Héloïse Seux1, Jonathan Garnier1, Jacques Ewald1, Ugo Marchese1, Flora Poizat2, Jean-Robert Delpero1, Olivier Turrini3
1Department of Surgical Oncology, Institut Paoli-Calmettes, Marseille, France
2Department of Pathology, Institut Paoli-Calmettes, Marseille, France
3Aix-Marseille University, Institut Paoli-Calmettes, Department of Surgical Oncology CNRS, Inserm, CRCM, Marseille, France
- Corresponding Author:
- Jonathan Garnier
Department of Surgical Oncology
Institut Paoli-Calmettes, Marseille, France
Tel: +33491223660
Fax: +3349223550
E-mail: garnierj@ipc-unicancer.fr
Received Date: May 18th, 2020; Accepted Date: July 06th, 2020
Keywords
Distal cholangiocarcinoma, Para-aortic lymph node, Paraaortic
sampling
Abbreviations
PALN para-aortic lymph node; PD
pancreaticoduodenectomy; PDAC pancreatic ductal adenocarcinoma;
DC distal cholangiocarcinoma; BMI Body Mass Index; FS Frozen-
Section; PE Paraffin-Embedded; POPF Postoperative Pancreatic
Fistula;
INTRODUCTION
Classification of cholangiocarcinoma depends on the
anatomical location, and it is divided into intrahepatic,
perihilar, or distal subtypes. Distal Cholangiocarcinoma
(DC) originates anywhere from the cystic duct to the ampulla
of Vater and mainly requires a Pancreaticoduodenectomy
(PD) when deemed resectable. Even though the prognosis
is poor [1], patients with DC tend to have better
survival outcomes than those with Pancreatic Ductal
Adenocarcinoma (PDAC). In patients with PDAC, Para-
Aortic Lymph Node (PALN) involvement was identified
as a prognostic factor [2] when detected intra-operatively by frozen section analysis. Despite the lack of consensus
on a valid PD, our strategy is not to resect when positive
intraoperative PALNs are found [3]. As the indisputable
distinction between PDAC and other periampullary tumors
is sometimes difficult to confirm preoperatively, we have
routinely assessed the PALN status in patients eligible for
PD with malignant pancreatic head tumours. Although
they arise from the same anatomical location, PDAC and
DC may vary in their lymphatic spread [4]. The present
study aimed to evaluate PALN status and its impact on
patients with DC eligible for a PD.
METHODS
Patient Selection
From January 2011 to December 2019, 63 patients
with DC underwent curative PD at Paoli-Calmettes
Institute (Marseille, France). Of them, forty-two patients
had available information about their pathological
PALN status. Twenty-one patients did not have a PALN
resection because the supposed aetiology was not
PDAC or DC; however, they were ultimately diagnosed
with DC. The study was approved by the Institutional
Review Board. The study participants provided
written informed consent as their data are listed in our
declared prospective institutional database and labelled by the National Institute for Data Protection (CNIL
N°Sy50955016U; NCT02871336). The study protocol
adhered to the tenets of the Declaration of Helsinki. All
patients were initially staged following NCCN guidelines,
and all cases were discussed and validated for surgery
during a multidisciplinary board meeting.
Operative Technique
After careful abdominal exploration to eliminate the
possibility of metastatic disease, PALN sampling (station
16b1 of the Japanese staging and classification for
pancreatic and periampullary cancer) [5] was performed
after an extended Kocher manoeuvre by harvesting the
lymphocellular aortocaval tissue located below the left
renal vein to the origin of the inferior mesenteric artery. We
routinely achieved frozen sections (except in six patients
due to technical issues). Half of the collected PALNs were
stained with haematoxylin and eosin and examined for
the presence of metastases. The remaining sections were
for paraffin embedding examinations. PALNs that were
negative were further analysed immunohistochemically
for micrometastases detection. All tumours were analysed
according to a standardized pathological protocol, and an
experienced pathologist confirmed that they were DCs
(not PDACs) [6, 7].
Studied Variables
Numerous clinical variables were evaluated: age, sex,
BMI, biliary stenting, number of PALNs examined, positive
PALNs (after frozen section or at definitive histological
report), numbers of examined and positive lymph nodes,
margin status (i.e., R0 or R1 resection), tumor size or stage,
postoperative morbidity according to the Clavien-Dindo
classification, and survival.
