Keywords
Cholangiopancreatography, Endoscopic Retrograde;
Pancreatitis
Abbreviations
ERCP endoscopic retrograde
INTRODUCTION
The Endoscopic Retrograde Cholangiopancreatography
(ERCP) is an advanced endoscopic procedure for diagnosis
and treatment of several biliary and pancreatic disorders
[1]. The ERCP is usually safe and carries expedited
postoperative recovery. However, related complications
such as post-ERCP pancreatitis (PEP), gastrointestinal
bleeding/perforation, biliary infection (cholangitis), and
even death may occur [2].
PEP is the most common complication following ERCP.
The estimated related annual costs exceed 150 million
dollars in the United States [1]. The incidence ranges from
2% to 10% and most patients present non-severe and selflimited
forms of PEP. However, some patients may present
severe pancreatitis and demand aggressive medical
interventions, particularly those with associated risk
factors [3]. Risk factors for PEP entail young age, female gender, previous history of cholangitis or pancreatitis,
prior post-ERCP pancreatitis, recurrent pancreatitis,
sphincter of Oddi dysfunction, repeated bile/pancreatic
duct cannulations, iatrogenic procedural injury, presence
of gallstones, periampullary diverticulum, and insufficient
pancreatic drainage. In high-risk patients, the incidence of
PEP ranges from 20% to 30% and increase length of stay
and medical costs [4, 5].
Pancreatic stenting is a prophylactic intervention to
avoid PEP, even though its mechanism of action is not
clear [6, 7]. Previous meta-analyses [3] have shown that
pancreatic stent placement benefits especially highrisk
patients. However, some of those studies included
both abstracts and full-text articles, and did not assess
related complications, which may have led to inaccurate
conclusions. Others, enrolled different populations in the
same analysis (high and low risk patients) [3, 4]. Once
again, there was no evaluation of complications.
Therefore, we performed this systematic review and
meta-analysis to elucidate efficacy and safety of pancreatic
stenting to prevent PEP in high-risk patients through a
strict and clear methodology.
MATERIALS AND METHODS
This systematic review was performed according to
the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)
[8] and was registered in the PROSPERO database
(CRD42017056261).
Eligibility criteria
Types of studies: Only RCTs were included. There was
no language or publication dates restriction. Abstracts and
studies enrolling low-risk patients were excluded [9, 10, 11].
Types of participants: Patients older than 18 years who
underwent ERCP.
Types of intervention: Pancreatic stenting
(intervention) versus no stent (control).
Types of outcomes: The main outcome was the
incidence and severity of PEP; secondary outcomes were:
hyperamylasemia rate, presence of abdominal pain, incidence
of cholangitis, duration of ERCP and length of stay.
Databases
We searched MEDLINE/PubMed, LILACS, Embase,
and Cochrane CENTRAL databases from inception to
October 2016; then, a manual search was performed
using references of the selected studies and previous
systematic reviews regarding PEP in high-risk patients.
The search strategy for MEDLINE was: (Endoscopic
Retrograde Cholangiopancreatography OR ERCP OR
Cholangiopancreatography, Endoscopic Retrograde OR
Retrograde Cholangiopancreatography Endoscopic) AND
(stent*) AND (pancreatitis OR pancreatic).
Selection of studies
Two independent reviewers assessed the studies for
eligibility. Discrepancies were resolved by consensus with
the others authors.
Risk of bias in studies
We analyzed the risk of bias in the studies by means of a
standardized table considering randomization, allocation,
blinding, withdrawal, prognostic factors, outcomes, and
intention-to-treat analysis. Also, all studies were classified
according the JADAD scoring system [12].
Data extraction
The first author extracted data from eligible studies
and organized spreadsheets divided in two groups
(intervention and control). A second author checked the
extracted data.
Statistical Analysis
The analyses were carried out with RevMan 5.3
software. Risk difference (RD) expressed differences
between outcomes for dichotomous variables and
means difference (MD) for continuous variables using
the Cochrane–Mantel–Haenszel test (95% confidence
interval). Also, we used inverse variance with fixed-effect
(95% confidence interval).
