diagnostic modality if CT scan is inconclusive |
| Echocardiography and ultrasound [20,33] |
Characteristics: A homogeneous echolucent mass with minor attenuation of the ultrasound through a low-density fluid-filled structure. There also exists an echo-free space indicating its separation from the cardiac chambers.
Advantage:
Safe
Low cost
May be performed on unstable patients
Disadvantage:
Limited windows, narrow field of view
Technical difficulties in case of obesity, obstructive lung disease or immediately post- cardiothoracic surgery
Localisation of cyst at uncommon location difficult
Operator dependent
Remarks: Best diagnostic modality for follow up and image guided percutaneous aspiration |
Table 3: Imaging modalities in pericardial cyst.
| Lesion |
Differentiating feature |
| Bronchial cysts |
Lined with bronchial epithelium [30] |
| Localised pericardial effusion |
Fluid between visceral and parietal pericardium |
| Teratoma |
Usually associated with some solid components with cystic components [37] |
| Neuroenteric cyst |
Located in the right posterior chest and associated with vertebral anomalies [20] |
| Lymphangioma |
Multilocular or multiple cysts[20] |
| Congenital cysts of primitive foregut origin (bronchogenic cyst, gastroenteric cyst, and esophageal duplication cyst) |
Usually located in posterior mediastinum and lined by respective epithelium |
Table 4: Differential diagnosis of isolated cystic shadow adjacent to the heart .
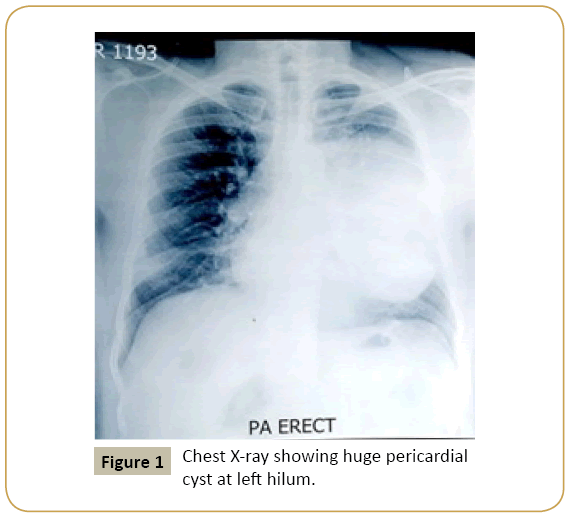
Figure 1: Chest X-ray showing huge pericardial cyst at left hilum.
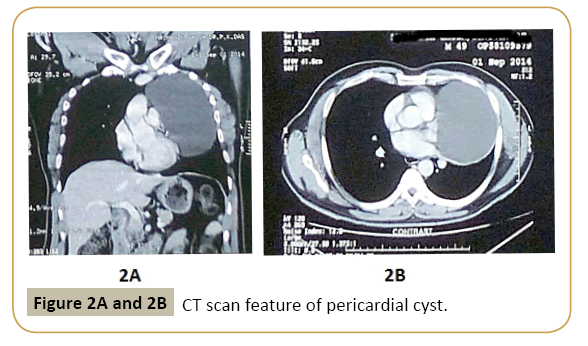
Figure 2A and 2B: CT scan feature of pericardial cyst.
Complication
Pericardial cysts are usually benign in nature but complications may arise eventually in the form of compression, inflammation, haemorrhage or rupture. Symptoms usually appear in presence of complications. Julius Chacha Mwita et al., [38] reported a case of a 22 year old female with a large (15 cmx10 cm) pericardial cyst compressing over right atrium and ventricle resulting in right heart failure. The patient had elevated jugular venous pressure, bilateral pitting pedal edema, engorged superficial veins in lower limb, ascites, hepatomegally, left varicocele and a grade 2/6 systolic ejection murmur over the precordium. The electrocardiography detected right axis deviation and incomplete right bundle-branch block. In echocardiography the inferior vena cava and hepatic veins were dilated without respiratory variation in size of the inferior vena cava. Pankaj Kaul and coworkers [39] described a case of massive benign pericardial cyst in a 66 year old woman presenting with tachycardia, dyspnoea engorged neck vein, purple discolouration of face, swelling of face and neck and wheeze over whole of right chest. CT scan, cardiac MRI and echocardiography revealed compression of the cyst over right hilum, right atrium, right ventricle, superior vena cava, the middle lobe and the anterior basal segment of the lower lobe of lung. Surgical removal of the cyst was approached by a median sternotomy. Haemorrhage within the pericardial cyst may occur spontaneously [23,40] or from external trauma [41]. Haemorrhage may cause sudden rapid expansion of the cyst and may culminate in severe pain, cardiac tamponade and congestive heart failure (Table 5) [42-51].
