Keywords
Drug Therapy; gemcitabine; Genes, BRCA1; Genes, BRCA2; Mutation; PALB2 protein, human; Pancreatic Neoplasms; Poly(ADPribose) Polymerases
Abbreviations
PARPi, poly (ADP-ribose) polymerase inhibitor; RECIST, Response Evaluation Criteria in Solid Tumors
Introduction
American Cancer Society estimates that more than 46000 people will be diagnosed with pancreatic cancer in 2014, 85% of which will die of pancreatic cancer. The incidence rates have slowly been increasing for the past 10 years with a 1.3% lifetime risk of developing pancreatic cancer [1]. There is a significant genetic component contributing to the risk of developing pancreatic cancer with hereditary cancers being 2% of total pancreatic cancers. The genetic mutation most commonly involves the tumor suppressor genes, BRCA1 and BRCA2, with their incidence varying between 5-10% [2-4]. BRCA2 mutation carriers have a 3.5-fold risk of developing pancreatic cancer [5, 6]. Women with BRCA 1/2 mutation have been shown to have a 2.4 fold increase in incidence of pancreatic cancer [7].
The BRCA1 and BRCA2 genes encode large proteins that coordinate the homologous recombination repair double strand breaks (DSBs) pathway. Poly-ADP ribose polymerases (PARP) are a family of nuclear enzymes that regulates the repair of DNA single-strand breaks (SSBs) through the base-excision repair (BER) pathway. In the presence of BRCA mutation, the BER rescue pathway for DNA repair not affected and thus can be utilized for DNA repair [8-10]. Synthetic lethality is a concept ofcellular condition in which simultaneous loss of two nonessential mutations results in cell death, which does not occur if either gene products is present and functional [11]. Using the same principle, inhibitors of PARP (PARPi) can be used to target tumor cells in patients with BRCA1/2-mutated tumors who cannot utilize homologous recombination to repair DSBs, to shut down their BER rescue pathway thus leading to accumulation of DNA damage, genomic instability and cell death (Figure 1) [12].
Figure 1. Schematic representation of PARP and BRCA mediated DNA repair in cells without exposure to PARP inhibitor and BRCA mutation (A), and
synthetic lethality in cells with BRCA mutation exposing to PARP inhibitor (B) [12].
What We Knew Before 2014 ASCO Annual Meeting?
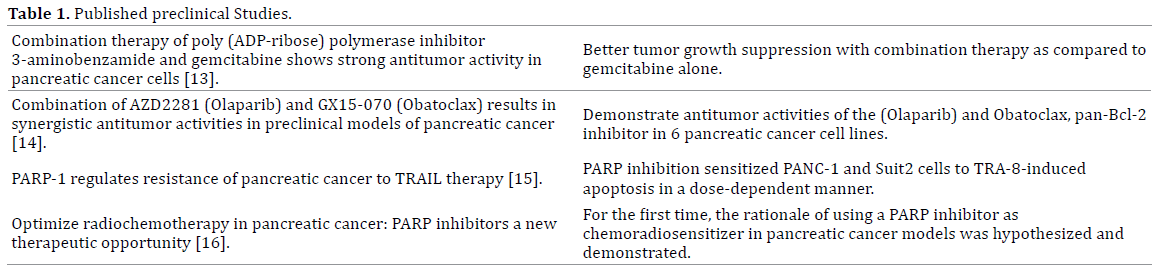
There has been a considerable interest in recent years on evaluation of therapies for pancreatic cancers associated with BRCA-mutations. Data from limited preclinical (Table 1), clinical (Table 2) studies and abstracts published at 2013 ASCO meeting (Table 3) has demonstrated that PARPi are efficacious.


What Have We Learned from the 2014 ASCO Annual Meeting?
Combination of Cisplatin, Gemcitabine, and Veliparibin Patients with Known or Potential BRCA or PALB2-Mutated Pancreas Adenocarcinoma
O’Really et al. presented the results of their Phase 1B study to assess the toxicity and recommend dose of Veliparib for phase II studies in combination with a fixed dose of Gemcitabine and Cisplatin in patients with pancreatic adenocarcinoma with BRCA and PALB2 mutations [21]. In addition, primary endpoints also included safety. Secondary end points assessed response rate by RECIST 1.1, duration of response, progression-free and overall survival and evaluated the sensitivity and resistance to the regimen.