Statistical Analysis
Analyses were performed using GraphPad Prism 8 (La
Jolla, CA, USA). Categorical factors were compared using
Fisher’s exact test or chi-squared test, and continuous
variables were analysed using the Student’s t-test. Overall
survival was calculated according to the Kaplan-Meier
method. All statistical significance levels were set at
P<0.05.
RESULTS
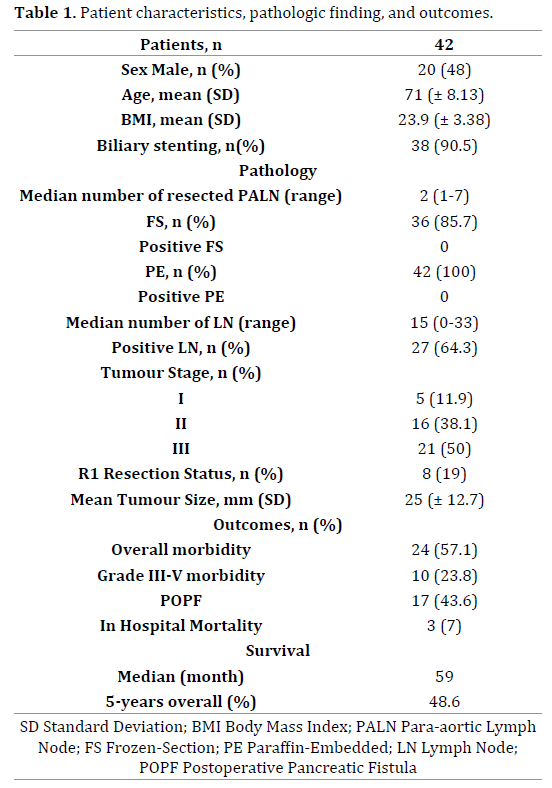
Patient characteristics, histopathological analysis
of the operative specimens, postoperative courses, and
survival are summarized in Table 1. The median number
of PALN analysed was 2 (range 1-7) out of a median of
15 lymph nodes. All PALN frozen section analyses were
negative, as were the definitive pathology results. Most
patients had an advanced stage (stage I: 11.9%; stage II:
38.1%; stage III: 50%) and R1 resection rate was 19%.
Postoperative Pancreatic Fistula (POPF) occurs in 43%
leading to a 24% of Clavien ≥ 3 complications, and 7% of
postoperative deaths. The median overall survival time
was 59 months. The 5-year overall survival rate was
48.6%.
DISCUSSION
During an eight-year study, we analyzed forty-two PDs
for DC, and PALNs were not found to be a site of lymphatic
spread in patients with DC. In several reports, tumorinfiltrative
PALNs were found in about 10% of patients
with PDAC and were associated with poor survival [2]. To
our knowledge, PALN status in patients who underwent
PD for malignant tumors other than PDAC has yet been
reported. We want to emphasize that an experienced
pathologist performed all histo-pathological analyses; this
ensures accurate diagnosis of DC and also the relevance
of the PALN analysis even if the median number of
PALN analyzed was low. Although our small sample size
precludes definitive conclusions, it highlights the debate
about lymphatic drainage in DC.
Yoshida et al. [8] reported a high rate (55%) of tumor
infiltrated PALNs in patients with DC that has never before
been observed. None of these PALNs were involved in
our study (despite a majority of tumor stages II and III
according to the 7th edition of the AJCC staging), only 13%
and 7.5% in the more recent studies [9, 10]. Overall, lymph
node status (N+) in patients with DC was consistently
reported as similar to patients with PDAC, and this was
confirmed here with a 64% tumor-infiltrated lymph node
status. However, the lymphatic network of the pancreatic
head is complex, and mechanisms regulating lymphatic
invasion are poorly understood. Furthermore, DC seems to have a similar capacity for lymphatic spread as PDAC,
but does not seem to reach the PALNs despite the claims
of previous literature [11]. As PDAC and DC are different
diseases with a unique extension [12] including within
the DC subtype [13, 14, 15] it makes sense that a different
lymphatic network should result in a different PALN
invasion capacity.