1. Complication due to compression of surrounding structure •Cardiac compression [23,38,39,43,44]
•Compression of right side of heart with deviation of septum
•Diastolic dysfunction
•Right ventricular outflow tract obstruction
•Pulmonary stenosis
•Mitral valve prolapsed
•Congestive heart failure
•Compression of lung: Obstruction of right main stem bronchus, Compression of adjacent lobes |
| 2. Inflammation: Pericarditis [45], Infected pericardial cyst [46] |
3. Cardiac tamponade •Intrapericardial rupture [47]
•Hemorrhage [23,40,41,48]
•Hydatid cyst rupture [49] |
| 4. Sudden death[50] |
5. Others •Atrial fibrillation [51]
•Erosion of the cyst into the superior vena cava and right ventricular wall
•Recurrent syncope [28]
•Pneumonia [29] |
Table 5: Complication of pericardial cyst [4,42].
Management
Management of pericardial cysts are similar to that of mediastinal mass [52] and should follow an algorithmic approach (Figure 3). Strategies are conservative management with follow up, percutaneous aspiration and surgery. Data regarding safety of conservative management are lacking and frequent follow up with imaging imposes anxiety and additional financial burden to the patients. Task force on the diagnosis and management of pericardial diseases of the european society of cardiology recommended percutaneous aspiration and ethanol sclerosis as initial treatment of congenital and inflammatory cysts [6]. Video assisted thoracotomy or surgical resection are recommended as second line treatment. Kinoshita et al., [53] reported a case of a 41 year old patient treated with ethanol sclerosis and no recurrence was found in 6 months follow up. However data regarding safety, efficacy and long term follow up with this technique is inadequate to support this technique as a first line treatment for all cases. The authors recommend an algorithmic approach to these patients based on presence or absence of symptoms, size of the mass, compression over the surrounding structures and patient concern. Surgery is recommended in symptomatic patients, large cysts, radiological features of compression or impending compression to vital structures, uncertainty of malignant potential and prevention of life threatening emergencies such as cardiac tamponade, obstruction