Keywords
Case Management; Causality; Epidemiology; Hospital Distribution Systems; Pancreatic Pseudocyst; Pancreatitis; Pancreatitis, Acute Necrotizing; Pancreatitis, Alcoholic; Pathology; Sanitation
INTRODUCTION
The widespread application of ultrasonography and CT has advanced our knowledge of the natural history of pancreatic pseudocysts. It is generally agreed that acute and chronic pseudocysts have a different natural history, although many reports do not differentiate between pseudocysts which complicate acute pancreatitis and those which complicate chronic disease [1]. This makes evaluation of different treatment options difficult or impossible. Also, the treatment evaluation is complicated due to the tendency towards spontaneous resolution of the pseudocysts.
The quality of data about spontaneous resolution of acute pseudocysts varies from study to study and, when there is no precise definition of the pseudocyst and when alcohol is the major cause, selection bias can occur which threatens the reliability of the results. Nevertheless, the results from published studies allow us to draw some limited conclusions and to raise questions which require further investigation.
Possible Mechanisms of Spontaneous Resolution
There are few, if any, reliable data on the mechanisms of spontaneous resolution of pancreatic pseudocysts. The only documented method is the spontaneous rupture of a pancreatic pseudocyst into the adjacent organs [2, 3]. The other supposed mechanisms are merely based on speculation rather than fact. Since resolution, when it does take place, seems to be complete within a few days, it may be unlikely that anterior transmural absorption is taking place in the absence of peritoneal signs of the development of ascites. A theoretical possibility is that, in such cases, drainage into the extrapancreatic retroperitoneal tissues as well as internal drainage through the pancreatic ductal system after clearance of a temporary obstruction of the duct may take place [4].
In a study of the mechanism of ductal drainage of the pancreas [5], plugs of precipitated proteinaceous material were demonstrated in the pancreatic ducts of patients with chronic pancreatitis. If the proteinaceous plugs become resolved or dislodged, the pseudocyst may drain into the ductal system. Once resolution of the pseudocyst begins, it is usually complete within a short time. However, since there is fibrosis and scarring of the ductal system in chronic pancreatitis, expectation of spontaneous resolution of chronic pseudocysts is quite low [6].
Resolution of Acute Pseudocysts
Earlier studies suggest that spontaneous resolution of an acute pseudocyst occurred in 8-70% of patients [2, 6, 7, 8, 9], i.e. the span of results is so wide that it is only possible to draw one conclusion: spontaneous resolution occurs. However, some important limitations are present in these studies. When the diagnosis is based on clinical presentation, barium meal study or angiography, one can expect that acute fluid collections and real pancreatic pseudocysts are mixed in one group. The more patients with diagnosed acute pseudocysts who actually have acute fluid collections, the higher the resolution rate is. As an example, in a prospective study [9], which inferred the presence of pancreatic pseudocysts from barium meal studies or angiography, 104 cases of acute alcoholic pancreatitis were evaluated. In 11% of the patients, the abdominal mass persisted and was considered to be a pancreatic pseudocyst. Over 70% of 11 pseudocysts appeared to resolve spontaneously within 3-12 weeks [9]. The situation has not changed even with the advent of ultrasonography since, for the most part, there has not been precise definition of the pseudocyst in the reports and it seems, from earlier studies, that any fluid present in the lesser sac was regarded as a pseudocyst. Also, the possibility that the results of the resolution of acute fluid collections and the resolution of acute pseudocysts were presented together should be considered.
Moreover, when alcohol is the major cause of pancreatic pseudocysts, only ERCP and MRCP can reliably differentiate between acute and acute-on-chronic pancreatitis. The greater the number of patients having acuteon- chronic pancreatitis the lower the spontaneous resolution rate is thought to be. Warshaw and Rattner [10] performed ERCP for patients with pancreatic pseudocysts. According to their findings, pancreatitis can be divided into acute, chronic and acute-onchronic. A 21% pseudocyst resolution rate was observed in the acute pancreatitis group, while no pseudocysts resolved in the other two groups.
When alcohol is the major cause of a pancreatic pseudocyst, a 20-29% spontaneous resolution rate has been reported by other pancreatologists. Bourliere and Sarles [11] noted a similar 20% spontaneous resolution rate in pseudocysts with biliary pancreatitis as the major cause. Alcohol-related pancreatitis was present only in 4% of cases in their series. However, a recent prospective cohort study of a non-alcoholic population with acute pancreatitis revealed that 65% of acute pancreatic pseudocysts resolved spontaneously within one year [12]. This study used the Atlanta criteria for a reliable diagnosis of acute pancreatic pseudocysts.
