Keywords
Pelvic floor; Collagen; Internal urethral sphincter; Internal anal sphincter; Stress urinary incontinence
Introduction
Anatomy of the pelvic floor
The pelvic floor consists of all the structures that close the pelvic outlet from the peritoneum superiorly to the skin inferiorly. It consists of three strata. The first stratum is the pelvic peritoneum. The second stratum is the pelvic diaphragm, which is a funnel-shaped fibro-muscular partition. It consists of the pelvic diaphragm muscles and the endopelvic fascia with its condensations, the pelvic ligaments (the uterosacral ligaments, the great transverse cervical ligaments and the pubo-cervical ligaments). The third stratum is the perineum, which consists of the perineal membrane, perineal muscles, perineal fascia, and the skin [1-3].
Three major tracts traverse the pelvic floor: the urinary bladder and the urethra in front. Then there is the genital tract in the middle, and the rectum and the anal canal posteriorly. The pelvic diaphragm is the strong support of the pelvic tracts that keeps them in their proper normal position. The contributions of the pelvic floor to the structural support and the functions of the three major tracts have been the subject of controversy. With increasing age, women can develop voiding troubles, such as urgency, overactive bladder (OAB), frequency, nocturia, and stress urinary incontinence (SUI). Other concomitant troubles that occur are genital prolapse, fecal incontinence (FI), and chronic pelvic pain (CPP). All these symptoms can be associated to a greater or lesser extent with pelvic floor defects [4,5].
Micturition, urinary continence and urinary incontinence
We, recently, the physiology of micturition, consist of two stages:
The First stage: In the newborn, infancy and early childhood, when the urinary bladder (UB) is full, afferent sensations travel to the spinal cord, sacral center along S 2, 3 and 4 sensory nerves. Then efferent exciter pelvic para-sympathetic nerves S 2, 3 and 4, cause detrusor contraction leading to voiding via a relaxed urethral sphincter, irrespective of neither time nor place [6-8].
The second stage: The mother teaches and trains her offspring, toilet or potty training, how to hold up himself, until favorable social circumstances are available. Thus, the person, by learning and training will acquire high alpha-sympathetic tone (T10-L2) at the IUS, keeping it contracted and the urethra closed and empty all the time [4]. On desire or demand to void, the person will inhibit the high alpha-sympathetic tone at the IUS, which leads to its relaxation, and open the urethra [9-11]. As urine enters the urethra the pelvic para-sympathetic will be stimulated and this causes detrusor contraction. The external urethral sphincter is a voluntary muscle innervated with somatic nerve, and will relax and allows free voiding.
The internal urethral sphincter (IUS)
The IUS is a collagen-muscle tissue cylinder that extends from the bladder neck to the perineal membrane in both sexes. The collagen is a tough strong tissue that creates high wall tension, and subsequently high urethral pressure [4,5] (Figure 1).
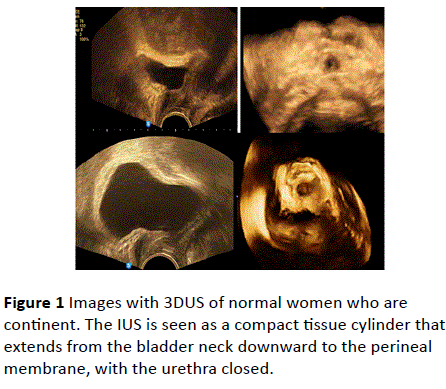
Figure 1 Images with 3DUS of normal women who are continent. The IUS is seen as a compact tissue cylinder that extends from the bladder neck downward to the perineal membrane, with the urethra closed.
The muscle is plain muscle has its nerve from the thoraciclumbar alpha sympathetic nerves T10-L2. After learning, there will be an acquired high alpha-sympathetic tone at the IUS, which keeps the urethra closed and empty all the time [8-10].
The IUS in women is intimately lying on the anterior vaginal wall. Childbirth trauma will cause overstretching of the vagina, and will lacerate the collagen chassis of the vagina and the intimately related IUS. Thus, a weak torn IUS will not stand against sudden rise of abdominal pressure, and urine will leak. This will cause embarrassment to the woman, and reflex sympathetic stimulation, will increase the existing alphasympathetic tone at the IUS preventing further leak of urine (Figure 1).
