Keywords
Adenocarcinoma; Pancreas; Recurrence; Survival
Abbreviation
CT computed tomography; ERCP endoscopic retrograde cholangiopancreatography; EUS endoscopic ultrasound; FDG-PET fluorodeoxyglucose positron emission tomography; PDAC pancreatic ductal adenocarcinoma; NA neoadjuvant
INTRODUCTION
Pancreatic ductal adenocarcinoma is currently the fourth leading cause of cancer death worldwide [1, 2]. Despite improvements in surgical technique, perioperative care, systemic treatment and follow-up methodology, PDAC continues to have dismal 5-year survival of only 5% with a reported median survival of 6 months [3, 4, 5, 6]. Surgical resection is still considered the only potentially curative treatment modality in selected patients. However, the vast majority of patients with resected PDAC either recur locally or have distant metastases within two years [7, 8, 9, 10].
Over the last two decades, multiple studies have explored clinicopathological variables that may help identify patients who are more likely to have a recurrence of PDAC following surgery [11, 12, 13, 14]. However, the timeline to recurrence and the different patterns of local vs. organ-specific recurrence based on clinicopathological variables has not been well characterized. A recent study by Groot et al. provided some insight but excluded patients who received neoadjuvant (NA) chemotherapy [10]. Unfortunately, this excludes a significant cohort of patients with borderline resectable disease who would normally be recommended NA chemotherapy or chemo-radiotherapy at high-volume centers [15].
This study aims to investigate 1) the timeline and pattern of recurrence for all patients following surgical resection of PDAC and 2) the impact of the site of recurrence on survival.
METHODS
Study Population
Patients undergoing pancreatic resection for nonmetastatic histopathologically confirmed PDAC at Royal North Shore Hospital and North Shore Private Hospital (Sydney, NSW, Australia) between January 2011 and December 2015 were identified from a prospectively maintained database. All patients were assessed at a multidisciplinary meeting and received routine preoperative workup including: triple phase computed tomography (CT) of the abdomen and pelvis; CT chest; endoscopic ultrasound (EUS) or endoscopic retrograde cholangiopancreatography (ERCP) for cytology; and a staging laparoscopy. Patients with distant lesions equivocal for metastatic spread on CT imaging underwent a 18-fluorodeoxyglucose positron emission tomography (FDG-PET) scan. Distant FDG-avid lesions were subsequently biopsied. In patients with non-metastatic disease, pancreatic resection was performed according to previously described methods [16, 17, 18]. Patients with non-PDAC periampullary lesions (e.g. ampullary adenocarcinoma, distal cholangiocarcinoma, duodenal cancer, neuroendocrine tumors, cystic neoplasms) were excluded from analysis. Patients with incomplete followup data were also excluded. The final cohort of patients who underwent curative-intent pancreatic resection for PDAC was retrospectively analyzed.
Demographic and Clinicopathological Characteristics
Patient demographics and pathological variables were obtained from the departmental database. Details regarding the use of NA and/or adjuvant therapy were recorded. Patients with borderline resectable disease according to the 2016 Australasian Gastrointestinal Trials Group Guidelines [19] were referred for NA therapy administered according to the recommendation of the multidisciplinary team. NA therapy included six months of perioperative chemotherapy (gemcitabine only, gemcitabine and nab-paclitaxel, or FOLFIRINOX) with/ without NA radiotherapy. The following pathological variables were analyzed: tumor size, resection margin status, lymphovascular and perineural invasion, and lymph node status. The largest diameter of resected specimen was taken as the tumor size. The location of the nearest margin was recorded as follows: portal vein bed, periuncinate soft tissue, pancreatic neck, anterior pancreatic capsule and posterior surface. An R1 resection was classified as a resection margin of ≤ 1 mm according to the standardized protocol for PDAC histology reporting [20]. The presence or absence of small vessel invasion, large vessel invasion and perineural invasion was identified. Classification of small and large vessel invasion was based on the ‘Structured Reporting Protocol’ by the Royal College of Pathology of Australasia [21]. Absolute lymph node count was determined from the resected specimen, and the lymph node ratio was calculated as the number of lymph nodes involved by tumor divided by the total number of resected lymph nodes. Overall survival was defined as a period from the date of surgery to the date of death.