The heterogeneity among studies was assessed with
the Higgin`s test (I2). Sensitivity analysis was performed when the heterogeneity was greater than 50%. A funnel
plot analysis aimed at identifying the study most likely to
carry publication bias (outlier). If an outlier was identified,
we excluded it and ran another analysis. If an outlier study
was not distinguishable, we considered true heterogeneity
and ran analysis using random-effect model to reduce
the impact of heterogeneity on outcomes. Forest plots
expressed graphically the results from the meta-analysis.
RESULTS
The initial search identified 2.805 articles screened
through title and abstract assessment. Fifteen articles
were selected. Among them, two studies presented only
abstracts [9, 10] while another did not evaluate highrisk
factors [11] and thus were excluded from this metaanalysis.
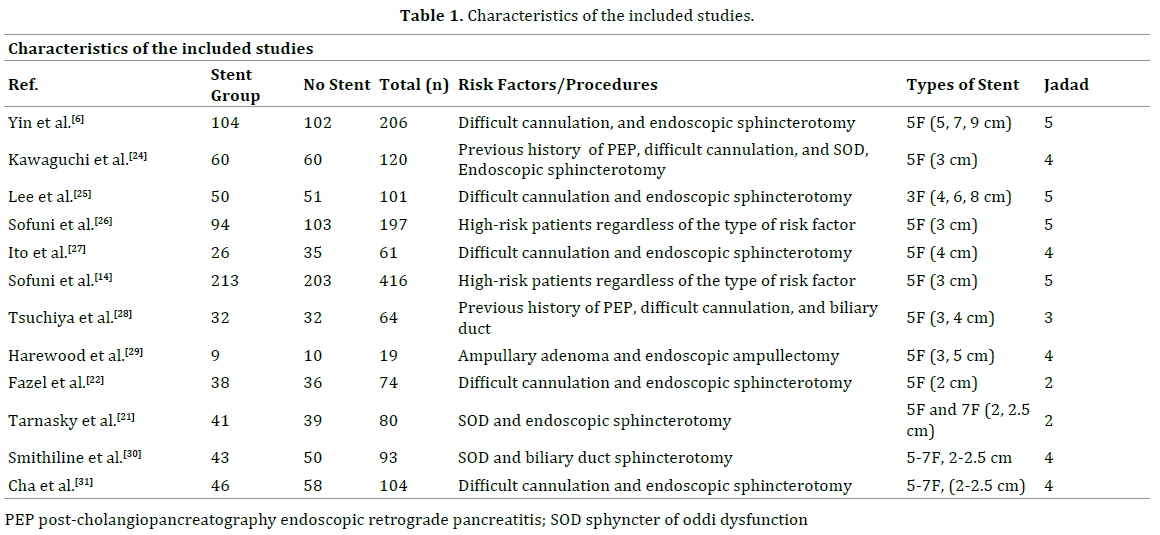
Finally, 12 RCTs enrolling 3.310 patients were
considered eligible (Figure 1). All trials were published
between 1990 and 2016 and randomly assigned 1673
high-risk patients to pancreatic stenting group and 1673
to the no stent group (Table 1).
Figure 1. PRISMA flowchart: flow of information through the systematic review.
Pancreatitis Severity Subgroups
A. Mild pancreatitis: The incidence of mild pancreatitis
was higher among no stent group patients: 11% (70/632)
vs. 4.8% (30/617). The meta-analysis showed statistical
difference in mild PEP incidence between groups
(p<0.0001) with RD of -0.06 (95% CI-0.09 -0.03) and low
heterogeneity (I2=0%) (Figure 2). The number needed to
treat was 2.5.
Figure 2. Forest plots and funnel plot. Forest plot depicting the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) in
the analyzed studies according to pancreatitis severity. (a). Mild pancreatitis; (b). Moderate pancreatitis; (c). Severe pancreatitis.
