Keywords
Pancreatic Cyst; Pancreatic Fistula; Pancreatic Pseudocyst; Pancreatitis; Stents
INTRODUCTION
A pancreatico-pleural fistula is a rare complication of chronic or acute pancreatitis. The communication between the thoracic structures and pancreatic duct can be through pseudocysts which may be incompletely formed or ruptured or through thin linear fistulous tracts through the esophageal or aortic diaphragmatic orifice or less commonly transdiaphragmatically.The result is large pleural effusions, unilateral or bilateral, mediastinal fluid collections or pseudocysts [1]. Communications between pancreatic ducts or collection with different intrathoracic structures have been reported most commonly with pleura and mediastinum, but also with pericardium and bronchus [2, 3].
In the past majority of pancreatico-pleural fistulas had been surgically treated most commonly with distal pancreatectomy and pancreaticojejunostomy. Few were conservatively managed with reports of successful medical management with octreotide [4]. With the development and refinements in endoscopic techniques, there were reports of successful treatment of these entities with endoscopic pancreatic duct stenting [5]. Conservative and expectant management while catering to fluid collections in the chest and abdomen have been advocated with surgery being reserved for cases in whom these measures have failed to relieve the symptoms [6].
METHODS
After obtaining the institutional ethics committee approval, retrospective review was done of the medical records of five patients of pancreatico-pleural fistulae who were diagnosed and successfully managed in year 2012 and 2013 in our hospital, which is a large urban tertiary care hospital and teaching institution in south India . Follow up without patient records of these patients was also included. The review included discharge summaries, laboratory, radiographic and endoscopic reports on hospital information system, radiographic and endoscopic images on PACS and outpatient records from records department. Findings were compared with the current available literature on this entity.
CASE REPORT
Case 1
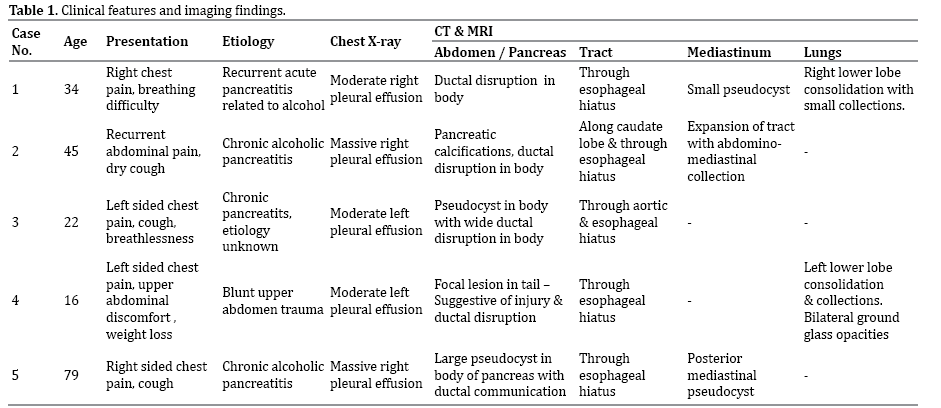
A thirty four years old male with history of alcohol related acute pancreatitis was admitted with right sided chest pain and breathing difficulty. Chest X-ray revealed moderate right pleural effusion, pleural fluid amylase was grossly elevated measuring 35, 590 U/L. CT demonstrated pancreatic ductal disruption in body of pancreas with a tract through esophageal hiatus and small mediastinal pseudocyst. There was also central peribronchovascular consolidation in the lower lobe of right lung with hypodense collections in the lung parenchyma and was judged to be pancreatico-bronchial fistula through these intraparenchymal collections due to the patient developing characteristic expectoration of copious amount of rusty brown coloured sputum during his hospital stay (Figure 1).
Figure 1. Chest CT demonstrates small posterior mediastinal collections
along with lung parenchymal consolidations and small collections due to
pancreatico-pleural –bronchial fistula.