Follow-up and PDAC Recurrence
Patients were followed up in an outpatient setting by the multidisciplinary team including surgeons, medical oncologists, and radiation oncologists. Follow-up evaluation included history, physical examination every three to six months for the first two years monitoring serum cancer-associated antigen 19-9 (CA 19-9) levels and CT scans of the chest, abdomen and pelvis. In the absence of recurrent disease after two years, patients were followed up annually. Follow up data collection concluded on January 17 2017. Disease recurrence was determined by evidence of a malignant appearing lesion on CT with histological/cytological confirmation or an 18- FDG-avid lesion on FDG-PET scan. A local recurrence was defined as the development of recurrent malignant disease within the pancreatic bed or regional lymph nodes. Distant recurrence was defined as a metastatic PDAC lesion developing outside of the pancreatic bed or regional lymph nodes, including the liver, lung, peritoneum, bone and abdominal wall. Multiple recurrence was defined as the simultaneous diagnosis of recurrent PDAC occurring in more than one body site, whether local or distant.
Ethics
This study was approved by the Northern Sydney Local Health District and North Shore Private Hospital Ethics Committees (Study numbers HREC/16/HAWKE/105 and NSPHEC 2016-007).
Statistical Analysis
Survival analysis was performed using the Kaplan- Meier method, and differences in survival were compared using the log-rank test. A Cox regression analysis was performed to identify factors independently associated with recurrence. A p-value of <0.05 was considered to be statistically significant.
RESULTS
Demographics
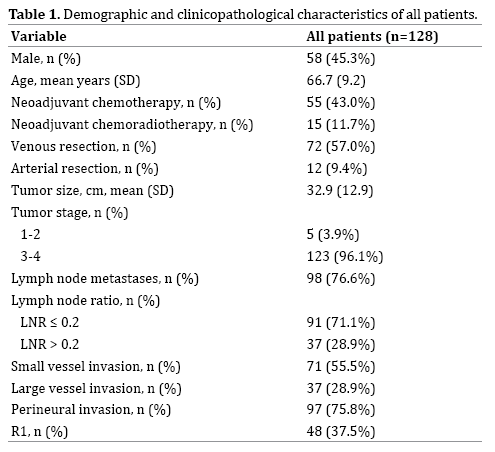
A total of 128 patients with histologically diagnosed PDAC underwent surgical resection in the study period. Seventy (55%) patients were female. The median age at the time of operation was 68 (IQR 60-73). Resection type was pancreaticoduodenectomy in 115 (89.8%), distal pancreatectomy in eight (6.3%) and total pancreatectomy in five patients (3.9%). Seventy patients (54.7%) received NA therapy of which 55 (42.9%) received NA chemotherapy and 15 (11.7%) received NA chemoradiotherapy. Of those who received NA chemotherapy, 37 patients developed disease recurrence. Eight patients who had NA chemoradiotherapy developed disease recurrence. The demographic and clinicopathological characteristics are summarized in Table 1. The median follow-up for all patients was 15.5 months (IQR 9-25.25 months). Disease recurrence was observed in a total of 82 (64%) patients (Table 1).
Factors Associated with Recurrence
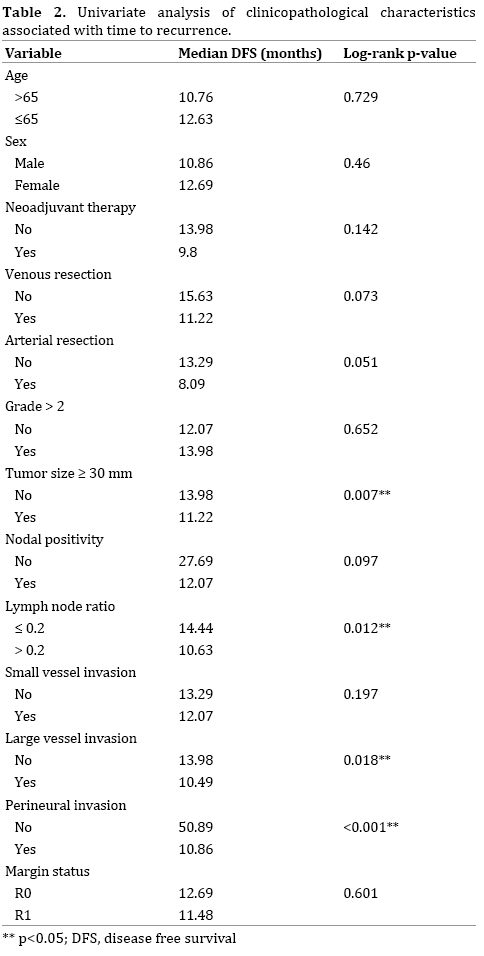
Univariate analysis of clinicopathological characteristics associated with time to recurrence is detailed in Table 2. Factors significantly associated with shorter median diseasefree survival (DFS) on this analysis included: tumor size ≥ 30 mm, lymph node ratio >0.2, large vessel invasion, and perineural invasion. Patients requiring a venous or arterial resection were associated with a non-significant trend towards shorter disease free survival (DFS).