17 patients were enrolled between 02/2012 and 10/2013, out of which 53% had BRCA mutations. All patients received a fixed dose of platinum based therapy with increasing doses of Velirapib. 56% of the BRCA mut positive patients had partial responses to the treatment and the rest had stable disease. Fatigue and hematologic side effects including anemia, neutropenia, and thrombocytopenia were the major dose limiting toxicities noted at 80 mg bid continuous (21 day) dosing regimen. Thus, they concluded that the recommended dose for phase 2 study (RP2D) for Velirapib should be 80 mg bid 1-12 days q3 weeks along with fixed dose of platinum based therapy and has shown evidence of high activity in BRCA mutated PC. This would form the basis of a randomized phase II trial currently enrolling patients with valuating the abovementioned regimen in patients with BRCA/PALB2 mutated pancreatic cancer.
Rucaparib in Patients with Pancreatic Cancer and a Known Deleterious BRCA Mutation
Domchek et al. presented the design of a Phase II study addressing the use of rucaparib, an oral PARPi, in patients with pancreatic ductal adenocarcinoma associated with a BRCA mutation [22]. It’s a single arm study where continuous rucaparib will be given to patients with BRCA mutation associated pancreatic carcinoma who have had a relapse with at least 1 but not more than 2 treatment regimens or are intolerant to chemotherapy along with no response evident on imaging. They will assess safety every 2-4 weeks, disease progression with CT scans and CA 19-9 every 4-8 weeks and survival every 4 weeks after disease progression. Primary endpoint will be RECIST1.1 response rate. Secondary endpoints will be duration of response, progression free survival, overall survival and safety. DNA analysis and gene sequencing will also be done. The trial is currently enrolling patients. NCT02042378.
Evaluation of PARP Inhibition as a Platinum Sparing Strategy in Brca2-Deficient Pancreatic Tumors
Another abstract presented at ASCO 2014 meeting was a preclinical study which assessed the efficacy of Cisplatin in combination with Olaparib (oral PARPi), Cisplatin with a non-active vehicle, Olaparib alone or vehicle alone in BRCA-2 deficient mice with pancreatic adenocarcinoma (KrasG12D/+; p53R270H/+; Pdx-1-Cre; Brca2mut ) [23]. MRI was done at regular intervals to detect tumor development. The results are shown in the Figure 2. They showed a significant prolongation of median overall survival and thus higher efficacy in Cisplatin treated mice compared to Ola alone or vehicle (p<0.001) and The benefit of adding Olaparib was increased time to tumor identification and reduced reuse of cisplatin.
Figure 2. Cisplatin treated mice compared to Ola alone or vehicle (p<0.001).
Discussion
Pancreatic adenocarcinomas with germline mutations in BRCA and related genes is an important subset of pancreatic cancers diagnosed every year. Prior and ongoing preclinical and clinical research to develop targeted therapies, including PARPi, as single or combination agent has shown great promise. Nuclear PARP has been shown to be an independent prognostic marker with respect to standard clinicopathological parameters [24]. The above mentioned studies have laid a foundation based on which multiple phase II/III trials are underway and are currently recruiting patients with the exception of one which is active but not recruiting (NCT01078662) (Table 4). The data from the studies will help a lot in establishing their efficacy and safety. Given the high mortality associated with these cancers, this is a step in the right direction.

Conflict of Interest
Authors declare no conflict of interest.
References
- American Cancer Society. Cancer Facts & Figures 2014. Atlanta: American Cancer Society. 2014.
- Lowery MA, Kelsen DP, Stadler ZK, Yu KH, Janjigian YY, Ludwig E, D'Adamo DR, et al. An emerging entity: pancreatic adenocarcinoma associated with a known BRCA mutation: clinical descriptors, treatment implications, and future directions. Oncologist. 2011; 16(10):1397-402. [PMID:21934105]
- Klein AP. Genetic susceptibility to pancreatic cancer. MolCarcinog. 2012; 51(1):14-24. [PMID: 22162228]