The genital tract
The vagina consists of collagen-elastic- muscle tissue cylinder. Childbirth trauma leads to overstretching of the vagina with lacerations in its collagen chassis, with subsequent patulous vagina and vaginal prolapse. The trauma may affect both the anterior vaginal wall, and the posterior vaginal wall or it may induce more damage to one of them. When the childbirth trauma affects the cervical ligaments then vault and uterine prolapse ensue [4,5]. Childbirth trauma, especially difficult labor, rapid labor, instrumental labor, frequent and multiple labors, causes overstretching of the vagina. This will cause lacerations in the collagen chassis of the vagina, and the intimately related IUS, and the internal anal sphincter (IAS) [10]. Estrogen deficiency causes atrophy of the pelvic collagen with further weakness of the collagen chassis. Chronic pelvic infection and recurrent infections lead to degeneration of the pelvic collagen with more weakness. This explains the high incidence of voiding troubles, genital prolapse and fecal incontinence (FI) after menopause [11] (Figure 2).
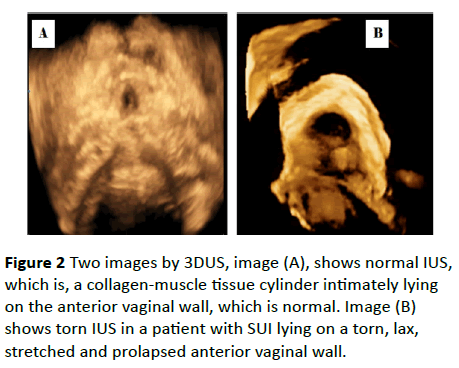
Figure 2 Two images by 3DUS, image (A), shows normal IUS, which is, a collagen-muscle tissue cylinder intimately lying on the anterior vaginal wall, which is normal. Image (B) shows torn IUS in a patient with SUI lying on a torn, lax, stretched and prolapsed anterior vaginal wall.
Defecation, fecal incontinence, and the internal anal sphincter (IAS)
The internal anal sphincter, (IAS) is a collagen-muscle tissue cylinder that surrounds the anal canal. The external anal sphincter (EAS) surrounds the lower part of the IAS. The IAS gets its nerves from the thoracic-lumbar sympathetic nerve plexus, (T10-L2). We described the physiology of defecation to consist of two stages [4,5]. The first stage in the newborn, infancy and early childhood, as the rectum is full; the pelvic parasympathetic (S 2. 3 and 4) will induce rectal muscles contraction and emptying its contents irrespective of neither time nor place [8].
The second stage, after training, in early childhood, the person will acquire high alpha-sympathetic tone at the IAS, that keeps the sphincter contracted and the anal canal closed and empty all the time. Childbirth trauma causes lacerations in the collagen chassis of the IAS that leads to its weakness and fecal incontinence (FI). Anal intercourse, also lacerate the collagen chassis of the IAS with subsequent FI. The external anal sphincter is a skeletal muscle that has its nerve supply from the systemic nervous system. It relaxes on defecation to allow passage of the stool. In addition, it voluntary, contracts and relaxes to push away the expelled stool [11].
In conclusion, childbirth trauma causes lacerations of the collagen chassis of the vagina and the intimately related IUS in front, and the IAS posteriorly, leading to vaginal prolapse, urinary incontinence (UI), and FI (Figure 3).
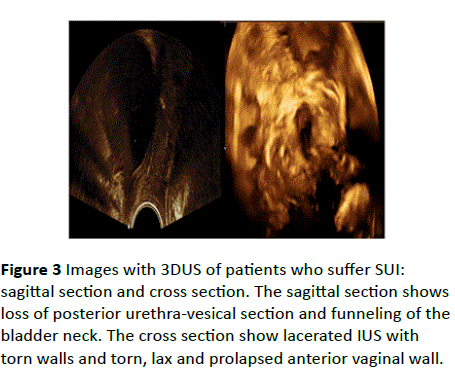
Figure 3 Images with 3DUS of patients who suffer SUI: sagittal section and cross section. The sagittal section shows loss of posterior urethra-vesical section and funneling of the bladder neck. The cross section show lacerated IUS with torn walls and torn, lax and prolapsed anterior vaginal wall.