of right main stem bronchus and sudden death. Video assisted thoracoscopic surgery is associated with less trauma and early postoperative recovery. The authors prefer echocardiography over CT scan for follow up for no ionising radiation and recommends CT scan to be reserved for cases with suspected complications. No treatment may be necessary in asymptomatic patients [5]. Management algorithm is outlined in Figure 3.
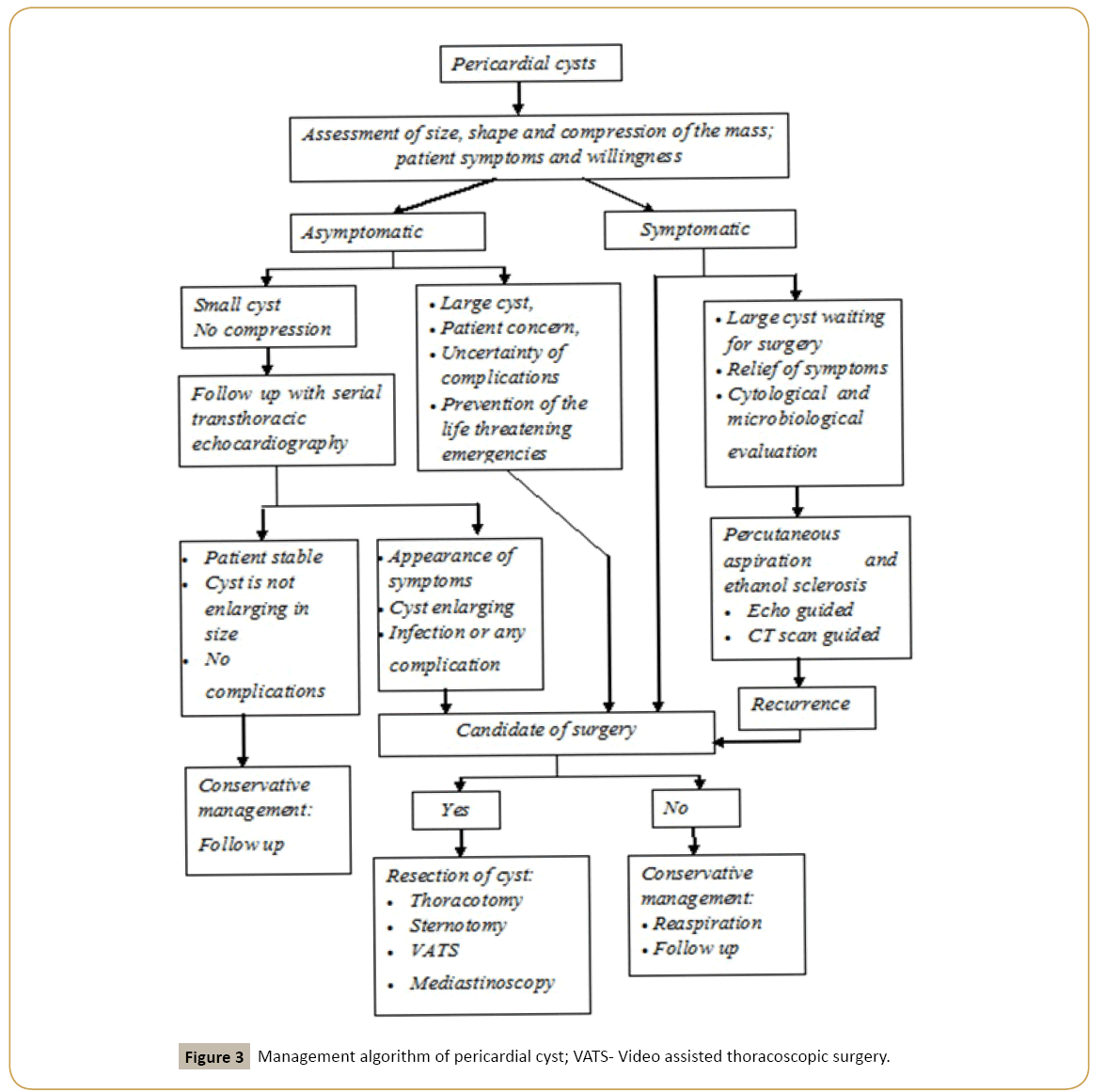
Figure 3: Management algorithm of pericardial cyst; VATS- Video assisted thoracoscopic surgery.
Conclusion
Pericardial cyst and diverticulum share similar developmental origin and may appear as an incidental finding in chest xray in an asymptomatic patient. The authors recommend CT scan as the diagnostic modality of choice in all cases and diffusion weighted cardiac MRI for cases with diagnostic confusion. Echocardiography provides a narrow window and lesions at unusual locations may be missed with this technique. The authors recommend echocardiography for follow up and image guided aspiration from the cyst. Management protocol is similar to that of mediastinal mass. Large cysts should be aspirated to reduce volume and thus the compressive effect and then resected surgically. An algorithmic approach should be followed for management depending on size, shape and compressibility of the mass, patient symptoms, surgical fitness and patient preference.
References
- Cohen AJ, Thompson L, Edwards FH, Bellamy RF (1991) Primary cysts and tumors of the mediastinum. Ann ThoracSurg 51: 378-384.
- Davis RD, Oldham HN, Sabiston DC (1987) Primary cysts and neoplasms of the mediastinum: recent changes in clinical presentation, methods of diagnosis, management, and results. Ann ThoracSurg 44: 229-237.
- Unverferth DV, Wooley CF (1979) The differential diagnosis of paracardiac lesions: pericardial cysts. CathetCardiovascDiagn 5: 31-40.
- Patel J, Park C, Michaels J, Rosen S, Kort S (2004) Pericardial cyst: case reports and a literature review. Echocardiography 21: 269-272.
- Elamin WF, Hannan K (2008) Pericardial cyst: an unusual cause of pneumonia. Cases J 1: 26.
- Maisch B, Seferović PM, Ristić AD, Erbel R, RienmÃller R, et al. (2004) Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J 25: 587-610.