- Lucas AL, Shakya R, Lipsyc MD, Mitchel EB, Kumar S, Hwang C, Deng L, et al. High prevalence of BRCA1 and BRCA2 germline mutations with loss ofheterozygosity in a series of resected pancreatic adenocarcinoma and other neoplastic lesions. Clin Cancer Res. 2013; 19(13):3396-403 [PMID:23658460]
- The Breast Cancer Linkage Consortium. Cancer Risks in BRCA2 Mutation Carriers. J Natl Cancer Inst. 1999; 91(15):1310-6. [PMID:10433620]
- Thompson D, Easton DF. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst. 2002; 94(18):1358-65. [PMID:12237281]
- Iqbal J, Ragone A, Lubinski J, Lynch HT, Moller P, Ghadirian P, Foulkes WD, et al. The incidence of pancreatic cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer. 2012; 107(12):2005-9. [PMID:23099806]
- Carden CP, Yap TA, Kaye SB. PARP inhibition: targeting the Achilles’ heel of DNA repair to treat germline and sporadic ovarian cancers. CurrOpinOncol. 2010; 22(5):473-80. [PMID:20485165]
- Plummer ER, Calvert H. Targeting poly (ADP-ribose) polymerase: a two armed strategy for cancer therapy. Clin Cancer Res. 2007; 13(21):6252-6. [PMID:17975135]
- Rouleau M, Patel A, Hendzel MJ, Kaufmann SH, Poirier GG. PARP inhibition: PARP1 and beyond. Nat Rev Cancer. 2010;10(4):293-301. [PMID:20200537]
- Comen EA, Robson M. Inhibition of poly(ADP)-ribose polymerase as a therapeutic strategy for breast cancer. Oncology (Williston Park). 2010; 24(1):55-62. [PMID:20187322]
- Yuan Y, Liao YM, Hsueh CT, Mirshahidi HR. Novel targeted therapeutics: inhibitors of MDM2, ALK and PARP. J HematolOncol. 2011; 4:16. [PMID:21504625]
- Jacob DA, Bahra M, Langrehr JM, Boas-Knoop S, Stefaniak R, Davis J, Schumacher G, et al. Combination therapy of poly (ADP-ribose) polymerase inhibitor 3-aminobenzamide and gemcitabine shows strong antitumor activity in pancreatic cancer cells. J GastroenterolHepatol. 2007; 22(5):738-48. [PMID:17444865]
- Chen S, Wang G, Niu X, Zhao J, Tan W, Wang H, Zhao L, et al. Combination of AZD2281 (Olaparib) and GX15-070 (Obatoclax) results in synergistic antitumor activities in preclinical models of pancreatic cancer. Cancer Lett. 2014; 348(1-2):20-8. [PMID:24534203]
- Yuan K, Sun Y, Zhou T, McDonald J, Chen Y. PARP-1 regulates resistance of pancreatic cancer to TRAIL therapy. Clin Cancer Res. 2013; 19(17):4750-9. [PMID:23833311]
- Porcelli L, Quatrale AE, Mantuano P, Leo MG, Silvestris N, Rolland JF, Carioggia E, et al. Optimize radiochemotherapy in pancreatic cancer: PARP inhibitors a new therapeutic opportunity. MolOncol. 2013; 7(3):308-22. [PMID:23148997]
- Lowery MA, Kelsen DP, Stadler ZK, Yu KH, Janjigian YY, Ludwig E, D'Adamo DR, et al. An emerging entity: pancreatic adenocarcinoma associated with a known BRCA mutation: clinical descriptors, treatment implications, and future directions. Oncologist. 2011; 16(10):1397-402. [PMID:21934105]
- Fogelman DR, Wolff RA, Kopetz S, Javle M, Bradley C, Mok I, Cabanillas F, et al. Evidence for the efficacy of Iniparib, a PARP-1 inhibitor, in BRCA2- associated pancreatic cancer. Anticancer Res. 2011; 31(4):1417-20. [PMID: 21508395]
- Kaufman B, Shapira-Frommer R, Schmutzler RK, Audeh MW et al. Olaparibmonotherapy in patients with advanced cancer and a germline BRCA1/2 mutation: An open-label phase II study. J ClinOncol. 31, 2013; (ASCO 2013 suppl; abstr 11024).
- Pishvaian MJ, Wang H, Zhuang T, He AR et al. A phase I/II study of ABT-888 in combination with 5-fluorouracil (5-FU) and oxaliplatin (Ox) in patients with metastatic pancreatic cancer (MPC). J ClinOncol. 31, 2013; (suppl 4; abstr 147).
- O'Reilly EM, Lowery MA, Segal MF, Smith SC et al. Phase IB trial of cisplatin (C), gemcitabine (G), and veliparib (V) in patients with known or potential BRCA or PALB2-mutated pancreas adenocarcinoma (PC). J ClinOncol. 32:5s, 2014; (suppl; abstr 4023).
- Domchek S, McWilliams RR, Hendifar AE, Shroff RA. A phase 2, open-label study of rucaparib in patients with pancreatic cancer and a known deleterious BRCA mutation. J ClinOncol. 32:5s, 2014; (suppl; abstr TPS4161).
- Lowery MA, Lee A, Tobias E, Sung P et al. Evaluation of PARP inhibition as a platinum sparing strategy in Brca2-deficient pancreatic tumors. J ClinOncol. 32, 2014; (suppl; abstr e15237).
- Klauschen F, von Winterfeld M, Stenzinger A, Sinn BV, Budczies J, Kamphues C, Bahra M, et al. High nuclear poly-(ADP-ribose)-polymerase expression is prognostic of improved survival in pancreatic cancer. Histopathology. 2012; 61(3):409-16. [PMID:22384823]