B. Moderate pancreatitis: The incidence of moderate
pancreatitis was also higher in the no stent group: 4.8%
(28/572) versus 1.4% (8/557). The risk difference was
-0.03 (95% CI-0.06 -0.01) favoring the pancreatic stenting
group (p<0.0001) in a highly homogenous analysis
(I2=0%). The number needed to treat was 5.
C. Severe pancreatitis: Again, the incidence of severe
pancreatitis was higher in the no stent group: 2.5% (12/469)
versus 0.2% (1/463). The risk difference between groups
was -0.02 (95% CI- 0.04 -0.00) with p<0.0001 and I2=47%
(Figure 2). The number needed to treat was 9.1
Hyperamylasemia
All articles assessed hyperamylasemia rate. In
pancreatic stenting group, 167 out of 710 patients (23.5%)
presented increased amylase in comparison with 619
among the 721 patients from the no-stent group. The
pancreatic stenting group showed significant lower risk
for hyperamylasemia (p<0.0001) (RD -0.62, 95% CI-0.65
-0.59). The number needed to treat was 0.2. However, we
detected high heterogeneity in this analysis (I2=100%)
but there was no distinguishable outlier in the funnel plot.
Therefore, we assumed heterogeneity to be real and ran a
random-effect analysis (Figure 3).
Figure 3. Forest plots and funnel plot. Meta-analysis showing the effects of pancreatic stent placement for hyperamylasemia.
Abdominal pain
Our results showed that 47 of the 399 patients in
pancreatic stenting group developed abdominal pain
compared to 69 of the 338 patients in the no-stent group (11.7% vs. 20.4%). The meta-analysis showed no statistical
difference (p<0.08) between groups (RD-0.10, 95% CI-0.21
0.01). Again, we identified high heterogeneity (I2=67%)
but no study was distinguishable as an outlier after funnel
plot analysis. Therefore, we assumed true heterogeneity
and performed a random-effect analysis (Figure 4).
Figure 4. Meta-analysis showing the effects of pancreatic stent placement for abdominal pain.
Cholangitis
Only 2 of the 67 patients (2.9%) in the pancreatic
stenting group presented post-ERCP cholangitis versus
none among the 74 patients in the no-stent group. The
meta-analysis showed no difference (p<0.29) between
groups (RD -0.03, 95% CI-0.03 0.09) and low heterogeneity
(I2=0%) (Figure 5).
Figure 5. Meta-analysis showing the effects of pancreatic stent placement for cholangitis.
Duration of ERCP
The comparison regarding the total duration of ERCP
was highly homogenous (I2=0%) and showed no difference
between pancreatic stenting and no-stent group (p<0.07)
(RD 2.97, 95% CI−0.19 6.12) (Figure 6).
Figure 6. Meta-analysis showing the effects of pancreatic stent placement for duration of ERCP.
Length of stay
The length of stay was similar between groups
(p>0.05) with mean difference of -1.55 (95% CI-4.39 1.29).
The meta-analysis showed high heterogeneity (I2=99%)
but since only two trial assessed length of stay, a single
exclusion would impair the pooled analysis (Figure 7). Therefore, we assumed it as true heterogeneity and
performed a random-effect analysis.
Figure 7. Meta-analysis showing the effects of pancreatic stent placement for length of hospital stay.
DISCUSSION
ERCP is central for the treatment of several biliary
and pancreatic diseases. However, the endoscopic
manipulation may impair the normal flow of the pancreatic
duct and activate intracellular proteolytic enzymes. Also, it
may cause bacterial contamination which results in chemical
pancreatic injury. All those factors trigger pancreatitis [3, 4].
Pancreatitis is the most common adverse event of
ERCP. PEP increases morbidity and mortality significantly,
especially in severe cases. Likewise, it carries increased
length of stay, which raises associated costs. The reported
incidence of PEP ranges from 2% to 30% [4, 12, 13, 14, 15, 16]. This wide variation is due to differences in patient
selection and procedure-related risk factors. Risk factors
for PEP include female gender, age ˂60 years, previous
history of PEP, pancreatic sphincterotomy, sphincter of
Oddi dysfunction, difficult cannulation, long duration of
procedure, pancreatic duct biopsy and less experienced
endoscopist [17, 18].