Diagnosis
In addition to the history and examination, in the local examination, the examiner should take in consideration few new important notes. If, without asking the patient to strain, you can see the anterior vaginal wall, then there is anterior vaginal wall descent [4,5]. Normally, the anterior vaginal wall is going up and backward and not seen on inspecting the vulva. The external urethral meatus has, normally, a forward direction, if its direction is forward and upward, then there is a loss of posterior urethra-vesical angle and this patient has overactive bladder (OAB). As well, the posterior vaginal wall is going up and backward normally and is not visible at the vaginal introitus [8-11]. If, without straining the posterior vaginal wall is bulging, then there is posterior vaginal wall prolapse. The size of the perineum is to be noticed and measured [12-14].
Imaging of the pelvis, by ultrasound (US), magnetic resolution imaging (MRI) and computerized axial tomographic scanning (CAT scan) will show the urethra open with lacerated wall in cases of urinary incontinence. As well, the anal canal is open with lacerated wall in cases of FI [15].
Conclusion
Laceration of the collagen chassis of the IUS leads to its weakness and subsequent stress urinary incontinence (SUI). Redundant lax vaginal walls, due to lacerations in the collagen chassis of the vagina leads to vaginal prolapse. Similarly, lacerations of the collagen chassis of the IAS lead to its weakness and FI.
Aim of the study and the new reconstructive operation
Therefore, mending the lacerated walls of the sphincters (IUS and IAS), will strengthen them, increase the wall tension with subsequent increase of the urethral and anal canal pressure, and cure involuntary leak (SUI and FI). We can achieve strengthening of the redundant vaginal walls by overlapping the bisected vaginal flaps and this will leads also to narrowing of the patulous vagina.
Urethro-ano-vaginoplasty operation
The operation consists of an anterior and a posterior section. In the anterior section, (Figures 4 and 5) we correct the SUI and the anterior vaginal wall descent, as follow:
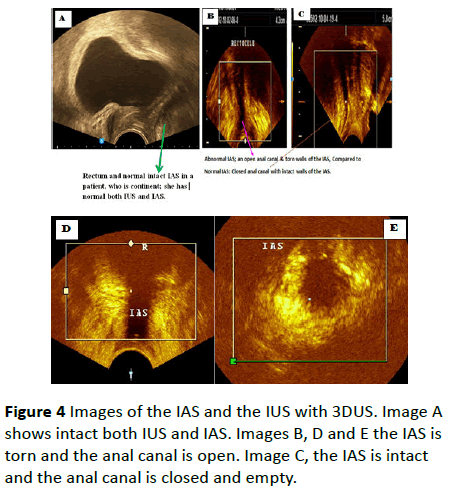
Figure 4 Images of the IAS and the IUS with 3DUS. Image A shows intact both IUS and IAS. Images B, D and E the IAS is torn and the anal canal is open. Image C, the IAS is intact and the anal canal is closed and empty.
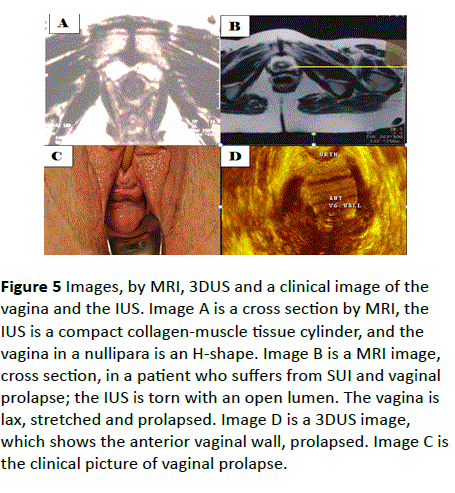
Figure 5 Images, by MRI, 3DUS and a clinical image of the vagina and the IUS. Image A is a cross section by MRI, the IUS is a compact collagen-muscle tissue cylinder, and the vagina in a nullipara is an H-shape. Image B is a MRI image, cross section, in a patient who suffers from SUI and vaginal prolapse; the IUS is torn with an open lumen. The vagina is lax, stretched and prolapsed. Image D is a 3DUS image, which shows the anterior vaginal wall, prolapsed. Image C is the clinical picture of vaginal prolapse.
1. Expose the IUS (we dissect the IUS clear from the anterior vaginal wall). The laceration in the posterior wall of the IUS will be obvious, we mend It with interrupted simple stitches with slowly absorbable suture material e.g. polyglycan (vicryl) no. one.