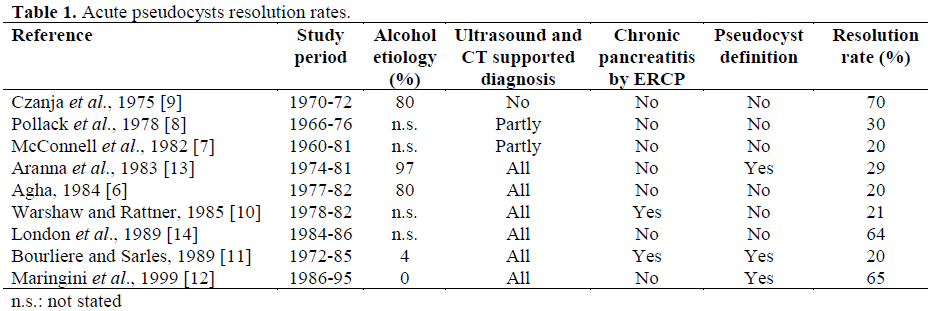
A collection of reports on the incidence of spontaneous resolutions show very variable results (Table 1).
There is also a report of a spontaneously vanishing pseudocyst in the remnant pancreas after a pylorus-preserving pancreatoduodenectomy. A cystic lesion appeared in the remnant pancreas 6 months after the operation and disappeared 3 months later [15].
Which Pseudocysts Are more Likely to Resolve?
From a clinical point of view, it is, of course, of interest to note that the pseudocyst may resolve spontaneously with time. However, it is even more interesting if there are prognostic factors that can give at least a hint as to which type of pseudocysts are likely to regress – and which will not resolve.
Duration of the Pseudocyst versus Size
Warshaw and Rattner [10] reported that no cyst presenting more than 6 weeks following an attack of acute pancreatitis resolved. On the other hand, the authors noted that the size of the cyst did not seem to affect the chance of resolution. Similarly, Bradley et al. [16] followed the natural history of pseudocysts in 93 patients, 31 who had acute pancreatitis and 62 who had chronic disease. Spontaneous resolution occurred in 10 (42%) of 24 patients in whom a pseudocyst was present for less than 6 weeks. By contrast, of the 13 pseudocysts which had been present for 7-12 weeks, only one (8%) resolved spontaneously. Spontaneous resolution did not occur in any of the remaining 12 patients followed for up to 18 weeks. The clear implication is that pseudocysts still presenting at 6 weeks are unlikely to resolve spontaneously [16].
This conclusion was challenged by the results of more recent studies. In the series of Vitas and Sarr [17], of 68 patients treated with the expectant approach overall resolution of the pseudocyst occurred in 57% of the 24 patients with satisfactory radiographic follow-up, and 38% resolved more than 6 months after diagnosis. O’Malley et al. [18] noted that pseudocysts of more than 4 cm resolved spontaneously at a mean of 3 months after diagnosis although, in one case, resolution did not occur until 28 months. Maringhini et al. [12] found that within one year after diagnosis 65% of acute pseudocysts resolved. Pseudocysts of less than 5 cm in size were more likely to resolve than larger ones. Gouyon et al. [19] observed a pseudocyst resolution rate of 26% in patients with chronic alcoholic pancreatitis. The median time to regression was 29 weeks (range 2-143) and the independent predictive factor of pseudocyst resolution or asymptomatic course was a size of less than 4 cm.
Size was a major factor predicting pseudocyst resolution in the Aranha et al. [13] series. The mean diameter of cystic lesions which resolved was 4±1 cm as compared to a diameter of 9±1 cm in those cysts that did not resolve, which was a significant difference. Only four of 26 pseudocysts greater than 6 cm in diameter at initial examination resolved. Several more studies also confirmed that cysts less than 4 cm in diameter could resolve spontaneously [20, 21, 22, 23].
Chronic Pseudocysts
Aranha et al. [13] noted that patients with pancreatic calcifications and evidence of chronic pancreatitis had no resolution of their pancreatic pseudocysts. Warshaw and Rattner [10], from their series of 42 patients with pancreatic pseudocysts, also concluded that evidence of chronic pancreatitis and pancreatic duct abnormality other than communication with the pseudocyst were criteria suggesting that a pseudocyst will not resolve spontaneously.