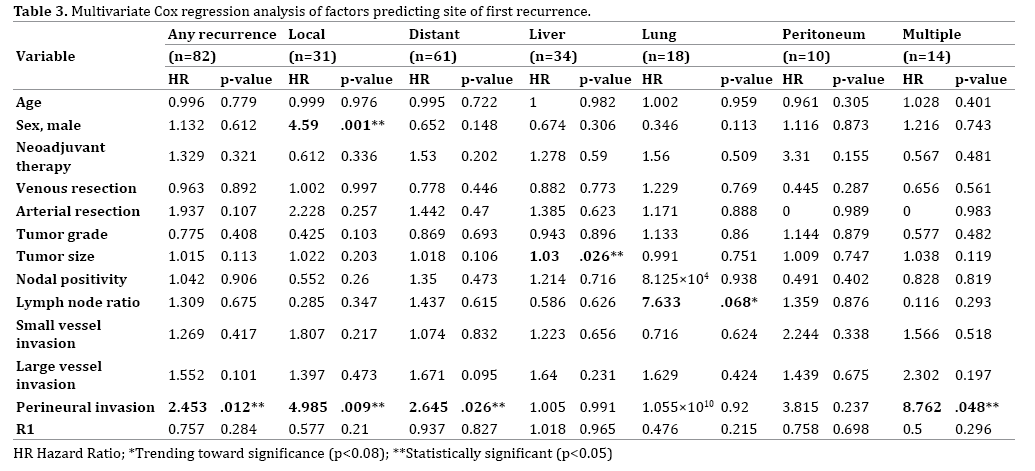
Multivariate Cox regression analysis was performed to identify independent predictors of disease recurrence (Table 3). Perineural invasion was identified as a significant independent predictor of early disease recurrence at any site (HR 2.43, p=0.012).
Site of Recurrence
Clinicopathological characteristics associated with the site of first recurrence of PDAC are shown on Table 3. Thirty-one patients (24.2%) developed a local recurrence, and 61 patients (47.7%) developed a distant metastatic recurrence. Thirty-four patients (26.6%) developed liver metastases, 18 (14.0%) developed lung metastases, and 10 (7.8%) developed peritoneal metastases. Fourteen patients (10.9%) developed recurrence in multiple body sites simultaneously.
Of the patients who developed multiple recurrences, the majority of patients (n=10/14) developed local recurrence with one other site of distant metastasis. When discovered simultaneously with other sites of recurrent disease, liver metastases were found most often in combination with local recurrences (n=6/10) followed by peritoneal lesions (n=3/10).
On Cox regression analysis, factors significantly predictive of the development of local recurrence included male gender (HR 4.590, p=0.001) and the presence of perineural invasion (HR 4.985, p=0.009). Perineural invasion was the only factor independently associated with the development of distant recurrence (HR 2.645, p=0.026). Increasing tumor size was significantly predictive of the development of liver recurrence (HR 1.030, p=0.026). An increase in lymph node ratio was associated with a trend toward an association with the development of lung metastases (HR 7.633, p=0.068). There were no factors predictive of the development of peritoneal recurrence. Perineural invasion was also significantly associated with the development of multiple simultaneous recurrences (HR 8.762, p=0.048).
Disease Recurrence and Survival
The median overall survival (OS) for the entire cohort was 26.2 months (IQR 12.6 – 57.4 months). Median OS was significantly longer in patients without recurrence as compared with those who did experience recurrence of disease (53.5 vs. 20.1months, log-rank p<0.001). Survival curves are presented in Figure 1a.