CONCLUSION
Our findings suggest that PALN sampling and frozen
section examination is futile for analyzing DC. However,
as the specific preoperative distinction between DC and
PDAC is difficult, PALN dissections during PD must be
routinely accomplished in uncertain cases. The question
remains about adjuvant treatment in patients with positive
PALN on Paraffin-Embedded (PE) analysis, as they have to
be assumed to be metastatic. In such situations, unusual
adjuvant therapy could be considered rather than the
standard regimen of capecitabine treatment.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- Ethun CG, Lopez-Aguiar AG, Pawlik TM, Poultsides G, Idrees K, Fields RC, et al. Distal Cholangiocarcinoma and Pancreas Adenocarcinoma: Are They Really the Same Disease? A 13-Institution Study from the US Extrahepatic Biliary Malignancy Consortium and the Central Pancreas Consortium. J Am Coll Surg 2017; 224:406-413. [PMID: 28017812]
- Schwarz L, Lupinacci RM, Svrcek M, Lesurtel M, Bubenheim M, Vuarnesson H, et al. Para-aortic lymph node sampling in pancreatic head adenocarcinoma. Br J Surg 2014; 101:530-538. [PMID: 24633831]
- Marchese U, Ewald J, Gilabert M, Delpero J-R, Turrini O. Outcomes of pancreatic adenocarcinoma that was not resected because of isolated para-aortic lymph node involvement. J Visc Surg 2019; 156:97-101. [PMID: 30026012]
- Pomianowska E, Westgaard A, Mathisen Ø, Clausen OPF, Gladhaug IP. Prognostic Relevance of Number and Ratio of Metastatic Lymph Nodes in Resected Pancreatic, Ampullary, and Distal Bile Duct Carcinomas. Ann Surg Oncol 2013; 20:233-241. [PMID: 22893118]
- Tol JAMG, Gouma DJ, Bassi C, Dervenis C, Montorsi M, Adham M, et al. Definition of a standard lymphadenectomy in surgery for pancreatic ductal adenocarcinoma: a consensus statement by the International Study Group on Pancreatic Surgery (ISGPS). Surgery 2014; 156:591-600. [PMID: 25061003]
- Verbeke CS, Gladhaug IP. Resection margin involvement and tumour origin in pancreatic head cancer. Br J Surg 2012; 99:1036-1049. [PMID: 22517199]
- Delpero JR, Bachellier P, Regenet N, Le Treut YP, Paye F, Carrere N, et al. Pancreaticoduodenectomy for pancreatic ductal adenocarcinoma: a French multicentre prospective evaluation of resection margins in 150 evaluable specimens. HPB 2014; 16:20-33. [PMID: 23464850]
- Yoshida T, Aramaki M, Bandoh T, Kawano K, Sasaki A, Matsumoto T, et al. Para-aortic lymph node metastasis in carcinoma of the distal bile duct. Hepatogastroenterology 1998; 45:2388-2391. [PMID: 9951929]
- Nappo G, Borzomati D, Perrone G, Valeri S, Amato M, Petitti T, et al. Incidence and prognostic impact of para-aortic lymph nodes metastases during pancreaticoduodenectomy for peri-ampullary cancer. HPB 2015; 17:1001-1008. [PMID: 26335256]
- Hempel S, Oehme F, Müssle B, Aust DE, Distler M, Saeger H-D, et al. Prognostic impact of para-aortic lymph node metastases in non-pancreatic periampullary cancer. World J Surg Oncol 2020; 18:16. [PMID: 31964383]
- Yoshida T, Matsumoto T, Sasaki A, Morii Y, Shibata K, Ishio T, et al. Lymphatic spread differs according to tumor location in extrahepatic bile duct cancer. Hepatogastroenterology 2003; 50:17-20. [PMID: 12629981]
- Menon KV, Gomez D, Smith AM, Anthoney A, Verbeke CS. Impact of margin status on survival following pancreatoduodenectomy for cancer: the Leeds Pathology Protocol (LEEPP). HPB 2009; 11:18-24. [PMID: 19590619]
- Kamposioras K, Anthoney A, Fernández Moro C, Cairns A, Smith AM, Liaskos C, et al. Impact of intrapancreatic or extrapancreatic bile duct involvement on survival following pancreatoduodenectomy for common bile duct cancer. Br J Surg 2014; 101:89-99. [PMID: 24375301]
- Miyazaki M, Ohtsuka M, Miyakawa S, Nagino M, Yamamoto M, Kokudo N, et al. Classification of biliary tract cancers established by the Japanese Society of Hepato-Biliary-Pancreatic Surgery: 3(rd) English edition. J Hepato-Biliary-Pancreat Sci 2015; 22:181-196. [PMID: 25691463]
- Primrose JN, Fox RP, Palmer DH, Malik HZ, Prasad R, Mirza D, et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol 2019; 20:663-673. [PMID: 30922733]