McConnell et al. [7] reported a resolution rate in only 3% of cases with chronic pancreatic pseudocysts. Bourliere and Sarles [11] reviewed 77 consecutive patients with pseudocysts of the pancreas associated with chronic pancreatitis. Ultrasonography and/or CT scans showed that 9% of them resolved spontaneously. The main diameter of chronic pancreatic pseudocysts which resolved was 3 cm [11]. Gouyon et al. [19] retrospectively studied the factors predicting the outcome of pseudocysts complicating alcoholic chronic pancreatitis. The patients were included if the presence of at least one of the following criteria was documented: calcifications, pancreatic duct anomalies which were at least moderate according to the international Cambridge classification and/or histological diagnosis of chronic pancreatitis. The pseudocyst resolution rate was 26% in their group of 90 cases [19].
Other Factors Associated with Pseudocyst Resolution
Other factors found to reduce the likelihood of the spontaneous resolution of cystic lesions are multiple cysts [13], pseudocyst location in the tail of the pancreas [12], thicker pseudocyst wall [10, 24], a lack of communication with the pancreatic duct, an associated proximal stricture of the pancreatic duct [24], increase in size on follow-up examination [13], biliary or postoperative etiology of pancreatitis [25] and extrapancreatic development in chronic alcoholic pancreatitis [19].
The severity of acute pancreatitis as well as the extent of the pancreatic necrosis was found to influence the spontaneous resolution rate. In the Neoptolemos et al. [26] study, all pseudocysts resolved spontaneously if they were the result of mild acute pancreatitis or severe pancreatitis with less than 25% of pancreatic necrosis.
Risk for Complications in Untreated Pancreatic Pseudocysts
It is difficult to interpret the current literature because patients whose pseudocysts follow acute or chronic pancreatitis are grouped together. Furthermore, papers on the natural history of pancreatic pseudocysts, due to their retrospective approach, may have some methodological bias, such as selection bias [16, 17], an elevated number of dropouts [16], or no regular imaging and clinical follow-up [16, 17, 27].
In the series of Bradley et al., the incidence of complications correlated directly with the length of time the pseudocyst was present: 20% of patients with an early pseudocyst (less than 6 weeks) had a complication, as opposed to 46% with cysts that were 7-12 weeks old and 75% of those with chronic cysts (beyond 13 weeks). Of particular interest is the observation that each of the seven deaths (12 %) occurred as a direct result of the pseudocyst and that their complications developed an average of thirteen and a half weeks after the presumed initial development of the pseudocyst [16].
More recently, Yeo et al. [27] in Baltimore, used serial CT to observe the natural history of pancreatic pseudocysts in 75 patients; their findings challenge the conclusion of Bradley et al. that delay is at best fruitless and at worst hazardous [27]. Thirty-six patients who were asymptomatic were managed without surgery and were observed for a mean of 1 year. Of these, 60% had complete resolution of the pseudocyst and 40% had pseudocysts which remained stable or reduced in size. Only one patient of the 36 treated expectantly, i.e. without surgery, developed a complication from the pseudocyst in the form of a transient intracystic haemorrhage.
Vitas and Sarr reported on 68 patients initially treated selectively with a nonoperative, expectant approach. Severe, life-threatening complications in this group which was followed up for a mean of 46 months occurred in only 6 patients (9%) including intracystic haemorrhage in 3, perforation in 2, and cyst infection in 1. Nineteen (28%) patients eventually underwent elective surgery directed at either the pseudocyst or other complications related to pancreatitis [17].
Maringhini et al. [12] analysed the natural history of 83 non-alcoholic patients with fluid collections and/or pseudocysts in which chronic pancreatitis was accurately excluded. In the first six weeks of follow-up, spontaneous disappearance was observed in 12 (14%) and complications in 19 (23%) of the 83 patients. The complications observed were pain in 12 patients, infection in 4, fistula in 2, and rupture in one patient. Only two patients died. After the first six weeks of follow up, the pseudocyst spontaneously disappeared in 31 and complications occurred in 14 of 48 patients. Eleven of the patients with complications had pain, while three presented fistulas.
There is a case presented in which a pancreatic pseudocyst masquerading as a pericardial effusion dissected into the mediastinum, eroding into the pericardial sac and causing a life-threatening pericardial tamponade [28].
Alcoholics versus Non-Alcoholics
In the Maringhini et al. [12] series, the incidence of complications and spontaneous disappearance did not differ from two of the three retrospective studies on natural history in a mainly alcoholic population [17, 27]. Yet another study [16] showed quite different results; a very low incidence of spontaneous disappearance and a high incidence of complications after the first six weeks of follow-up. This study was based on an indigent alcoholic population in whom compliance with medical therapy is notoriously poor and continued alcohol abuse is common. Extrapolation of these data to other patient populations who have pancreatic pseudocysts related to causes other than alcohol abuse may be inappropriate. Moreover, 39% of this population was lost to follow-up. Consequently, the incidence of late resolution of pseudocysts may be underestimated and the incidence of serious complications may be overestimated [12].