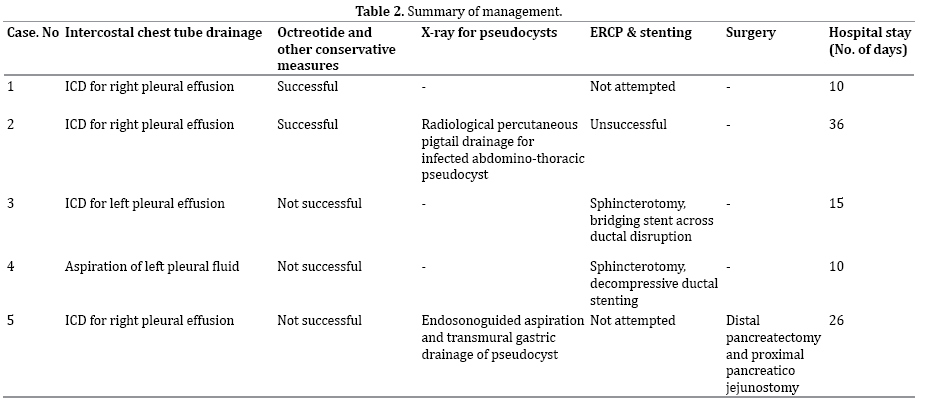
Conservative management was adopted with patient kept nil per oral and on NJ tube. He was started on NJ feeds gradually. Simultaneously analgesics, injection octreotide, IV fluids, prophylactic antibiotics were administered. Intercostal chest tube was inserted to drain the pleural fluid. The patient responded to conservative measures with hospital stay of ten days. Resolution of lung consolidation was noted in subsequent X-rays and long term follow up of approximately one year has not shown any recurrence.
Case 2
A forty five year old male, case of alcohol related chronic pancreatitis admitted with recurrent abdominal pain with dry cough. Chest X-ray showed massive right pleural effusion. Pleural fluid amylase was significantly elevated (67440 U/L). Intercostal drain was inserted to drain the pleural effusion. CT demonstrated features of calcific pancreatitis with ductal disruption in the body with pleuro-peritoneal and mediastinal fistulous tract along caudate lobe of liver (Figure 2).
Figure 2. Coronal CT reformat demonstrates a linear pancreatico -pleural
fistulous tract along the caudate lobe of liver.
The ductal disruption was localized to the superior body of pancreas. ERCP was attempted which showed disruption of the pancreatic duct in the body region, however the guide wire could not be negotiated into the ductal system and stenting was not successful. The patient was managed conservatively on nasoenteral feeds, intercostal tube drainage, injection octreotide and other supportive measures. During the hospital stay the patient developed persistent fever unresponsive to antibiotics. A repeat CT showed expansion of the pancreatico-mediastinal fistulous tract with large lobulated fluid collection along the pancreatic body which tracked through the esophageal hiatus into the posterior mediastinum (Figure 3). Ultrasound guided aspiration of collection was done which revealed frank purulent aspirate. This infected abdominothoracic collection was treated with percutaneous catheter drainage with placement of 10F pig tail catheter under ultrasound guidance, allowing complete drainage of the intra-abdominal and intrathoracic components of the pseudocyst over a period of approximately 1 week. The patient was also managed alongside with antibiotics and other supportive measures. The patient showed considerable improvement and was subsequently discharged. No separate treatment was thereafter required for the pancreatico-pleural fistula or ductal disruption. The total hospital stay was of 36 days. A follow up over approximately one year has not shown any recurrence of peripancreatic or chest collections. Recently the patient had a recurrent episode of acute exacerbation of pancreatitis involving body and tail region which was deemed to be of mild clinical severity and required a brief hospitalization.
Figure 3. Follow up CT in the above patient after few days of conservative
management shows expansion of the fistulous tract with development of
large collection along the tract extending into the mediastinum.