Several drugs and techniques have been investigated to
avoid PEP [18, 19, 20] and the pancreatic stenting is one of
the most robust in terms of available evidence. The stent
may assure the pancreatic flow in case of papillary edema or sphincter spasms caused by the endoscopic manipulation.
Possibly, this is the mechanism of action through which the
pancreatic stent effectively prevent PEP [3, 16].
The trials included in our meta-analysis showed that
pancreatic stenting reduced the risk of mild and moderate
pancreatitis. This data is in accordance with previous
meta-analyses [3, 13, 19, 20, 21, 22, 23]. However, our
study demonstrated that such intervention does not affect
the incidence of severe PEP, even though there was a subtle
trend toward risk decrease. Possibly, the tiny severe PEP
incidence might explain the lack of statistical difference
between groups. Therefore, further and larger studies
might change this statement.
In addition, pancreatic stenting reduced the incidence
of post-ERCP hiperamylasemia. This result goes according
to with from previous meta- analyses [13, 23, 24, 25, 26].
these results support the claim that post-ERCP pancreatic
stent prevents pancreatitis.
Regarding abdominal pain, we showed that pancreatic
stenting group was similar to no-stent group, and the
difference was not statistically significant. It should be noted that abdominal pain is one of the criteria to define
acute pancreatitis and, once diagnosed, patients have a
longer hospital stay and costs increase proportionally.
This result goes according to with from previous
meta- analyses [27, 28, 29]. Moreover, the analysis
of cholangitis as a post-ERCP, showed no difference
between groups. The heterogeneity between the trials
was low. This data is in accordance with previous metaanalyses
[6, 26, 30, 31].
The mean duration of ERCP was longer in the pancreatic
stent group than in the no-stent group; however, there
was no statistical significance. Although the insertion of
a pancreatic stent reduces PEP incidence, it is important
to note that it is a challenging procedure. Difficulties may
arise in the identification and cannulation of the pancreatic
duct ostium, and the progression of the guidewire and the
pancreatic stent itself in the duct lumen may be complex, with
increasing local manipulation and duration of the procedure.
The mean length of hospital stay was shorter in the
pancreatic stent group than in the no-stent group; however,
there was no statistical significance. Because there was no stratification in the length of hospital stay, it was not possible
to evaluate or predict costs; therefore, prospective studies
focusing on this topic should ideally be performed.
Our study has some limitations. The first we could not
evaluate the risk of post-ERCP pancreatitis in patients who
failed PD stent placement. Finally various lengths of stents
were used, which may result in evaluation bias.
ERCP is an essential procedure for the treatment
of several pancreatobiliary disorders. In our study, we
demonstrated that the placement of pancreatic stents is
important because it prevents post-ERCP pancreatitis
(mild and moderate). In addition, no serious complications
were reported in individuals in the stent group. Thus, it is
assumed that post-ERCP pancreatic stent placement leads
to a reduction in morbidity, mortality, and possibly costs to
the health system.
CONCLUSION
Pancreatic stenting is effective in reducing the incidence
of mild and moderate post-ERCP acute pancreatitis in
high-risk patients.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- ASGE Standards of Practice Committee, Chandrasekhara V, Khashab
MA, Muthusamy VR, Acosta RD, Agrawal D, et al. Adverses event associated
with ERCP. Gastrointest Endosc 2017; 8:32-47. [PMID: 27546389]
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman DJ,
et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter
study. Gastrointest Endosc 2001; 54: 425–434. [PMID: 11577302]
- Fan JH, Qian JB, Wang YM, Shi RH, Zhao CJ. Updated meta-analysis
of pancreatic stent placement in preventing post-endoscopic retrograde
cholangiopancreatography pancreatitis. World J Gastroenterol 2012;
21:7577–7583. [PMID: 26140006]
- Shi QQ, Ning XY, Zhan LL, Tang GD, Lv XP. Placement of
prophylactic pancreatic stents to prevent post-endoscopic retrograde
cholangiopancreatography pancreatitis in high-risk patients: A metaanalysis.