- DE ROOVER P, MAISIN J, LACQUET A (1963) Congenitalpleuropericardial cysts. Thorax 18: 146-150.
- Schweigert M, Dubecz A, Beron M, Ofner D, Stein HJ (2012) The tale of spring water cysts: a historical outline of surgery for congenital pericardial diverticula and cysts. Tex Heart Inst J 39: 330-334.
- LE ROUX BT (1959) Pericardialcoelomic cysts. Thorax 14: 27-35.
- Pickhardt OC (1933) Pleuro-diaphragmatic cyst. In: Transactions of the New York Surgical Society-Stated Meeting held April 1, 1933. Ann Surg 99: 814–816.
- Hart T (1837) An account of hernia pericardii. Dublin J Med Sci 11: 365–367.
- Greenfield L, Steinberg L, Touroff AS (1943) Spring water cyst of the mediastinum. J ThoracSurg 12: 495–502.
- Rohn A (1903) Ueberdivertikel-und cystenbildung am perikard [in German]. Prag Med Wochschr 28: 461–464.
- Yater WM (1931) Cyst of the pericardium.Am Heart J 6: 710–712.
- Cushing EH (1937) Diverticulum of the pericardium. Arch Intern Med 59: 56–64.
- Lambert AV (1940) Etiology of thin-walled thoracic cysts. J ThoracSurg 10: 1–7.
- MAZER ML (1946) True pericardial diverticulum; report of a case, with safe operative removal. Am J Roentgenol Radium Ther 55: 27-29.
- LILLIE WI, McDONALD JR, CLAGETT OT (1950) Pericardialcelomic cysts and pericardial diverticula; a concept of etiology and report of cases. J ThoracSurg 20: 494-504.
- Lewis KM, Sherer DM, Gonçalves LF, Fromberg RA, Eglinton GS (1996) Mid-trimester prenatal sonographic diagnosis of a pericardial cyst. PrenatDiagn 16: 549-553.
- Bernasconi A, Yoo SJ, Golding F, Langer JC, Jaeggi ET (2007) Etiology and outcome of prenatally detected paracardial cystic lesions: a case series and review of the literature. Ultrasound ObstetGynecol 29: 388-394.
- Dasbaksi K, Haldar S, Mukherjee K, Mukherjee P (2015) A rare combination of hepatic and pericardial hydatid cyst and review of literature. Int J Surg Case Rep 10: 52-55.
- Kosecik M, Karaoglanoglu M, Yamak B (2006) Pericardialhydatid cyst presenting with cardiac tamponade. Can J Cardiol 22: 145-147.
- Borges AC, Gellert K, Dietel M, Baumann G, Witt C (1997) Acute right-sided heart failure due to hemorrhage into a pericardial cyst. Ann ThoracSurg 63: 845-847.
- Sokouti M, Halimi M, Golzari SE (2012) Pericardial cyst presented as chronic cough: a rare case report. Tanaffos 11: 60-62.
- Mejía Lozano P, Pérez Ortiz E, PuchaesManchón C (2010) Cardiac tamponade due to a pleuropericardial cyst with invasive lung cancer. Arch Bronconeumol 46: 658-659.
- Satur CM, Hsin MK, Dussek JE (1996) Giant pericardial cysts. Ann ThoracSurg 61: 208-210.
- Masood AM, Ali OM, Sequeira R (2013) A hiding in the lining: painful pericardial cyst. BMJ Case Rep 2013.
- Ilhan E, Altin F, Ugur O, Özkara S, Kayacioglu I, et al. (2012) An unusual presentation of pericardial cyst: recurrent syncope in a young patient. Cardiol J 19: 188-191.
- Forouzandeh F, Krim SR, Bhatt R, Abboud LN, Ramchandani M, et al. (2012) Giant pericardial cyst presenting as pneumonia. Tex Heart Inst J 39: 296-297.
- Lau CL, Davis RD (2004) Chapter 56: The Mediastinum, in Sabiston’s Textbook of Surgery, (17thedn.) Philadelphia, Elsevier 1738-1739 and 1758.
- Wang ZJ, Reddy GP, Gotway MB, Yeh BM, Hetts SW, et al. (2003) CT and MR imaging of pericardial disease. Radiographics 23 Spec No: S167-180.