Figure 1a. Kaplan-Meier sur vival curve demonstrating overall survival of disease recurrence group vs. non-recurrence group. Log-rank p<0.0001.
The median disease free survival was 12.1 months (IQR 7.3 - 36.5 months). There was a significant difference in median time to recurrence depending on the site of first recurrence (Figure 1b). Median time to recurrence according to site of recurrence were: peritoneal, 2.7 months (IQR 1.6-3.5 months); multiple sites, 6.7 months (IQR 5.1- 14.4 months); liver, 7 months (IQR 4.1-11.8 months); local, 10.4 months (IQR 7.8-12.7 months); and lung, 11.5 months (IQR 7.9-30.1 months, log-rank p=0.001) (Figure 1b). The combined timeline to recurrence is represented in Figure 2.
Figure 1b. Kaplan-Meier survival curve of overall survival by the site of recurrence from the date of recurrence. For clarity of the figure, the curve for the “other” recurrence group has been omitted.
Figure 2. Timeline to recurrence by site from the date of operation. The median and interquartile range in months is represented within the horizontal bar graph. For clarity of the figure, the “other” recurrence group has been omitted.
Median survival with recurrent disease (date of recurrence to date of death/censor) was 7.8 months (IQR 3.7-18.5 months). There was a significant difference in median survival with recurrent disease depending on the site of recurrence. Median survival periods with recurrent disease according to site of recurrence were: peritoneal, 2.8 months (IQR 2.1-4.1 months); multiple sites, 3.9 months (IQR 2.8-5.2 months); liver, 7.6 months (IQR 3.8-18.5 months); local, 11.4 months (IQR 6.3-30.9 months); lung, 12.9 months (IQR 6.1-30.4 months, log-rank p=0.007).
DISCUSSION
The current study reviewed the pattern and site of recurrence in resected PDAC patients including those who received NA therapy and identified clinicopathological predictors of recurrence. On univariate analysis, larger tumor size, large vessel invasion, higher lymph node ratio and perineural invasion were significantly associated with shorter DFS. On multivariate Cox regression analysis, perineural invasion was independently associated with shorter DFS. This is in keeping with Ozaki et al. [22] and Lewis et al. [23]. Several clinicopathological factors were identified as independent risk factors for the development of recurrence in particular sites of the body. Notably, male gender was significantly associated with the development of local recurrence, and perineural invasion was significantly associated with the development of local, distant, and multiple recurrences. This study also demonstrated significantly different survival durations in the presence of recurrence depending upon the location of recurrence. Patients with peritoneal recurrence had the shortest median survival in the presence of recurrence, and those with local or lung recurrence survived the longest duration.
The present study largely confirms the findings of previously published studies examining similar variables and outcomes. A large tumor size and a greater lymph node burden increase the risk of disease recurrence and poorer survival [10, 24, 25, 26, 27]. The distribution and timing of sites of recurrence in the present study are very similar to those reported by Groot et al.
Contrary to some published reports, the present study does not demonstrate a significant relationship between R1 resection and the risk of local recurrence [24, 25, 26]. Van de Broek et al. [11] and Groot et al. [10] showed a significant reduction in survival in patients with R1 resection and increased local recurrence rates. However, our findings are in agreement with Nitta et al. who reported that there was no increase in the local recurrence rates in R1 resections [28]. The figures in the present study may be attributed to high rates of NA as well as adjuvant chemotherapy which has been shown to decrease local recurrence rates significantly [29, 30].
There was a distinct survival pattern for individual sites of recurrence in our series. The current study has demonstrated significantly longer disease-free survival and overall better prognosis in patients who developed solitary lung recurrences as the first site of recurrence. This is in contrast to patients with liver, peritoneal and multiple sites of recurrence who had shorter disease-free survival and shorter overall survival (Figure 1b). Recent studies [3, 9, 31] have also observed a similar pattern of better prognosis among patients who developed solitary lung recurrences after PDAC resection [10]. Whether the pattern of recurrence in PDAC reflects a particular pattern of gene expression remains to be elucidated. Campbell et al. have demonstrated particular PDAC genotypes can drive metastases to particular organs, which may explain organ-specific metastases [32]. Identification of genomic, proteomic, and/or metabolomic signatures predicting individual patterns of recurrence may significantly influence early recognition and tailored therapy.