2. Mend the torn wall of the sphincter; this may take 5-7 simple interrupted stitches.
3. Strengthen the anterior vaginal wall by overlapping the two vaginal flaps, we do this by the innovated “pull, or dragging sutures”. We start on the left vaginal flap, far lateral, go with the needle to the near edge of the right vaginal flap, come down about 1-2 cm. then go far lateral to the left vaginal flap below the start. When we tie the suture, this will drag the right vaginal flap beneath the left one [4,5]. We repeat this suture 5-6 times, start externally and go up. We then, suture the free left vaginal edge as far lateral to the right side of the vagina. By this way; we also add extra support to the mended IUS and narrow the patulous vagina [11,16] (Figure 4).
In the posterior section we: (Figures 6 and 7).
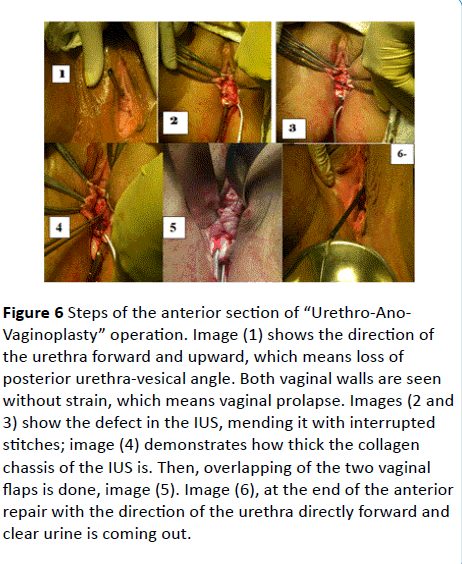
Figure 6 Steps of the anterior section of “Urethro-Ano- Vaginoplasty” operation. Image (1) shows the direction of the urethra forward and upward, which means loss of posterior urethra-vesical angle. Both vaginal walls are seen without strain, which means vaginal prolapse. Images (2 and 3) show the defect in the IUS, mending it with interrupted stitches; image (4) demonstrates how thick the collagen chassis of the IUS is. Then, overlapping of the two vaginal flaps is done, image (5). Image (6), at the end of the anterior repair with the direction of the urethra directly forward and clear urine is coming out.
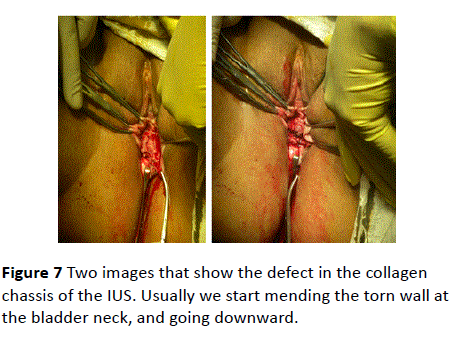
Figure 7 Two images that show the defect in the collagen chassis of the IUS. Usually we start mending the torn wall at the bladder neck, and going downward.
1. Expose the IAS (by dissecting the torn IAS clear from the posterior vaginal wall), the lacerations in the IAS will appear. Mending the torn walls of the IAS, using interrupted vicryl no one sutures.
2. Mend the torn sphincter; this may take 4-6 stitches.
3. Approximate the two-levator ani muscles.
4. Strengthen the posterior vaginal wall by overlapping the two vaginal flaps; also, we add extra support to the mended IAS and narrow the patulous vagina.
5. Repair the perineum.
Patients and methods
Since 2009, we performed the operation on five hundred and fifty patients with combined SUI, and FI, in addition to vaginal prolapse, both anterior and posterior. Their age ranged between 42 and 65 years. All had vaginal deliveries. Fifty patients had previous TVT (tension free vaginal tape) operation. Seventy of them had previous classical repair and Kelley’s plicatory sutures repair for SUI. None had surgery for FI [17-19]. All patients had their history and clinical examination. Five hundred patients had Three- dimension ultrasound (3DUS) scanning, and fifty patients have MRI. Urine analysis is done and patients with urinary infection treated according to results of culture and sensitivity test [20-22].
Urethro-ano-vaginoplasty operation
In the anterior section, we correct the SUI and the anterior vaginal wall descent through the following steps: (Figures 4 and 5).
