Keywords
Neurilemmoma; Pancreas; Radiotherapy
INTRODUCTION
Schwannomas are uncommon neoplasms. They typically arise from neural crest cells which encapsulate the nerve sheath and are sometimes also referred as neurilemmomas. Schwannomas usually occur in the extremities, but can also be found in the trunk, head and neck, retroperitoneum, mediastinum, pelvis and rectum [1]. Benign schwannomas comprise 65% of all neurogenic tumors; however 10-15% of these tumors are malignant [2, 3].
Pancreatic schwannomas are even more unusual neoplasms that affect adults with an equal gender distribution [4]. These tumors vary considerably in size and approximately two thirds are reported to undergo degenerative changes including cyst formation, calcification, hemorrhage, hyalinization and xanthomatous infiltration [5]. As a result, they may radiographically mimic cystic pancreatic lesions (e.g. pancreatic cystadenomas and cystadenocarcinomas and pancreatic pseudocysts), making a preoperative diagnosis a clinical challenge.
In the present report, we discuss a case of pancreatic schwannoma and provide a pertinent review of the literature with an emphasis on the clinical presentation, diagnostic modalities and treatment options in the management of this rare clinical entity.
CASE REPORT
A 69-year-old female presented to the hospital with progressive worsening left upper quadrant and epigastric pain for three weeks. Her pain was constant and ranged from moderate to severe and was associated with nausea and vomiting. The patient denied other constitutional symptoms such as weight loss or fever.
Her past medical history was unremarkable. The patient denied alcohol, tobacco or illegal drugs use. On physical examination, she was hemodynamically stable and afebrile. Her abdomen was soft, non-distended, without a palpable mass, but moderately tender to palpation in the epigastrium and left upper quadrant.
Laboratory tests demonstrated normal hemoglobin and hematocrit at 12.7 g/dL (reference range: 12.7-17.5 g/dL) and 37.3% (reference range: 39-49%), respectively. The chemistry panel, liver function tests and amylase were normal as were tumor markers cancer antigen 19-9 (CA 19-9: 10.7 U/mL; reference range: 5.0-37.0 U/mL) and carcinoembryonic antigen (CEA: 2.2 U/mL; reference range: 0-2.5 U/mL).
Dynamic computed tomography (CT) scans with 3-dimenional reconstruction of the abdomen and pelvis demonstrated a 5.0x4.4 cm mass at the pancreatic head with abutment of the superior mesenteric artery and portal vein confluence (Figures 1 and 2). Endoscopic ultrasound (EUS) and fine needle aspiration (FNA) of the mass demonstrated characteristic spindle cells, whorling appearance and strong immunoperoxidase staining with S-100 protein which were consistent with schwannoma. Clinical staging with CT scans and EUS demonstrated no lymph node involvement or metastasis. The patient was subsequently taken to the operating room for tumor resection.
Figure 1. a. CT scan demonstrated a pancreatic head
mass that abuts the superior mesenteric artery (black
arrow). b. Loculated cystic degeneration can also be
seen in the center of the tumor.
Figure 2. Delayed-phase CT scan (a.) with 3-D
reconstruction (b.) demonstrated tumor abutment at the
portal vein confluence (black arrows).
At laparotomy, a large retroperitoneal mass at the head of the pancreas was found to encase the superior mesenteric artery, and the portal vein confluence (Figure 3). No lymphadenopathy in the mesentery, peritoneal implants or liver lesion was found. Frozen biopsy confirmed benign schwannoma (Figures 4 and 5). Due to extensive vascular involvement and favorable tumor biology, the tumor was not completely resected. A gastrojejunostomy was then performed.
Figure 3. Tumor encasement of the portal vein
confluence. The SMA was also involved but very
fibrotic for safe mobilization.
Figure 4. Immunohistochemical stain with S100
protein antibody shows that the tumor cells are
diffusely and strongly positive (Avidin-biotinperoxidase
complex method, 10x).
Figure 5. The histologic section from the biopsy of this
pancreatic tumor reveals a long spindle cell
proliferation with eosinophilic neurofibliary
background. The nuclei are slender, slightly wavy, and
with pointed ends. Antoni A and B areas are both
evident. In this field of hypercellular area, palisading
nuclei are arranged in a palisading fashion (Verocay
body). (Hematoxylin and Eosin stain, 10x).