- Raja A, Walker JR, Sud M, Du J, Zeglinski M, et al. (2011) Diagnosis of pericardial cysts using diffusion weighted magnetic resonance imaging: A case series. J Med Case Rep 5: 479.
- Jeung MY, Gasser B, Gangi A, Bogorin A, Charneau D, et al. (2002) Imaging of cystic masses of the mediastinum. Radiographics 22 Spec No: S79-93.
- Peebles CR, Shambrook JS, Harden SP (2011) Pericardial disease--anatomy and function. Br J Radiol 84 Spec No 3: S324-337.
- Verhaert D, Gabriel RS, Johnston D, Lytle BW, Desai MY, et al. (2010) The role of multimodality imaging in the management of pericardial disease. CircCardiovasc Imaging 3: 333-343.
- Rohn A (1903) Ueberdivertikel-und cystenbildung am perikard. Prag Med Wochschr 28: 461–464.
- de Bustamante TD, Azpeitia J, Miralles M, Jiménez M, Santos-Briz A, et al. (2000) Prenatal sonographic detection of pericardial teratoma. J Clin Ultrasound 28: 194-198.
- Mwita JC, Chipeta P, Mutagaywa R, Rugwizangoga B, Ussiri E (2012) Pericardial cyst with right ventricular compression. Pan Afr Med J 12: 60.
- Kaul P, Javangula K, Farook SA (2008) Massive benign pericardial cyst presenting with simultaneous superior vena cava and middle lobe syndromes. J CardiothoracSurg 3: 32.
- Marigliano A, Cirio EM, Versace R (2010) Pericardial cyst with intracystichemorrhage. A case report and review of the literature. G ItalCardiol (Rome) 11: 493-497.
- Temizkan V, Onan B, Inan K, Ucak A, Yilmaz AT (2010) Hemorrhage into a pericardial cyst and associated right ventricular compression after blunt chest trauma. Ann ThoracSurg 89: 1292-1295.
- Najib MQ, Chaliki HP, Raizada A, Ganji JL, Panse PM, et al. (2011) Symptomatic pericardial cyst: a case series. Eur J Echocardiogr 12: E43.
- Martins IM, Fernandes JM, Gelape CL, Braulio R, Silva Vde C, et al. (2011) A large pericardial cyst presenting with compression of the right-side cardiac chambers. Rev Bras Cir Cardiovasc 26: 504-507.
- Lesniak-Sobelga AM, Olszowska M, Tracz W (2008) Giant pericardial cyst compressing the right ventricle. Ann ThoracSurg 85: 1811.
- McMillan A, Souza CA, Veinot JP, Turek M, Hendry P, et al. (2009) A large pericardial cyst complicated by a pericarditis in a young man with a mediastinal mass. Ann ThoracSurg 88: e11-13.
- Hoque M, Siripurapu S (2005) Methicillin-resistant Staphylococcus aureus-infected pericardial cyst. Mayo ClinProc 80: 1116.
- El Hammoumi MM, Sinaa M, El Oueriachi F, Arsalane A, Kabiri EH (2014) [Pleuropericardial cyst rupturing into the pericardium causing tamponade]. Rev Mal Respir 31: 442-446.
- Shiraishi I, Yamagishi M, Kawakita A, Yamamoto Y, Hamaoka K (2000) Acute cardiac tamponade caused by massive hemorrhage from pericardial cyst. Circulation 101: E196-197.
- Kumar Paswan A, Prakash S, Dubey RK (2013) Cardiac tamponade by hydatid pericardial cyst: a rare case report. Anesth Pain Med 4: e9137.
- Fredman CS, Parsons SR, Aquino TI, Hamilton WP (1994) Sudden death after a stress test in a patient with a large pericardial cyst. Am Heart J 127: 946-950.
- Generali T, Garatti A, Gagliardotto P, Frigiola A (2011) Right mesothelial pericardial cyst determining intractable atrial arrhythmias. InteractCardiovascThoracSurg 12: 837-839.
- Kar SK, Ganguly T, Dasgupta CS, Goswami A (2014) Cardiovascular and Airway Considerations in Mediastinal Mass During Thoracic Surgery. J ClinExpCardiolog 5: 354.
- Kinoshita Y, Shimada T, Murakami Y, Sano K, Tanabe K, et al. (1996) Ethanol sclerosis can be a safe and useful treatment for pericardial cyst. ClinCardiol 19: 833-835.