The significant differences demonstrated in the timing of recurrence depending on the site of recurrence may have implications on the way that patients are surveyed post-operatively. The data from the present study suggest that the highest risk for peritoneal recurrence is within the first three months, whereas local and lung recurrence occur much later. Practically, this implies that the clinician should remain vigilant for the development of peritoneal recurrence particularly in the early follow-up period. Rising serum Ca19-9 levels in the absence of visible recurrence on CT imaging should prompt an 18-FDG-PET scan to look for peritoneal disease.
The identification of particular factors associated with patterns of recurrence also carries clinical implications. Patients with perineural invasion in particular may warrant a more intensive follow-up schedule. From the data in the present study, it is unclear why males should be more likely to develop local recurrence. Further work is required to determine whether this relates to unknown factors that were not included in the multivariate model e.g. compliance with systemic therapy or genetic/epigenetic phenomena.
This current study included patients who underwent NA therapy prior to resection. It is understood that NA therapy controls local disease and is thereby able to downstage patients with locally advanced PDAC to resectable criteria [27, 33]. This ultimately influences prognosis by providing an opportunity for surgical resection which is the only significant treatment known to have a chance of cure. In the literature, it has been suggested that NA therapy substantially lowers the rate of local recurrence following resection [30, 34, 35].
Currently, most patients with disease recurrence are managed with cytotoxic chemotherapy regardless of the site of recurrence. Whilst this may be appropriate for patients with evidence of widespread disease, locoregional or organ-specific therapies may be suitable for patients with single site disease. Examples of such therapies include radiofrequency ablation, transarterial chemoembolization (TACE) and SIR-Spheres for liveronly disease, and radiotherapy for local recurrence [36, 37]. Surgical resection of isolated metastases has also been recently reported with inconsistent reports of survival benefit [38, 39]. Given the paucity of highquality data to guide such management decisions, further research in the form of randomized trials are required to clarify the efficacy of these locoregional management strategies.
There were several limitations to our study. While the cohort size was small, the follow-up was very close thereby capturing the majority of patients as opposed to other studies where only a small percentage of the cohort could be included for analysis [10]. A longer follow-up period may have captured future recurrences for some patients which may take longer to develop such as lung recurrences. The current study did not include quality of life data, which should be the focus of future pancreatic cancer research. The inclusion of how the disease recurrence and the subsequent treatment affects the patients' and their family's quality of life is important to enable more comprehensive end of life care.
CONCLUSION
The rate of PDAC recurrence following curative resection remains high. There are distinctive patterns of recurrence by the site which inevitably also affects survival. Further research is now needed to investigate possible tumor cell and or stroma specific biomarkers which may help predict these patterns of disease recurrence. Such research will be critical for personalizing cancer therapy for the PDAC patient.
Conflict of Interest
We declare that we have no conflict of interests.
References
- American Cancer Society. Cancer Facts & Figures 2013. Atlanta: American Cancer Society.
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 2011; 61:212-236. [PMID: 21685461].
- Wolfgang CL, Herman JM, Laheru DA, Klein AP, Erdek MA, Fishman EK,, et al. Recent progress in pancreatic cancer. CA Cancer J Clin 2013; 63:318–348. [PMID: 23856911].
- Winter JM, Brennan MF, Tang LH, D'angelica MI, Dematteo RP, Fong Y, et al. Survival after resection of pancreatic adenocarcinoma: results from a single institution over three decades. Ann Surg Oncol 2012; 19:169–175. [PMID: 21761104].
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10–15. [PMID: 16794383].
- Katz MH, Wang H, Fleming JB, Sun CC, Hwang RF, Wolff RA, et al. Long-term survival after multidisciplinary management of resected pancreatic adenocarcinoma. Ann Surg Oncol 2009; 16:836–847. [PMID: 16794383].
- Kleeff J, Reiser C, Hinz U, Bachmann J, Debus J, Jaeger D, et al. Surgery for recurrent pancreatic ductal adenocarcinoma. Ann Surg 2007; 245:566–572. [PMID: 17414605].