Case 3
A twenty three year old male with chronic pancreatitis presented with complaints of cough, left sided chest pain and breathlessness of one day duration and was admitted in the department of pulmonology. Chest X-ray revealed moderate left pleural effusion. Pleural fluid analysis revealed significantly elevated levels of amylase of 25,569 U/L. CT scan demonstrated pseudocyst in the body of pancreas with a wide disruption in the posterosuperior aspect of the body of pancreas and fistulous tracts into the mediastinum and left pleura through the esophageal and aortic hiatus. Intercostal tube drainage was performed for pleural effusion. The patient was transferred to gastroenterology and was initially managed conservatively. Due to no significant improvement in clinical condition, endoscopy with ERCP and pancreatic ductal stenting was planned. Endoscopy demonstrated deformed duodenum and pulled up ampulla. Cholangiogram demonstrated dilated CBD and smooth stricture in the lower CBD for which wide sphincterotomy was done. Pancreatogram showed multiple areas of dye leakage in the main pancreatic duct suggestive of multiple ductal disruptions (Figure 4). The areas of dye leakage were present in the head and body with no areas of leakage in the tail region. The guide wire was negotiated upto the tail region, pancreatic duct sphincterotomy was done. A 7F 9 cms straight stent was placed across the pancreatic duct. The patient showed significant clinical improvement post procedure. The total hospital stay was of fifteen days. Pancreatic duct stent removal was done endoscopically after further three months (total seven months after they were inserted). There has been no recurrence of any fluid collections in the chest.
Figure 4. ERCP in a patient with pancreatico-pleural fistula demonstrating
multiple ductal disruptions and leakage of dye.
Case 4
A Sixteen year old male who had sustained an injury following fall two months ago following which he had abdominal pain for 2 weeks which subsided with conservative management at local outside hospital. He presented sometime later with left sided chest pain, vague left upper abdomen discomfort, post prandial abdominal pain and significant weight loss. Chest X-ray showed a massive left pleural effusion for which he was admitted in the department of pulmonology. CT revealed a large left sided pleural effusion. There were in addition multiple ground glass opacities in both lungs and consolidation in the left lower lobe. Upper slices of abdomen revealed a focal hypodense lesion in the tail of pancreas with a small track leading to left lung consolidation through the esophageal hiatus suggesting pancreatico-pleural and pancreatico bronchial fistula likely post traumatic etiology. The ground glass opacities in both lungs could be explained by the aspiration of pancreatic contents through pancreaticobronchial fistula. An MRI obtained confirmed the CT findings and demonstrated a small pseudocyst communicating with main pancreatic duct and pancreatico-pleural–bronchial fistula (Figure 5). It was decided to attempt ERCP due to no significant response to conservative measures. ERCP revealed a normal cholangiogram while a pancreatogram revealed mild leakage of dye in the main pancreatic duct at the junction of body and tail of pancreas. Pancreatic duct sphincterotomy was done and a 7F 9cm straight stent was placed across the main pancreatic duct. Since actual ductal disrupton was in the tail of pancreas it could not be bridged and the stenting was purely decompressive in nature. Post ERCP period was uneventful. He was subsequently discharged and later underwent aspiration of the residual pleural fluid collection. The patient did well subsequently and underwent stent removal after six months and has not had a recurrent fluid collection in the chest or abdomen on follow up.
Figure 5. Coronal MRI image demonstrates a fistulous tract form the tail
region of pancreas heading superiorly towards the left hemidiaphragm
along with left pleural effusion.
Case 5
A seventy-nine-year-old man, known alcoholic who presented with complaints of cough, right sided chest pain and abdominal pain since 3 months. There was right sided massive pleural effusion. Pleural fluid analysis showed mildly elevated amylase levels of 1,725 U/L. CT showed cystic fluid collection arising from the body of pancreas and communicating with the pancreatic duct with the collection tracking superiorly around the gastroesophageal junction into the posterior mediastinum where small multicystic collections were noted communicating with the right pleural effusion. ERCP was not attempted as CT had demonstrated wide communication of the duct with pseudocyst, significant atrophy of the pancreatic parenchyma distal to the ductal disruption and an impacted calculus proximally, hence chances of technically successful endoscopic stenting were deemed low. Since the pancreatic pseudocyst was behind the stomach endoscopic ultrasound guided transmural drainage of pseudocyst was attempted. Endoscopic ultrasound demonstrated a small well defined pseudocyst in the lesser sac with communication with the main pancreatic duct and pancreatico-pleural fistula with pseudocyst communicating with right pleural effusion (Figure 6). Endoscopic transmural gastric drainage of pseudocyst was done and the tapped fluid showed grossly elevated amylase levels of 109,800 U/L. However due to small size of the pseudocyst and immature walls, dislodgement of the catheter was noted on follow up CT. The dislodged catheter was snared endoscopically. The patient was nonresponsive to conservative management and had persisting pleural effusion and abdominal pain. He underwent successful surgical treatment which included distal pancreatectomy, splenectomy and proximal pancreatico-jejunostomy. Intraop complication included bleeding from short gastric vessels and splenic vein and brief episode of hypotension requiring dopamine infusion. Postoperatively the patient required ventilator support for one day. The patient also required drainage of the right pleural fluid collection postoperatively. The total hospital stay was of 26 days. Long term follow up had not shown any recurrent symptoms (Table 1).
