Keywords
Pancreas; Pancreatectomy Pancreatic Neoplasms; Teratoma; Wounds and Injuries
INTRODUCTION
Solid-pseudopapillary tumors of the pancreas account for less than 4% of pancreatic cystic tumors [1]. They are composed of homogeneous, fleshy tissue separated by areas of hemorrhagic and necrotic cyst degeneration [2] and are believed to have an acinar origin [2]. Many tumors are detected incidentally, but may occasionally present with sudden pain due to bleeding within the tumor or with symptoms related to the compression of adjacent organs [3]. It is almost exclusively encountered in young females having a mean age of 26 years and has a male to female ratio of 1:9 [3, 4]. Therefore, solid-pseudopapillary tumors are exceedingly rare in males and only a few cases have been reported in children [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. We report a case of a young boy presenting with this rare pancreatic tumor and discuss the diagnostic dilemma and the malignant potential of such tumors.
CASE REPORT
A 12-year-old Saudi boy presented with a 2- day history of left upper quadrant pain, which started following a slight trauma to his abdomen and was associated with nausea and vomiting. Initially, he denied any history of trauma and there was no history of weight loss or preexisting abdominal swellings. There was neither history of sickle cell disease nor any other hemolytic anemias. On examination, he looked ill, dehydrated and pale but there was no jaundice or lymphadenopathy. His vital signs were stable, and chest and cardiovascular systems were normal. Abdominal examination revealed a tender abdominal mass occupying the epigastrium and left hypochondrium, with guarding and rigidity. Blood investigations revealed a hemoglobin of 9.6 g/dL (reference range: 12-16 g/dL), a leukocytosis of 13.6 x109/L (reference range: 3.5-10.0 x109/L) and normal amylase, lipase and liver function tests. Emergency abdominal ultrasound and computerized tomography (CT) scans revealed a mixed attenuated round mass (9.2x9.3 cm) at the body and the tail of the pancreas, possibly a complicated pseudocyst with a normal liver and spleen (Figure 1). Soon after admission, he became pyrexial with persistent tenderness and rigidity. Repeated investigation revealed a leukocytosis of 30,000 mm-3 and a normal amylase level. An emergency laparotomy was performed using a roof-top incision. There was free blood in the peritoneal cavity and a huge retroperitoneal mass arising from the body and the tail of the pancreas with bleeding coming from a small laceration in its wall. Distal pancreatectomy and splenectomy were performed (Figure 2). His postoperative recovery was uneventful and he was given pneumococcal and Haemophilus influenzae vaccines before he was discharged a week later. The histopathologic examination revealed a solid-pseudopapillary tumor of the pancreas (Figures 3 and 4). He has remained well after a 3-year follow-up with no evidence of recurrence on repeated abdominal CT scan.
Figure 1. The ACT scan of the abdomen showing the cystic lesion arising from the tail of the pancreas with a normal
pancreatic parenchyma.
Figure 2. A macrograph of the resected operative
specimen showing the tumor at the tail of the pancreas
and the spleen. The hemorrhagic contents are also
shown.