- Hernandez JM, Morton CA, Al-Saadi S, Villadolid D, Cooper J, Bowers C, et al. The natural history of resected pancreatic cancer without adjuvant chemotherapy. Am Surg 2010; 76:480–485. [PMID: 20506876].
- Herman JM, Swartz MJ, Hsu CC, Winter J, Pawlik T, Sugar E, et al. Analysis of fluorouracil-based adjuvant chemotherapy and radiation after pancreaticoduodenectomy for ductal adenocarcinoma of the pancreas: results of a large, prospectively collected database at the Johns Hopkins Hospital. J Clin Oncol 2008; 26:3503–3510. [PMID: 18640931].
- Groot VP, Rezaee N, Wu W, Cameron JL, Fishman EK, Hruban RH, et al. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann Surg. In press 2017. [PMID: 28338509].
- Van Den Broeck A, Sergeant G, Ectors E, Van Steenbergen W, Aerts R, Topal B. Patterns of recurrence after curative resection of pancreatic ductal adenocarcinoma. Eur J Surg Oncol 2009; 35:600–604. [PMID: 19131205].
- Shibata K, Matsumoto T, Yada K, Sasaki A, Masayuki O, Kitano S. Factors predicting recurrence after resection of pancreatic ductal carcinoma. Pancreas 2005; 31:69–73. [PMID: 15968250].
- Hernandez JM, Morton CA, Al-Saadi S, Villadolid D, Cooper J, Bowers C. The natural history of resected pancreatic cancer without adjuvant chemotherapy. Am Surg 2010; 76:480-485. [PMID: 20506876].
- Suenaga M, Fujii T, Kanda M, Takami H, Okumura N, Inokawa Y, et al. Pattern of first recurrent lesions in pancreatic cancer: hepatic relapse is associated with dismal prognosis and portal vein invasion. Hepatogastroenterology 2014; 61:1756 – 1761. [PMID: 25436375].
- Assifi MM, Lu X, Eibl G, Reber HA, Hines OJ. Neoadjuvant therapy in pancreatic adenocarcinoma: a meta-analysis of phase II trials. Surgery 2011; 150:466-473. [PMID: 21878232].
- Gundara J, Wang F, Alvarado-Bachmann R, Williams N, Choi J, Gananadha S, et al. The clinical impact of early complete pancreatic head devascularisation during pancreatoduodenectomy. Am J Surg 2013; 206:518-525. [PMID: 23809671].
- De Reuver P, Mittal A, Neale M, Gill A, Samra J. Extended pancreatoduodenectomy as defined by the International Study Group for Pancreatic Surgery is associated with worse survival but not with increased morbidity. Surgery 2015; 158:183-190. [PMID: 25920909].
- Kleeff J, Diener M, Z’Graggen K, Hinz U, Wagner M, Bachmann J, et al. Distal pancreatectomy: risk factors for surgical failure in 302 consecutive cases. Annals of Surgery 2007; 245:573-582. [PMID: 17414606].
- Williamson SG, Barbour A, Samra J, Haghighi K, Nikfarjam M, Kench W. Definition of surgical standards for pancreatic cancer: A Consensus statement by the Australasian Gastro-Intestinal Trials Group. 2016.
- Verbeke CS, Leitch D, Menon KV, Mcmahon MJ, Guillou PJ, Anthoney A. Redefining the R1 resection in pancreatic cancer. Br J Surg 2006; 93:1232-1237. [PMID: 16804874].
- Royal College of Pathology of Australasia. Cancer of the Exocrine Pancreas, Ampulla of Vater and Distal Common Bile Duct Structured Reporting Protocol, 1st Edition. 2014.
- Ozaki H, Hiraoka T, Mizumoto R, Matsuno S, Matsumoto Y, Nakayama T, et al. The prognostic significance of lymph node metastasis and intrapancreaticperineural invasion in pancreatic cancer after curative resection. Surg Today 1999; 29:16-22. [PMID: 9934826].
- Lews R, Drebin J, Callery M, Fraker D, Kent T, Gates J, et al. A contemporary analysis of survival for resected pancreatic ductal adenocarcinoma. HPB 2013; 15: 49-60. [PMID: 23216779].
- Fortner JG, Klimstra DS, Senie RT, Maclean BJ. Tumor size is the primary prognosticator for pancreatic cancer after regional pancreatectomy. Ann Surg 1996; 222:147-153. [PMID: 8597508].