The patient’s post-operative course was unremarkable. She was discharged home on post-operative day number five and was scheduled for radiation therapy and CT scan surveillance. Curative resection will be offered if adjuvant therapy results in safe tumor resection.
DISCUSSION
Only 24 cases of pancreatic schwannoma have been reported in the English literature (Table 1) [6]. These tumors vary considerably in size ranging from 1.5 to 20.0 cm in diameter with the majority of the tumors located in the head (38%) and body (25%) of the pancreas. Schwannomas of the pancreas arise from Schwann cells encasing peripheral nerves and can be benign or malignant. Generally, pancreatic schwannomas have slow growth rates and usually originate from the peripheral epineurium of either autonomic sympathetic or parasympathetic fibers, which embryologically course through the pancreas via the vagus nerve [7].
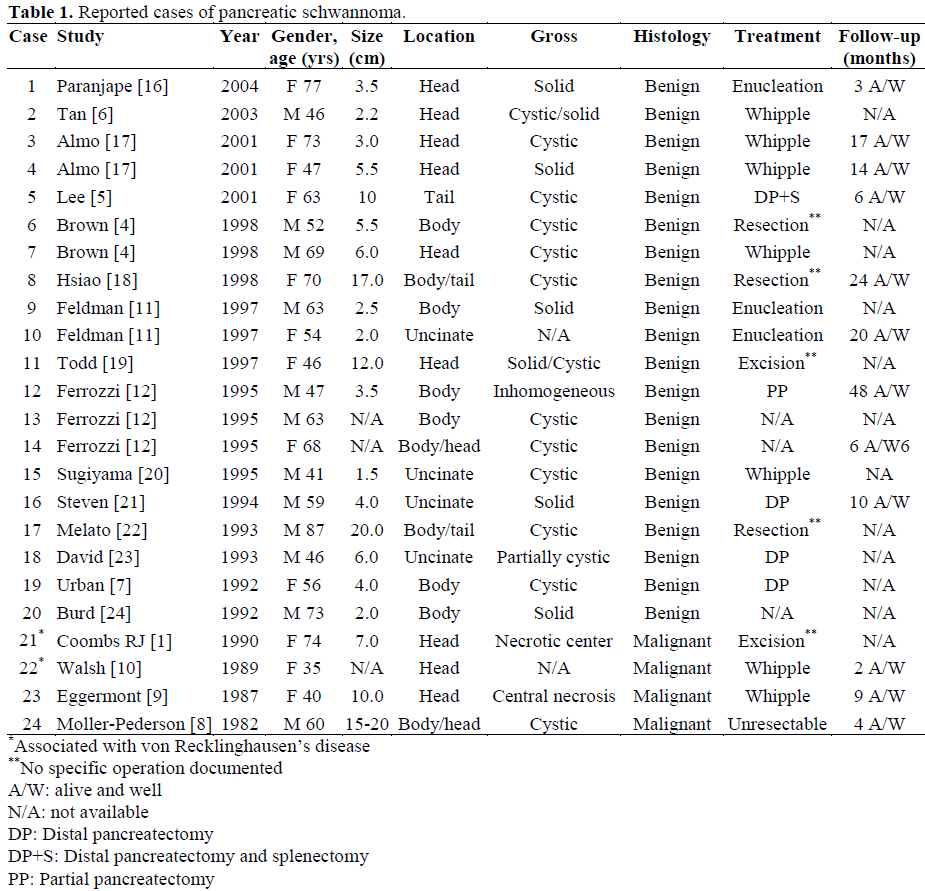
As depicted in Table 1, more than half of the reported schwannomas are cystic and 83% are benign. Malignant pancreatic schwannomas, albeit uncommon, have been reported in four cases [1, 8, 9, 10]. Malignant transformation is associated with von Recklinghausen’s disease in 8% of cases [1, 10].
Non-specific abdominal pain was the most commonly reported symptoms but weight loss, jaundice and gastrointestinal bleeding had been reported [8, 9, 10]. The preoperative diagnosis of schwannoma presents a clinical challenge and CT scan is often the initial study of choice to establish a pancreatic lesion. CT findings in pancreatic schwannomas, however, are typically similar to non-pancreatic schwannomas and usually demonstrate well-defined and hypodense tumors with encapsulation and cystic degeneration [11]. Degenerative changes with cyst formation pose a formidable diagnostic challenge because they mimic the whole spectrum of cystic pancreatic lesions including: neuroendocrine tumors, cystadenoma, cystadenocarcinoma, intraductal papillary mucinous tumor, lymphangiomas and pancreatic pseudocysts [6].