Figure 3. A micrograph showing cystic degeneration
with solid and pseudopapillary formations and red
blood cells in the cystic space. (H&E stain. x100)
Figure 4. Tumor cells radially arranged around fibrovascular
stalks forming rosette-like patterns. (H&E
stain. x400)
DISCUSSION
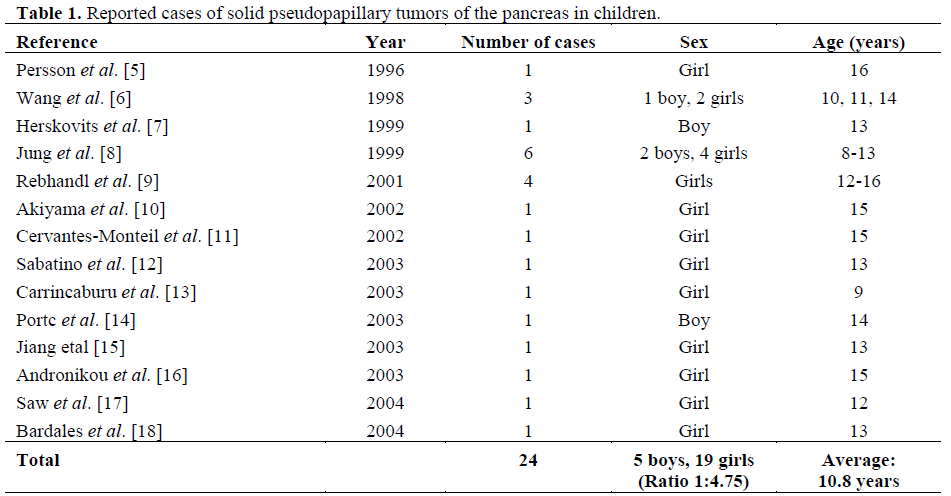
Solid-pseudopapillary tumors of the pancreas are very rare and almost exclusively encountered in young females (mean age 26 years) as genetic and hormonal factors may play an important role in their development [3, 4, 18, 19]. The tumor is exceedingly rare in males [3, 20, 21, 22]. In one review, there was only one male among 31 patients [3]. Review of the literature revealed some 24 cases of solid-pseudopapillary tumors of the pancreas reported in children (Table 1) with an average age of 10.8 years (range 8-16 years) and a male:female ratio of 1:4.75 [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. There were 4 cases (3 girls and a boy) 13-16 years of age presented acutely following blunt abdominal trauma in a fashion similar to that of our present case [5, 11, 14, 15] An emergency Whipple procedure was performed in 3 cases [11, 13, 15]. Bombi et al. reported another 2 cases of pseudopapillary tumors in older female patients 22 and 23 years of age [2]; one presented with an acute abdomen and pneumoperitoneum. This presentation was also somewhat similar to that of our patient whose tumor was the result of a slight trauma which had already been forgotten and was initially denied causing a diagnostic dilemma.
Patients are often asymptomatic and the cyst is discovered incidentally on physical or radiological examination [3]. Patients may also occasionally present with an increasing abdominal mass associated with vague abdominal discomfort or may rarely present with an acute abdomen due to tumor rupture and hemoperitoneum as happened in our patient. Jung et al. reported a series of 6 pediatric cases (4 girls and 2 boys) with a mean age of 11.2 years (range 8-13 years); 5 of the lesions were located in the head necessitating pancreaticoduodenectomy and one was located in the tail which was treated by distal pancreatectomy [8]. All were alive with no recurrence at an average follow-up of 5.5 years. Wang et al. reported a solidpseudopapillary tumor in 3 children (2 girls 11 and 14 years of age and a boy 10 years of age) and concluded that the tumor arises early in life, grows slowly and rarely metastasizes [6]. Another presentation of a solidpseudopapillary tumor is acute pancreatitis with an abdominal mass [23]. Rebhandl et al. reported the cases of 4 girls 12-16 years of age presenting with abdominal pain and masses (diameter 7-15 cm); located in the tail (n=2), the body and tail (n=1) and the head (n=1). Only one patient developed two recurrences and metastases after surgical resection despite receiving chemotherapy [9].