- Griffin JF, Smalley SR, Jewell W, Paradelo JC, Reymond RD, Hassanein RE, et al. Patterns of failure after curative resection of pancreatic carcinoma. Cancer 1990; 66:56–61. [PMID: 2354408].
- Barugola, G, Falconi, M, Bettini, R, Boninsegna, L, Casarotto A, Salvia R, et al.The determinant factors of recurrence following resection for ductal pancreatic cancer. JOP 2007; 8:132–140. [PMID: 17228145].
- Takahashi S, Ogata Y, Miyazaki H, Maeda D, Murai S, Yamataka K, et al. Aggressive surgery for pancreatic duct cell cancer: feasibility, validity, limitations. World J Surg 1995; 19:653–659. [PMID: 7676716].
- Nitta T, Nakamura T, Mitsuhashi T, Asano T, Okamura K, Tsuchikawa T, et al. The impact of margin status determined by the one-millimeter rule on tumor recurrence and survival following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. Surg Today 2017; 47:490-497. [PMID: 27677294] .
- Whittington R, Bryer MP, Haller DG, Solin LJ, Rosato EF. Adjuvant therapy of resected adenocarcinoma of the pancreas. Int J Radiat Oncol Biol Phys 1991; 21:1137-1143. [PMID: 1938511] .
- Spitz FR, Abbruzzese JL, Lee JE, Pisters PW, Lowy AM, Fenoglio CJ, et al. Preoperative and postoperative chemoradiation strategies in patients treated with pancreaticoduodenectomy for adenocarcinoma of the pancreas. J Clin Oncol 1997; 15:928–937. [PMID: 9060530].
- Sperti C, Pasquali C, Piccoli A, Pedrazzoli S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 1997; 21:195–200. [PMID: 8995078].
- Campbell PJ, Yachida S, Mudie LJ, Stephens PJ, Pleasance ED, Stebbings LA, et al. The patterns and dynamics of genomic instability in metastatic pancreatic cancer. Nature 2010; 467:1109-1113. [PMID: 20981101].
- Townend P, De Reuver PR, Chua TC, Mittal A, Clark SJ, Pavlakis N, et al. Histopathological tumour viability after neoadjuvant chemotherapy influences survival in resected pancreatic cancer: analysis of early outcome data. ANZ J Surg. In press 2017. [PMID: 28318082].
- Massucco P, Capussotti L, Magnino A, Sperti E, Gatti M, Muratore A, et al. Pancreatic resections after chemoradiotherapy for locally advanced ductal adenocarcinoma: analysis of perioperative outcome and survival. Ann Surg Oncol 2006; 13:1201–1208. [PMID: 16955382].
- Greer SE, Pipas J, Sutton JE, Zaki BI, Tsapakos M, Colacchio TA, et al. Effect of Neoadjuvant Therapy on Local Recurrence after Resection of Pancreatic Adenocarcinoma. J Am Coll Surg 2008; 206:451-457. [PMID: 18308215].
- Sun JH, Zhou TY, Zhang YL, Zhou GH, Nie CH, Zhu TY, et al. Efficacy of transcatheter arterial chemoembolization for liver metastases arising from pancreatic cancer. Oncotarget. 2017 Jun 13;8:39746-39755. [PMID: 28099930].
- Gibbs P, Do C, Lipton L, Cade DN, Tapner MJ, Price D, et al. Phase II trial of selective internal radiation therapy and systemic chemotherapy for liver-predominant metastases from pancreatic adenocarcinoma. BMC Cancer 2015; 25:802. [PMID: 26503593] .
- Gleisner AL, Assumpcao L, Cameron JL, Wolfgang CL, Choti MA, Herman JM, et al. Is resection of periampullary or pancreatic adenocarcinoma with synchronous hepatic metastasis justified? Cancer 2007; 110:2484-2492. [PMID: 17941009].
- Antoniou, E, Margonis, GA, Sasaki, K, Andreatos, N, Polychronidis G, Pawlik TM, et al.Is resection of pancreatic adenocarcinoma with synchronous hepatic metastasis justified? A review of current literature. ANZ J Surg 2016; 86:973-977. [PMID: 27580713].