World J Gastroenterol 2014; 20:7040–7048. [PMID: 24944500]
- Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher
PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J
Med 1996; 335: 909–918. [PMID: 8782497]
- Yin HK, Wu HE, Li QX, Wang W, Ou WL, Xia HH. Pancreatic stenting
reduces post-ERCP pancreatitis and biliary sepsis in high-risk patients: a
randomized, controlled study. Gastroenterol Res Pract 2016; 13:2655–
2668. [PMID: 27057161]
- Chahal P, Tarnasky PR, Petersen BT, Topazian MD, Levy MJ, Gostout
CJ, et al. Short 5Fr vs long 3Fr pancreatic stents in patients at risk for
post-endoscopic retrograde cholangiopancreatography pancreatitis. Clin
Gastroenterol Hepatol 2009; 7:834–839. [PMID: 19447196]
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis
JPA, et al. The PRISMA statement for reporting systematic reviews
and meta-analyzes of studies that evaluate health care interventions:
explanation and elaboration. J Clin Epidemiol 2009; 62: 1–34.
- Sherman S, Earle D, Bucksot L, Weber C, Gottlieb K, Lehman G.
Does leaving a main pancreatic duct stent in place reduce the incidence
of precut biliary sphincterotomy-induced pancreatitis? Randomized
prospective study. Am J Gastroenterol 1995; 90: 241.
- Patel R, Tarnasky PR, Hennessy WS. Does stenting after pancreatic
sphincterotomy reduce post-ERCP pancreatitis in patients with prior
biliary sphincterotomy’ preliminary results of a prospective randomized
study. Gastrointest Endosc 1999; 49. AB80.
- Pan XP, Dang T, Meng XM, Xue KC, Chang ZH, Zhang YP. Clinical study
on the prevention of post-ERCP pancreatitis by pancreatic duct stenting.
Cell Biochem Biophys 2011; 61:473–479. [PMID: 21739262]
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan
DJ, et al. Assessing the quality of reports of randomized clinical trials: is
blinding necessary? Control Clin Trials 1996; 17:1–12. [PMID: 8721797]
- Choudhary A, Bechtold ML, Arif M, Szary NM, Puli SR, Othman MO,
et al. Pancreatic stents for prophylaxis against post-ERCP pancreatitis:
a meta-analysis and systematic review. Gastrointest Endosc 2011; 73:
275–282. [PMID: 21295641]
- Sofuni A, Maguchi H, Mukai T, Kawakami H, Irisawa A, Kubota K, et al.
Endoscopic pancreatic duct stents reduce the incidence of post-endoscopic
retrograde cholangiopancreatography pancreatitis in high-risk patients. Clin
Gastroenterol Hepatol 2011; 9: 851–888. [PMID: 21749851]
- Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito
F, et al. Incidence rates of post-ERCP complications: a systematic survey
of prospective studies. Am J Gastroenterol 2007; 102: 1781–1788.
[PMID: 17509029]
- Bourke MJ, Costamagna G, Freeman ML. Biliary cannulation during
endoscopic retrograde cholangiopancreatography: core technique and
recent innovations. Endoscopy 2009; 41: 612–617. [PMID: 19588290]
- Cheng CL, Sherman S, Watkins JL, Barnett J, Freeman M, Geenen J,
et al. Risk factors for post-ERCP pancreatitis: a prospective multicenter
study. Am J Gastroenterol 2006; 101:139–147. [PMID: 16405547]
- Shah TU, Liddle R, Branch MS, Jowell P, Obando J, Poleski M. Pilot
study of aprepitant for prevention of post-ERCP pancreatitis in high risk
patients: a phase II randomized, double-blind placebo controlled trial.
JOP 2012; 13:514–518. [PMID: 22964958]
- Otsuka T, Kawazoe S, Nakashita S, Kamachi S, Oeda S, Sumida C, et al.