In our case, a CT scan raised the possibility of a complicated pancreatic pseudocyst (either infected or bleeding within), but amylase and lipase levels were within normal limits. Furthermore, the rest of the pancreas looked normal with no evidence of pancreatitis in the CT scan. It was noted that magnetic resonance imaging (MRI) is superior to CT for diagnosing these tumors [20, 24, 25]. An MRI was not requested in this case but, at laparotomy, the mass had a mature thick true wall, easily separable from the posterior wall of the stomach and was therefore thought to be a cystadenoma or a cystadenocarcinoma rather than a pseudocyst of the pancreas. Drainage of this cystic tumor in the stomach or jejunum would have resulted in disastrous consequences of local invasion and possible future metastases. The option of distal pancreatectomy and splenectomy offered a complete cure and settled this diagnostic dilemma. This procedure can be conducted laparoscopically and laparoscopic spleenpreserving distal pancreatectomy for solidpseudopapillary tumor has been reported [13]. The role of endoscopic ultrasound-guided fine needle aspiration in accurately diagnosing solid-pseudopapillary tumors is now wellestablished [18, 26, 27, 28, 29]. This usually demonstrates low levels of carcinoembryonic antigen and a moderate elevation in cyst fluid carbohydrate antigen 19-9 and lipase and the cyst fluid cytology may be diagnostic [29]. Extensive necrosis and rare mitotic figures may be present. Solid-pseudopapillary tumors of the pancreas show strong cellular immunoreactivity for vimentin and focal weak keratin reactivity. Neuron-specific enolase, alpha1-antitrypsin, and alpha1- antichymotrypsin stains, if carried out, may be strongly positive [18, 29]. US-guided FNA was not carried out in our case due to the acute presentation.
Solid-pseudopapillary tumors possess a malignant potential risk of 5-10% and must therefore be resected completely and aggressively as there are no prognostic factors to distinguish between pseudopapillary tumors with or without malignant potential [3, 30]. Unlike pancreatic ductal adenocarcinoma, surgical resection often results in cure and long disease-free periods even in patients who have recurrences or metastases [31]. One series reported a 100% survival after an average 10-year follow-up [32]. However, anything short of surgical resection (e.g. internal or external drainage) is associated with tumor progression locally and invasion of the surrounding structures and distant metastases [33]. Even in the presence of advanced local invasion, palliative resection is advised and offers an excellent prognosis and survival benefits [4, 31, 34]. After resection, only a small number recur or develop metastases. However, subsequent visceral metastases after incomplete resection of a pseudopapillary tumor following a prolonged period of observation have been reported [4, 16, 35, 36]. Nevertheless, the growth of a recurrent tumor is very slow. Our patient has had a relatively short follow-up period (just over 3 years); until now there has been no evidence of recurrence or distant metastases. It seems that tumors arising in children are low grade, grow very slowly, rarely metastasize and have a good prognosis [6, 8]. This low-grade malignant potential manifests itself by invasion of the capsule and neighboring structures [3]. Macroscopically, they are well-circumscribed tumors which contain solid and cystic areas consisting of hemorrhagic and central cystic necrosis. This often gives a characteristic CT appearance which aids diagnosis and allows differentiation from islet cell tumors [32, 37]. Our case was erroneously diagnosed as a complicated pseudocyst based on CT scan findings.
In conclusion, this case report emphasizes the fact that solid-pseudopapillary tumors of the pancreas may arise in male children, and that it may cause diagnostic confusion especially in children with asymptomatic lesions who may present acutely following trauma. Increased awareness of this tumor allows appropriate emergency management to be undertaken.