We grasp the cervix with two pairs of cervical volsela. We inject about 10-20 ml. normal saline with adrenaline (2 per thousand concentration}, beneath the vaginal wall to act as hydro dissection and vasoconstrictor. This separates the anterior vaginal wall from the posterior wall of the IUS. We do 2-4 cm transverse incision about three cm above the external cervical os. With a pair of dissecting scissors, we separate the anterior vaginal wall from the IUS [23-26]. We cut the anterior vaginal wall longitudinally from the transverse cut we made up to the submeatal sulcus, which correspond to the perineal membrane. We grasp each vaginal flap with three pairs of Kocher’s forceps. The defect in the IUS will be apparent and on each side, we can clearly see two edges. One edge is of the anterior vaginal wall and the other is of the torn posterior wall of the IUS [27,28].
1. Expose the IUS (we free the IUS clear from the anterior vaginal wall).
2. Mend the torn posterior wall of the IUS by several (6-8) simple interrupted sutures using number 0 polyglycan thread, sutures (Figures 4 and 5).
3. Strengthen the anterior vaginal wall by overlapping the two vaginal flaps, using a novel dragging sutures, dragging the right vaginal flap underneath the left vaginal flap. Then we suture the free edge of the left vaginal flap as far lateral on the right side of the vagina. So we strengthen the anterior vaginal wall and decrease its width, we also add extra support to the mended IUS, and preserve the body’s own collagen (Figure 6).
In the posterior section, we do as in Figures 6 and 7.
We do hydro dissection between the posterior vaginal wall and the anal canal; and in the perineum as done anteriorly.
We do a V-shape incision at the line between the posterior vaginal wall and the perineal skin down to the perineum. Then we try to create a space between the posterior vaginal wall and the anal canal by sharp and blunt dissection. Next with a pair of dissecting scissors, we separate the posterior vaginal wall from the anal canal. Then we cut the posterior vaginal wall longitudinally in the midline to beyond the apex of the prolapse protrusion.
We hold each vaginal flap with three pairs of Kocher’s forceps. We will clearly see two different edges on each side, one is the vaginal edge, and the other is the anterior wall of the torn IAS [29-31] (Figure 8 and 9).
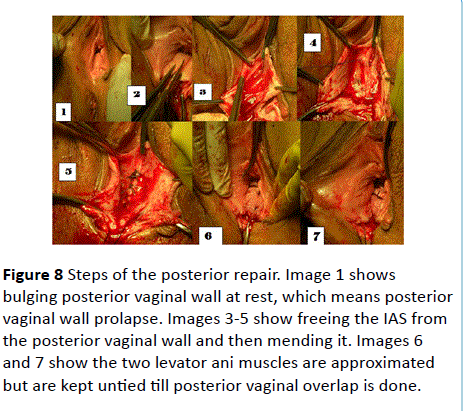
Figure 8 Steps of the posterior repair. Image 1 shows bulging posterior vaginal wall at rest, which means posteriorvaginal wall prolapse. Images 3-5 show freeing the IAS from the posterior vaginal wall and then mending it. Images 6 and 7 show the two levator ani muscles are approximated but are kept untied till posterior vaginal overlap is done.
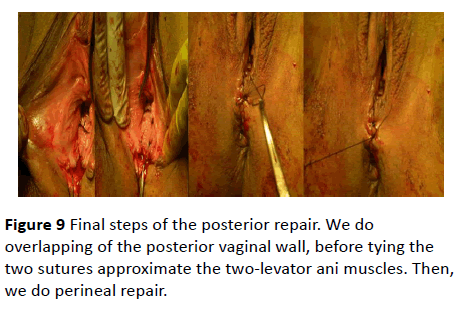
Figure 9 Final steps of the posterior repair. We do overlapping of the posterior vaginal wall, before tying the two sutures approximate the two-levator ani muscles. Then, we do perineal repair.
1. We dissect the torn IAS clear from the posterior vaginal wall.
2. Mend the torn wall of the sphincter by serial interrupted simple sutures with number one polyglcan (vicryl) thread.
3. Approximate the two-levator ani muscles by 2-3 sutures, but leave them untied until we finish repair of posterior vaginal wall.