Figure 6. Endoscopic ultrasound image acquired superiorly shows
communication (comm.) of cyst (arrow) with pleural effusion.
DISCUSSION
We had five cases of pancreatico-pleural fistula, of which two had additionally pancreatico-bronchial fistulae. Three cases had in addition large abdominal, mediastinal pseudocysts or fluid collections of which one case had infected collection with frank abscess. Successful management of these conditions requires an accurate timely diagnosis and adherence to standard treatment protocol. The patients present with unilateral or bilateral massive pleural effusions.In addition there can be mediastinal collections or lung parenchymal collections with bronchial communications. In the latter scenario the patient has complaint of coughing out copious amounts of rusty coloured material. Due to localization of complaints primarily to the chest the patients are frequently initially seen by the respiratory physicians. Establishment of diagnosis requires a careful attention to history and subsequent cross sectional imaging to identify pancreatico-pleural or mediastinal fistulae. Analysis of pleural fluid reveals a transudative effusion with elevated pleural fluid amylase, the amylase levels may be as high as 30,000-60,000 U/L.
Contrast CT is often the next investigation after chest radiography and accurately establishes the diagnosis of pancreaticopleural fistulae. The findings include pancreatic ductal disruptions and fistulous tracts. A wide communication with the pleural cavity may be evident in some cases, in others intra-thoracic extension of the tracts with small posterior mediastinal fluid collections are seen with communication with pleural cavity being inferred due to presence of pleural effusion. The collections usually track along the right or left crus of diaphragm through the esophageal or aortic hiatus. Associated mediastinal and intra-abdominal fluid collections and pseudocysts may be seen and these usually lie along the path of the tract, though other separate collections may also be co-existing. CT can also demonstrate the status of the main pancreatic duct and can be helpful in deciding the management strategy including the technical feasibility of endoscopic stenting and trajectory planning of percutaneous drainage of fluid collections. In our case series an accurate diagnosis of pancreatico-pleural or pancreatico-bronchial fistulae was achieved in all cases with CT scan of chest and abdomen. MRI is complementary and affords more detail and clarity. Thus ERCP purely for diagnostic purposes may not be necessary, this is in contradistinction to some of the earlier reported case series on this entity [7]. Endoscopic ultrasound can also demonstrate the fistulous tracts and ductal and pleural communications (Figure 6), however being invasive its role should be primarily for interventions in pancreatic collections.
An initial conservative approach to management of these conditions is appropriate. Patients generally require intercostal tube drainage for large pleural collections. The medical management consists of administration of synthetic somatostatin analogue octreotide. It has a longer half-life compared to somatostatin and acts to dramatically decrease pancreatic exocrine secretion thus decreasing the fistula output [7]. It can be administered subcutaneously with dose titration upto a maximum of 250 μg thrice daily. This is combined with other measures including NJ feeds, chest drains and percutaneous therapies for pseudocysts as in the first two cases.The first two cases which were successfully treated with conservative measures, received octreotide during their hospital stay, first case for 10 days duration and the second case for four weeks. Usually the response to these measures is rapid in responders and the conservative medical management may not exceed more than two to four weeks [6]. Supportive and medical management can alleviate symptoms and lead to rapid improvement. In some patients a conservative management is all that is required as noted in the first case. A favourable response to conservative management combining enteral nutrition and somatostatin analogues obviates the need for pancreatic stenting or surgery. Failure of medical therapy is indicated by continued abdominal pain and failure of clearing of pleural effusions and pseudocysts.