Once a pancreatic lesion has been determined, magnetic resonance imaging (MRI) is helpful in characterizing schwannomas by their typical encapsulation, hypointensity on T1- weighted images and hyperintensity on T2 [11, 12]. In addition to variable signal intensities, MRI may reveal vascular involvement which can further characterize a lesion with malignant potential [11]. MRI may also differentiate pancreatic schwannoma from adenocarcinoma by the characteristic hyperintensity on T2 weighted images and marked enhancement of the lesion in comparison with the remainder of the gland [11]. However, further differentiation from islet cell tumors cannot be established by this modality [11].
Further characterization of a pancreatic mass may be established by EUS-guided FNA. However, the diagnosis of pancreatic schwannoma by FNA may be complicated by inadequate amount of specimen or by inherent specimen collecting techniques. A recent study demonstrated that FNA correctly diagnosed only one out of eight histologically proven schwannomas [13].
Although pre-operative radiographic imaging may help narrow the differential diagnosis, pancreatic schwannoma is usually diagnosed at the time of laparotomy, followed by histological analysis [4, 6, 11]. Microscopically, schwannomas stain strongly positive for S-100 protein, vimentin and CD56 while negative for other tumor markers including cytokeratin AE1/AE3, desmin, smooth muscle myosin, CD34 and CD117 (Figure 4) [6]. On histological analysis, schwannomas have two different patterns which are designated as Antoni A and B. Antoni A refers to areas that are highly cellular and composed of spindle cells arranged in a palisading fashion without mitotic figures, while Antoni B areas are typically hypocellular with degenerative changes (Figure 5) [6].
Since malignant transformation of pancreatic schwannomas is uncommon, simple enucleation is usually sufficient even though oncologic resections (Whipple’s procedure and distal pancreatectomy) had been reported (Figure 6). To date, no documented recurrent case has been reported for either mode of resection. In the present case, the tumor was found to encase the superior mesenteric artery as well as the portal vein confluence with severe associated inflammation and fibrosis of the surrounding tissues. Curative surgical resection was thus deemed high risk.
Figure 6. Operative management of pancreatic
schwannomas.
Review of the literature shows one reported case of unresectable tumor, but no report of previous treatment with chemoradiation therapy [8]. However, radiation therapy has been shown to decrease tumor growth and regression in neurogenic schwannomas [14, 15]. Because schwannomas share similar biological characteristics, it is conceivable that radiation therapy would have similar effects in pancreatic schwannomas as with neurogenic schwannomas. However, the role of radiation therapy in the management of pancreatic schwannomas is still unclear. Surgical excision with close follow up and surveillance remain the mainstay of treatment.
CONCLUSION
Pancreatic schwannoma, albeit rare, is an important clinical entity to include in the differential diagnosis of pancreatic lesions, especially when cyst formation was demonstrated on radiologic imaging. Preoperative diagnosis is difficult but CT and MRI help raise the suspicion of this diagnosis. Definitive diagnosis, however, requires histological examination. Simple enucleation is usually adequate for benign tumors while malignant tumors require standard oncologic resection. The role of radiation therapy in the management of unresectable tumors is still unclear and therapeutic effectiveness remains to be seen.
References
- Coombs RJ. Case of the season. SeminRoentgenol 1990; 25:127-9. [PMID 2112269]
- Kawarada Y, Isaji S. Modified standard (D1+alpha) pancreaticoduodenectomy for pancreatic cancer. J Gastrointest Surg 2000; 4:227-8. [PMID 10939864]
- DeVita VT Jr, Helman S, Rosenberg SA. Cancer: Principles and Practice of Oncology. 3rd ed. Philadelphia, PA, USA: JB Lippincott, 1989:721.