4. Strengthen the posterior vaginal wall by overlapping the two vaginal flaps; thus, we also add extra support to the mended IAS and keeping the natural body collagen.
5. Tie the sutures that approximate the two levators ani muscles by surgical knots.
6. Repair the perineum.
7. We put a Foley’s catheter and vagina pack for 24 hours.
Results
Four hundred and fifty patients are cured and did not have any complaint soon after the operation and for more than three years follow up. Fifty patients improved significantly soon after the operation and progressively got better and cured after six to twelve months later. Fifty patients showed cure on FI but some unsatisfactory improvement on urinary leak [28,30,31].
Discussion
Traumatic lacerations of the collagen chassis of the IUS leads to urinary incontinence. When the main trauma affects the upper part of the cylinder, this, on sudden increase of abdominal pressure, allows urine to leak into the urethra, causing a desire to void, and leading to over active bladder (OAB). Mostly the trauma causes lacerations along the entire length of the IUS, which leads to mixed type of urinary incontinence. Rarely, the trauma affects mainly the lower part of the IUS, which leads to genuine SUI. Healing of the collagen may be slow and not necessary by collagen fibers, it may heal with weak fibrous tissue fibers. This may explain the failure and the slow improvement in some patients. Local estrogen application may help in the collagen repair, we tried it, and it shows success. We advised the patient to apply estrogen cream vaginally twice after removal of the vaginal pack for two to four months. The trauma, which affects the internal anal sphincter (IAS), leads to fecal incontinence (FI). The trauma is mostly childbirth trauma affecting both the posterior vaginal wall that leads to posterior vaginal wall prolapse; and the IAS with subsequent FI. In addition, anal intercourse is another traumatic factor that leads to FI. The patients show cure from FI, as well from vaginal prolapse and were quite satisfied. Narrowing the vagina by overlapping the vaginal flaps, lead to good sex life. In addition, we did not cut and remove any body tissues, and thus we spared the body’s own collagen.
Conclusion
Laceration of the collagen chassis of the IUS leads to its weakness and subsequent stress urinary incontinence (SUI). Redundant lax vaginal walls due to lacerations in the collagen chassis of the vagina leads to vaginal prolapse. Similarly, lacerations of the collagen chassis of the IAS leads to it weakness and FI. Mending the lacerations in the sphincters and strengthening the mended sphincters further by overlapping the bisected vaginal flaps will restore the normal anatomy and hence the normal physiology and continence.
References
- Abrahams H, Hutchings RT, Marks SC (1998) Human Anatomy. (4th edn), Mosby, USA, 238-245.
- Harold E(1972) Clinical Anatomy: A Revision and Applied Anatomy for Clinical Students. Blackwell Scientific Publications124-139.
- Warwick R, Peter LW (1973) Gyay’s Anatomy.(35thedn), Longman, UK, 1314-1351.
- Hemaly AKMEl, Laila AES, Mousa, Ibrahim MK, Abdul KAA (2014) Pelvic Floor Dysfunction and its Reconstructive Surgery: Novel Concepts; Createspace, an ISBN 978-1-001-04115.
- Hemaly AKMEl, Laila AM, Ibrahim MK, Al-Adwani KAA (2013) Pelvic Floor Dysfunction And Its Surgical Treatment: Novel Concepts On Pelvic Organs Dysfunction And Their Reconstructive Surgery. In:Al-Adwani KAA (ed.) Al Ahram Publication Ltd, Cairo, Egypt.
- Hemaly AKMEl, Laila M, Ibrahim K (2015) Continence. International Journal of Gynecology, Obstetrics and Neonatal Care 2: 24-29.
- Hemaly AKMEl, Laila M, Ibrahim K (2014) Continence and Incontinence: How Can You Gain Continence? ISBN 978-3-639-66683-0, Scholars press.
- Hemaly AKMEl, Laila AES, Mousa, Ibrahim MK, Khaled AS, (2014) Imaging of the Pelvic Floor. Current Medical Imaging Reviews 10: 205-214.
- Hemaly AKMEl, Mousa LAS, Kandil IM (2014) Micturition and Urinary Incontinence, Journal of Nephrology and Urology Research 2: 19-26.