Historically before the advent of ERCP and stenting, the treatment consisted of conservative medical management and surgery in nonresponsive cases with the world literature of that time reporting a significantly high rate of surgical intervention, with as many as 66 of 89 reviewed patients by Rocky and Cello underwent surgery [8]. With the advent of endoscopic techniques and further refinements there have been more reports of successful endoscopic treatments. This includes a series of four cases of which two patients underwent successful treatment with ERCP and stenting, while other two responded to conservative management with octreotide, including one with failed ERCP and stenting [7]. In another series of eight cases, a successful pancreatic stenting with bridging of the site of ductal diusruption was possible in only one case, with surgery required in four cases and remaining three cases responding to further conservative measures [9]. Hence ERCP and stenting may not be feasible or successful in all cases. This is also noted in our case series in which ERCP and stenting was successful in two of the three attempted cases with actual bridging of ductal disruption in one case and a decompressive stenting with sphincterotomy in another case. The case with purely decompressive stenting showed good results similar to bridging stent. Thus the primary roles of ERCP in these conditions is two fold, first consists of decompressing the ductal system with measures like sphincterotomy, dilatation of ductal strictures and extraction of any obstructing calculi, the other being to bridge the site of ductal disruption by inserting a stent across the ductal disruption [6]. Both the objectives may be achieved if the fistula arises from the head or body of pancreas as noted in the third case above while bridging may not be feasible if the fistula arises from the distal body or tail and the only option may be to decompresses the ductal system by sphincterotomy and stenting as in fourth case above. The stents used range from 5F to 7F size, with 7F usually being preferred by us. No large studies have assessed optimum duration of drainage with pancreatic stents, duration usually varies from 4 to 12 weeks [6]. The two patients who had undergone pancreatic stenting in our series had their stents removed after six and seven months respectively and have done well subsequently The common reasons for failure of ERCP and stenting include failure of cannulation of pancreatic duct, stricture or stones in the main pancreatic duct or location of the fistula distally in the tail of pancreas [9]. In the latter scenario however decompressive ductal stenting can be performed. Failure of ERCP and ductal stenting should not however always mean surgical intervention and conservative management can be continued for some more time and may result in successful outcome as noted in the second case above with similar cases also noted in the different literatures [7, 9].
Management of the fluid collections or pseudocyst which usually forms part of the fistulous tract is important and can be done as in other pancreatic pseudocysts by percutaneous radiological approach or by endoscopic ultrasound guided transmural drainage. The infected collections are best managed radiologically by percutaneous aspiration or drainage (CT or ultrasound guided) as in the second case. Percutaneous catheter drainage is part of emergency treatment of infected pseudocyst [10]. It affords rapid symptomatic relief and allows complete drainage of infected material and resolution of pseudocyst. Percutaneous drainage of mediastinal pseudocysts is also possible and various approaches including indirect drainage by draining the abdominal component of pseudocyst as in second case above, paraspinal extrapleural CT guided approach or transhepatic subxiphoid approach has been described [11]. A successful percutaneous radiological treatment of the associated collection along with conservative and supportive measures may be all that is required in some cases and may result in clinical improvement with no further therapy needed for pancreaticopleural fistula or ductal disruption as noted in second case. Endoscopic transmural pseudocyst drainage has a low complication rate [10]. A common endoscopic approach is transmural drainage – placing stents through the gastric or duodenal wall and is done through a EUS scope. The prerequisites are no vascular structures are present between the gastric wall and pseudocyst, and the distance between the gastric or duodenal wall and the pseudocyst should be less than 1 cm [12]. Initial technical success was noted in the fifth case above, this was however followed by stent dislodgement. The possible reasons for this could have been the immature cyst walls, lack of firm abutment of the cyst with the gastric wall and a relatively small size of the cyst. Persistence of symptoms in this patient and lack of adequate response to conservative management lead to surgical intervention.