- Brown SZ, Owen DA, O’Connell JX, Scudamore CH. Schwannoma of the pancreas: a report of two cases and a review of the literature. Mod Pathol 1998; 11:1178-82. [PMID 9872648]
- Lee JS, Kim HS, Jung JJ, Han SW, Kim YB. Ancient schwannoma of the pancreas mimicking a cystic tumor: case report and literature review. Virchows Arch 2001; 439:697-9. [PMID 11764392]
- Tan G, Vitellas K, Morrison C, Frankel WL. Cystic schwannoma of the pancreas. Ann Diagn Pathol 2003; 7:285-91. [PMID 14571430]
- Urban BA, Fishman EK, Hruban RH, Cameron JL. CT findings in cystic schwannoma of the pancreas. J Comput Assist Tomogr 1992; 16:492-3. [PMID 1592939]
- Moller-Pedersen VM, Hedes A, Giraem N. A solitary malignant schwannoma mimicking a pancreatic pseudocys. Acta ChirScand 1982; 148:697- 8. [PMID 7170905]
- Eggermont A, Vuzeuski V, Huisman M, DeJang K, Jeekel J. Solitary malignant schwannoma of the pancreas: report of a case and ultrastructural examination. J Surg Oncol 1987; 36:21-5. [PMID 3626558]
- Walsh MM, Brandspigel K. Gastrointestinal bleeding due to pancreatic schwannoma complicating von Recklinghausen’s disease. Gastroenterology 1989; 97:1550-1. [PMID 2511055]
- Feldman L, Philpotts LE, Reinhold C, Duguid WP, Rosenberg L. Pancreatic schwannoma: report of two cases and review of the literature. Pancreas 1997; 15:99-105. [PMID 9211499]
- Ferrozzi F, Bova D, Garlaschi G. Pancreatic schwannoma: report of three cases. Clin Radiol 1995; 50:492-5. [PMID 7614798]
- Yu GH, Sack MJ, Balock Z, Guptua PK. Difficulties in the fine needle aspiration (FNA) diagnosis of schwannoma. Cytopathology 1999; 10:186-94. [PMID 10390067]
- Prasad D, Jalali R, Shet T. Intracranial subfrontalschwannoma treated with surgery and 3D conformal radiotherapy. Neurol India 2004; 52:248-50. [PMID 15269484]
- Sawamura Y, Shirato H, Sakamoto T, Aoyama H, Suzuki K, Onimaru R, et al. Management of vestibular schwannoma by fractionated stereotactic radiotherapy and associated cerebrospinal fluid malabsorption. J Neurosurg 2003; 99:685-92. [PMID 14567604]
- Paranjape C, Johnson SR, Khwaja K, Goldman H, Kruskal JB, Hanto DW. Clinical characteristics, treatment, and outcome of pancreatic schwannomas. J Gastrointest Surg 2004; 8:706-12. [PMID 15358332]
- Almo KM, Traverso LW. Pancreatic schwannoma: an uncommon but important entity. J Gastrointest Surg 2001; 5:359-63. [PMID 11985975]
- Hsiao WC, Lin PW, Chang KC. Benign retroperitoneal schwannoma mimicking a. pancreatic cystic tumor: case report and literature review. Hepatogastroenterology 1998; 45:2418-20. [PMID 9951935]
- Todd KE, Lewis MPN, Gloor B, Ashley SW, Reber HA. Management decisions for unusual periampullary tumors. Am Surg 1997; 63:927-32. [PMID 9322675]
- Sugiyama M, Kimura W, Kuroda A, Muto T. Schwannoma arising from peripancreatic nerve plexus. AJR Am J Roentgenol 1995; 164:232. [PMID 7785620]
- Steven K, Burcharth F, Holm N, Pederson IK. Single stage pancreaticoduodenectomy (Whipple’s procedure), radical cystectomy and bladder substitution with the urethral kock reservoir. Scand J Urol Nephrol 1994; 25:385-7. [PMID 7939474]
- Melato M, Bucconi S, Marus W, Spivach A, Perulli A, Mucelli RP. The schwannoma: an uncommon type of cystic lesion of the pancreas. Ital J Gastroenterol 1993; 25:385-7. [PMID 8280901]
- David S, Barkin JS. Pancreatic schwannoma. Pancreas 1993; 8:274-6. [PMID 8460103]
- Burd DA, Tyagi G, Bader DA. Benign schwannoma of the pancreas. AJR Am J Roentgenol 1992; 159:675. [PMID 1503050]