References
- Fernandez-Del Castillo C, Warshaw AL. Cystic tumors of the pancreas. Surg Clin North Am 1995; 75:1001-16. [PMID 7660245]
- Bombi JA, Milla A, Badal JM, Piulachs J, Estape J, Cardesg A. Papillary-cystic neoplasm of the pancreas: report of two cases and review of the literature. Cancer 1984; 54:780-4. [PMID 6744212]
- Kloppel G, Kosmahl M. Cystic lesions and neoplasms of the pancreas. The features are becoming clearer. Pancreatology 2001; 1:648-55. [PMID 12120249]
- Kaufman SL, Reddick RL, Stiegel M, Wild RE, Thomas CG Jr. Papillary cystic neoplasm of the pancreas: a curable pancreatic tumor. World J Surg 1986; 10:851-9. [PMID 3022489]
- Persson M, Bisgaard C, Nielsen BB, Christiansen T, Kroustrup JP. Solid and papillary epithelial neoplasm of the pancreas presenting as a traumatic cyst. Case report. Acta ChirScand 1986; 152:223-6. [PMID 3716743]
- Wang KS, Albanese C, Dada F, Skarsgard ED. Papillary cystic neoplasm of the pancreas: a report of three pediatric cases and literature review. J Pediatr Surg 1998; 33:842-5. [PMID 9660210]
- Herskovits M, Cohen I, Loberant N, Szvalb S. Papillary cystic neoplasm of the pancreas in a teenage boy. Eur Radiol 1999; 9:1354-6. [PMID 10460373]
- Jung SE, Kim DY, Park KW, Lee SC, Jang JJ, Kim WK. Solid and papillary epithelial neoplasm of the pancreas in children. World J Surg 1999; 23:233-6. [PMID 9933691]
- Rebhandl W, Felberbauer FX, Puig S, Paya K, Hochschorner S, Barlan M, Horcher E. Solidpseudopapillary tumor of the pancreas (Frantz tumor) in children: report of four cases and review of the literature. J Surg Oncol 2001; 76:289-96. [PMID 11320522]
- Akiyama H, Ono K, Takano M, Sumida K, Ikuta K, Miyamoto O. Solid-pseudopapillary tumor of the pancreatic head causing marked distal atrophy: a tumor originated posterior to the main pancreatic duct. Int J Gastrointest Cancer 2002; 32:47-52. [PMID 12630770]
- Cervantes-Monteil F, Florez-Zorrilla C, Alvarez- Martinez I. Solid-cystic pseudopapillary tumor of the pancreas: acute post-traumatic presentation. Case report and review of the literature. Rev Gastroenterol Mex 2002; 67:93-6. [PMID 12214341]
- Sabatino D, Kosuri S, Quiles R. Solid and papillary epithelial neoplasm of the pancreas in an 11- year-old girl: case report and literature review. PediatHematol Oncology 2003; 20:357-60. [PMID 12775532]
- Carricaburu E, Enezian G, Bonnard A, Berrebi D, Belarbi N, Huot O, et al. Laparoscopic distal pancreatectomy for Frantz's tumor in a child. Surg Endosc 2003; 17:2028-31. [PMID 14598158]
- Potrc S, Kavalar R, Horvat M, Gadzijev EM. Urgent Whipple resection for solid pseudopapillary tumor of the pancreas. J HepatobiliaryPancreat Surg 2003; 10:386-9. [PMID 14598141]
- Jiang J, Gonzalez M, Hartman GG. Pathologic quiz case: a 13-year-old girl with an abdominal mass following trauma. Solid-pseudopapillary carcinoma of the pancreas. Arch Pathol Lab Med 2003; 127:e399- 401. [PMID 12951995]
- Andronikou S, Moon A, Ussher R. Peritoneal metastatic disease in a child after excision of a solid pseudopapillary tumour of the pancreas: a unique case. Pediatr Radiol 2003; 33:269-71. [PMID 12709760]
- Saw HP, Ho ML, Chen JY. Solid cystic pseudopapillary tumor of the pancreas: report of one case. Acta Paediatr Taiwan 2003; 44:368-71. [PMID 14983661]