- Hemaly AKMEl, Mousa LA, Kurjak A, Kandil IM, Serour AG (2013) Pelvic Floor Dysfunction, the Role of Imaging and Reconstructive Surgery, Donald School Journal of Ultrasound in Obstetrics and Gynecology7:86-97.
- Hemaly AKMEl, Laila AM, Ibrahim MK, Sayed MSAI, Mohammed AZ, et al. (2014) A Novel Concept on the Patho-Physiology of Defecation and Fecal Incontinence (FI) in Women-Moreover, Its Reconstructive Surgery; Anthony G. Catto-Smith, ed: FECAL INCOTINENCE Causes, Management AND OUTME. INTECH Publication, Croatia 47-67.
- Hemaly AKMEl, Ibrahim MK, Asim K, Laila ASM, Hossam HK, at al. (2011) Ultrasonic Assessment of the Urethra and the Vagina in Normal Continent Women and Women Suffering from Stress Urinary Incontinence and Vaginal Prolapse. Donald School Journal of Ultrasound in Obstetrics and Gynecology 5: 330-38.
- Hemaly AKMEl, Ibrahim MK, Asim K, Laila ASM, Hossam HK, et al. (2011) Ultrasound Assessment of the Internal Anal Sphincter in Women with Fecal Incontinence and Posterior Vaginal Wall Prolapse (Rectocele). Donald School Journal of Ultrasound in Obstetrics and Gynecology 5: 330-42.
- Hemaly AKMEl, Ibrahim MK, Asim K, Ahmad GS, Laila ASM, et al. (2009) Imaging the Internal Urethral Sphincter and the Vagina in Normal Women and Women Suffering from Stress Urinary Incontinence and Vaginal Prolapse. Gynaecologia Et Perinatologia 18: 169-286.
- Hemaly AKMEl, Laila ASM, Ibrahim MK, Fatma SElS, Ahmad GS, at al. (2010) Fecal Incontinence, A Novel Concept: The Role of the internal Anal sphincter (IAS) in defecation and fecal incontinence. Gynaecologia Et Perinatologia19: 79-85.
- Hemaly AKMEl, Laila ASM, Ibrahim MK, Fatma SElS, Ahmad GS, et al. (2010) Surgical Treatment of Stress Urinary Incontinence, Fecal Incontinence and Vaginal Prolapse By A Novel Operation "Urethro-Ano-Vaginoplasty" Gynaecologia Et Perinatologia19: 129-188.
- de Boer TA, Salvatore S, Cardozo L, Chapple C, Kelleher C, et al. (2010) Pelvic organ prolapse and overactive bladder. Neurourol Urodyn 29: 30-39.
- https://www.obgyn.net/urogynecology/urethro-vaginoplasty.
- https://www.obgyn.net/urogynecology/urethro-raphy-new-technique-surgical-management-stress-urinary-incontinence
- https://www.obgyn.net/incontinence/urethro-raphy
- https://www.obgyn.net/urogynecology/menopause-voiding-troubles.
- El Hemaly AK, Mousa LA (1996) Micturition and urinary continence. Int J Gynaecol Obstet 52: 291-292.
- https://www.obgyn.net/urogynecology/urinary-incontinence-gynecology-review-article.
- El Hemaly AK (1998) Nocturnal enuresis: pathogenesis and treatment. Int Urogynecol J Pelvic Floor Dysfunct 9: 129-131.
- El Hemaly AK, Mousa LA (1996) Stress urinary incontinence, a new concept. Eur J Obstet Gynecol Reprod Biol 68: 129-135.
- https://www.obgyn.net/urogynecology/stress-urinary-incontinence-sui-facts-and-fiction
- Hemaly AKMEl, Nabil AM, Laila AM, Ibrahim MK, Asem A, et al. Evidence based Facts on the Pathogenesis and Management of SUI.
- https://www.obgyn.net/urogynecology/urethro-plasty-novel-operation-based-new-concept
- Ibrahim MK, Hemaly AKMEl, Mohamad MR (2003) Ultrasonic Assessment of the Internal Urethral Sphincter in Stress Urinary Incontinence. The Internet Journal of Gynecology and Obstetrics 2(1).
- https://www.obgyn.net/urogynecology/nocturnal-enuresis-novel-concept-its-pathogenesis-and-treatment
- https://www.obgyn.net/urogynecology/nocturnal-enuresis-update-pathogenesis-and-treatment