Low-dose rectal diclofenac for prevention of post-endoscopic retrograde
cholangiopancreatography pancreatitis: a randomized controlled trial. J
Gastroenterol 2012. [PMID: 22350703]
- Abdel Aziz AM, Lehman GA. Pancreatitis after endoscopic retrograde
cholangiopancreatography. World J Gastroenterol 2007; 13:2655–2668.
[PMID: 17569133]
- Tarnasky PR, Palesch YY, Cunningham JT, Mauldin PD, Cotton
PB, Hawes RH. Pancreatic stenting prevents pancreatitis after biliary
sphincterotomy in patients with sphincter of Oddi dysfunction.
Gastroenterol 1998; 115:1518–1524. [PMID: 9834280]
- Fazel A, Quadri A, Catalano MF, Meyerson SM, Geenen JE. Does a pancreatic
duct stent prevent post-ERCP pancreatitis? A prospective randomized study.
Gastrointest Endosc 2003; 57:291–294. [PMID: 12612504]
- He LX, Gong P, Bie LK. The pancreatic stents to prevent the high risk
patient s from post-ERCP pancreatitis: a metaanalysis. Zhonghua Xiaohua
Neijing Zazhi 2010; 27: 94-98.
- Kawaguchi Y, Ogawa M, Omata F, Ito H, Shimosegawa T, Mine T.
Randomized controlled trial of pancreatic stenting to prevent pancreatitis
after endoscopic retrograde cholangiopancreatography. World J
Gastroenterol 2012; 18:1635–1641. [PMID: 22529693]
- Lee TH, Moon JH, Choi HJ, Han SH, Cheon YK, Cho YD, et al.
Prophylactic temporary 3F pancreatic duct stent to prevent post-ERCP
pancreatitis in patients with a difficult biliary cannulation: a multicenter,
prospective, randomized study. Gastrointest Endosc 2012; 76: 578–585.
[PMID: 22771100]
- Sofuni A, Maguchi H, Itoi T, Katanuma A, Hisai H, Niido T, et al.
Prophylaxis of post-endoscopic retrograde cholangiopancreatography
pancreatitis by an endoscopic pancreatic spontaneous dislodgement
stent. Clin Gastroenterol Hepatol 2007; 5:1339–1346. [PMID: 17981247]
- Ito K, Fujita N, Noda Y, Kobayashi G, Obana T, Horaguchi J, et al. Can
pancreatic duct stenting prevent post-ERCP pancreatitis in patients who
undergo pancreatic duct guidewire placement for achieving selective
biliary cannulation? A prospective randomized controlled trial. J
Gastroenterol 2010; 45:1183–1191. [PMID: 20607310]
- Tsuchiya T, Itoi T, Sofuni A, Itokawa F, Kurihara T, Ishii K, et al.
Temporary pancreatic stent to prevent post-endoscopic retrograde
cholangiopancreatography pancreatitis: a preliminary, single-center,
randomized controlled trial. J Hepatobiliary Pancreat Surg 2007; 14:302–
307. [PMID: 17520207]
- Harewood GC, Pochron NL, Gostout CJ. Prospective, randomized,
controlled trial of prophylactic pancreatic stent placement for endoscopic
snare excision of the duodenal ampulla. Gastrointest Endosc 2005;
62:367– 370. [PMID: 16111953]
- Smithline A, Silverman W, Rogers D, Nisi R, Wiersema M, Jamidar P,
et al. Effect of prophylactic main pancreatic duct stenting on the incidence
of biliary endoscopic sphincterotomy-induced pancreatitis in high-risk
patients. Gastrointest Endosc 1993; 39:652–657. [PMID: 8224687]
- Cha SW, Leung WD, Lehman GA, Watkins JL, McHenry L, Fogel EL,
et al. Does leaving a main pancreatic duct stent in place reduce the
incidence of precut biliary sphincterotomy-associated pancreatitis? A
randomized, prospective study. Gastrointest Endosc 2013; 77: 209–216.
[PMID: 23084272]