- Bardales RH, Centeno B, Mallery JS, Lai R, Pochapin M, Guiter G, et al. Endoscopic ultrasoundguided fine-needle aspiration cytology diagnosis of solid-pseudopapillary tumor of the pancreas: a rare neoplasm of elusive origin but characteristic cytomorphologic features. Am J Clin Pathol 2004; 121:654-62. [PMID 15151205]
- Pezzi CM, Schuerch C, Erlandson RA, Deitrick J. Papillary-cystic neoplasm of the pancreas. J Surg Oncol 1988; 37:278-85. [PMID 3283458]
- Levy C, Pereira L, Dardarian T, Cardonick E. Solid-pseudopapillary pancreatic tumor in pregnancy. A case report. J Reprod Med. 2004; 49:61-4. [PMID 14976799]
- Ng KH, Tan PH, Thng CH, Ooi LL Solidpseudopapillary tumour of the pancreas. ANZ J Surg. 2003; 73:410-5. [PMID 12801340]
- Mancini GJ, Dudrick PS, Grindstaff AD, Bell JL. Solid-pseudopapillary tumor of the pancreas: two cases in male patients. Am Surg 2004; 70:29-31. [PMID 14964542]
- Sakagami J, Kataoka K, Sogame Y, Taii A, Ojima T, Kanemitsu D, et al. Solid pseudopapillary tumor as a possible cause of acute pancreatitis. JOP. J Pancreas (Online) 2004; 5:348-52. [PMID 15365201]
- Buetow PC, Buck JL, Pantongrag-Brown L, Beck KG, Ros PR, Adair CF. Solid and papillary epithelial neoplasm of the pancreas: imaging pathologic correlation in 56 cases. Radiology 1996; 199:707-11. [PMID 8637992]
- Cantisani V, Mortele KJ, Levy A, Glickman JN, Ricci P, Passariello R, et al. MR imaging features of solid pseudopapillary tumor of the pancreas in adult and pediatric patients. AJR Am J Roentgenol 2003; 181:395-401. [PMID 12876017]
- Mergener K, Detweiler SE, Traverso LW. Solidpseudopapillary tumor of the pancreas: diagnosis by EUS-guided fine-needle aspiration. Endoscopy 2003; 35:1083-4. [PMID 14648429]
- Master SS, Savides TJ. Diagnosis of solidpseudopapillary neoplasm of the pancreas by EUSguided FNA. GastrointestEndosc 2003; 57:965-8. [PMID 12776058]
- Pettinato G, Di Vizio D, Manivel JC, Pambuccian SE, Somma P, Insabato L. Solid-pseudopapillary tumor of the pancreas: a neoplasm with distinct and highly characteristic cytological features. DiagnCytopathol 2002; 27:325-34. [PMID 12451561]
- Ashton J, Sutherland F, Nixon J, Nayak V. A case of solid-pseudopapillary tumor of the pancreas: preoperative cyst fluid analysis and treatment by enucleation. Hepatogastroenterology 2003; 50:2239- 41. [PMID 14696507]
- Le Borgne J. Cystic tumours of the pancreas. Br J Surg 1998; 85:577-9. [PMID 9635798]
- Kato T, Egawa N, Kamisawa T, Tu Y, Sanaka M, Sakaki N. A case of solid pseudopapillary neoplasm of the pancreas and tumor doubling time. Pancreatology 2002; 2:495-8. [PMID 12378119]
- Zinner MJ, Shurbaji MS, Cameron JL. Solid and papillary epithelial neoplasms of the pancreas. Surgery 1990; 108:475-80. [PMID 2396191]
- Hyde GL, Davis JB, McMillin RD, McMillin M. Mucinous cystic neoplasm of the pancreas with latent malignancy. Am Surg 1984; 50:225-9. [PMID 6712017]
- Sanfey H, Mendelsohn G, Cameron JL. Soild and papillary neoplasm of the pancreas: A potentially curable surgical lesion. Ann Surg 1983; 197:272-6. [PMID 6830334]
- Matsuda Y, Imai Y, Kawata S, Nishikawa M, Miyoshi S, Saito R. Papillary-cystic neoplasm of the pancreas with multiple hepatic metastases: a case report. Gastroenterol Jpn 1987; 22:370-84. [PMID 2442059]
- Warshaw AL, Rutledge PL. Cystic tumors mistaken for pancreatic pseudocysts. Ann Surg 1987; 205:393-8. [PMID 3566376]
- McCormick FCS, Stamp GWH. Cystic neoplasms of the pancreas. Surgery 1998; 124 (Suppl. 16):84a.