Surgery is needed in patients not responding to conservative and medical management or endoscpic stenting and also in patients with recurrence of symptoms. Surgery involves removal of the diseased portion of the pancreas by partial pancreatectomy and pancreatico jeunostomy. Surgery is a major endeavor in these patients and is not without risks with somewhat stormy but manageable post-operative course. Simpler forms of surgery, from the thoracic approach with use of pedicled intercostal muscle flap tagged around the fistula into diaphragm to close the pancreatico-pleural fistulous tract have also been described [13]. Some studies have also demonstrated shorter hospital stay in patients who were operated early in the course of disease [14] (Table 2).
The management strategy needs to be individualized for each patient depending on the clinical situation. Follow up is essential for signs of recurrence. Chest X-ray and ultrasound are the most basic investigations which can be offered during periodic OPD visits. It should be remembered that these patients have established chronic pancreatitis, new complications developing due to their underlying condition including recurrent acute exacerbations is to be expected.
Conflict of Interest
Authors declare that they have no conflict of interest to disclose.
References
- Tombroff M, Loicq A, De Koster JP, Engleholm L, Govaerts JP. Pleural effusion with pancreaticopleural fistula. Br Med J. 1973; 1: 330-331. [PMID: 4685624]
- Sakurai T, Fujiyama R, Ohnishi H, Tada K, Tomioka H, Sakamoto H, Iwasaki H, Aoki M. Pancreatic pleural effusion accompanied by bronchopleural fistula. Nihon Kokyuki Gakkai Zasshi. 1999; 37: 662-666. [PMID: 10496109]
- Balasubramanian P, Jeyamani R, Govil S, Chacko A, Kurian G, Subhash HS, Govil S, Thomas K. Pancreatico-pericardial fistula: a rare complication of chronic pancreatitis. Indian J Gastroenterol. 2004; 23: 31- 32. [PMID: 15106719]
- Poddar U, Kochhar R, Singh A, Nagi B, Singh K. Pancreatico-pleural fistula: successful treatment with octreotide. Indian J Gastroenterol. 1995; 14: 145-146. [PMID: 8868358]
- Safadi BY, Marks JM. Pancreatic-pleural fistula: the role of ERCP in diagnosis and treatment. Gastrointest Endosc. 2000; 51:213-215. [PMID: 10650272]
- Machado NO. Pancreaticopleural Fistula: Revisited. DiagnTherEndosc. 2012. [PMC: 815476]
- Dhebri AR, Ferran N. Nonsurgical Management of Pancreaticopleural Fistula. J Pancreas. 2005; 6: 152-161.
- Rockey DC, Cello JP. Pancreaticopleural fistula: report of 7 patients and review of the literature. Medicine (Baltimore) 1990; 69: 332-344. [PMID: 2233231]
- Wronski M, Slodkowski M, Cebulski W, Moronczyk D, Krasnodebski IW. Optimizing management of pancreaticopleural fistulas. World J Gastroenterol. 2011; 17: 4696–4703. [PMC: 3233676]
- Lerch MM, Stier A, Wahnschaffe U, Mayerle J. Pancreatic pseudocysts: observation, endoscopic drainage, or resection? DtschArzteblInt 2009; 106: 614-621. [PMID: 19890418]
- Aabakken L, Chittom P, McKay DC, Uflacker R, Wilson FA. Percutaneous drainage of a mediastinal pancreatic pseudocyst: a paraspinal, extrapleural CT-guided approach. J VascInterv Radiol 1997; 8: 283-285. [PMID: 9083998]
- Jacobson BC, Baron TH, Adler DG, Davila RE, Egan J, Hirota WK, Leighton JA, Qureshi W, et al. ASGE guideline: the role of endoscopy in the diagnosis and the management of cystic lesions and inflammatory fluid collections of the pancreas. Gastrointestendosc. 2005; 61: 363-370. [PMID: 15758904]
- Amer K, Mahesh B, Ascione R. Pedicled intercostal muscle flap: a simple technique of closing pancreatico-pleural fistula from a thoracic approach. Eur J Cardiothorac Surg. 2002; 22: 831-832. [PMID: 12414056]
- King JC, Reber HA, Shiraga S, Hines OJ. Pancreatic-pleural fistula is best managed by early operative intervention. Surgery. 2010; 147: 154- 159. [PMID: 19744435]