Asymptomatic versus Symptomatic Pseudocysts
9% [17] in patients managed without surgery and observed for a mean of 1 and 3.5 years, respectively. These results may represent different study populations and selection biases. Bradley et al. [16], in their prospective study, aimed at exploring the natural history of the pseudocysts. They excluded from the study 11 patients with acute pancreatitis who had undergone urgent exploration and drainage because of a suspected intraabdominal catastrophe or the appearance of superimposed sepsis. The patients with chronic symptoms and pseudocyst were excluded only in the case in which they underwent elective drainage primarily due to a prestudian bias on the part of the surgical investigator. Thus, their population presents a mixed series of symptomatic and asymptomatic pseudocysts. By contrast, in the studies with a low complication rate, non-operative management was reserved only for those patients who had asymptomatic pseudocysts and were able to tolerate oral intake. Moreover, they continued with a non-operative approach only if the patient had no enlargement or complications of the pseudocyst. These studies represent more the success of patient selection for a non-operative approach than the real natural course of pancreatic pseudocysts.
Concluding Remarks
Obviously, it is possible to conclude that there are spontaneous resolutions of pancreatic pseudocysts, especially pseudocysts in postacute pancreatitis. The resolution rate and complication rate of untreated pseudocysts is not known, but, in most series, it is less than one in ten. However, as in all results concerning pseudocysts, the rate strongly depends on the selection criteria of the population studied. Overall, the incidence of late resolution of pseudocysts may be underestimated and the incidence of serious complications may be overestimated.
Patients with a lesser likelihood of spontaneous resolution of pseudocystic lesions are those found after acute pancreatitis, multiple cysts, pseudocyst location in the tail of the pancreas, thicker pseudocyst wall, a lack of communication with the pancreatic duct, an associated proximal stricture of the pancreatic duct, increase in size on follow-up examination, biliary or postoperative etiology of pancreatitis, short time of symptoms of the pseudocyst and extrapancreatic development in patients with chronic alcoholic pancreatitis.
References
- Andrén-Sandberg Å, Dervenis C. Pancreatic Pseudocysts in the 21st Century. Part I: Classification, Pathophysiology, Anatomic Considerations and Treatment. JOP. J Pancreas (Online) 2004; 5:8-24. [PMID 14730118]
- Sankaran S, Walt AJ. The natural and unnatural history of pancreatic pseudocysts. Br J Surg 1975; 62:37-44. [PMID 1111673]
- Hanna WA. Rupture of pancreatic cysts. Report of a case and review of the literature. Br J Surg 1960; 47:495-8. [PMID 14399534]
- Bradley EL 3rd, Clements LJ. Spontaneous resolution of pancreatic pseudocysts: implications for timing of operative intervention. Am J Surg 1975; 129:23-8. [PMID 1211527]
- Nakamura K, Sarles H, Payan H. Three dimensional reconstruction of the pancreatic ducts in chronic pancreatitis. Gastroenterology 1972; 62:942-9. [PMID 5029079]
- Agha FP. Spontaneous resolution of acute pancreatic pseudocysts. Surg Gynecol Obstet 1984; 158:22-6. [PMID 6691163]
- McConnell DB, Gregory JR, Sasaki TM, Vetto RM. Pancreatic pseudocyst. Am J Surg 1982; 143:599- 601. [PMID 7081569]
- Pollak EW, Michas CA, Wolfman EF Jr. Pancreatic pseudocyst: management in fifty-four patients. Am J Surg 1978; 135:199-201. [PMID 626292]
- Czaja AJ, Fisher M, Marin GA. Spontaneous resolution of pancreatic masses (pseudocysts?) – development and disappearance after acute alcoholic pancreatitis. Arch Intern Med 1975; 135:558-62. [PMID 1138670]
- Warshaw AL, Rattner DW. Timing of surgical drainage for pancreatic pseudocyst. Clinical and chemical criteria. Ann Surg 1985; 202:720-4. [PMID 4073984]
- Bourliere M, Sarles H. Pancreatic cysts and pseudocysts associated with acute and chronic pancreatitis. Dig Dis Sci 1989; 34:343-8. [PMID 2646086]
- Maringhini A, Uomo G, Patti R, Rabitti P, Termini A, Cavallera A, et al. Pseudocysts in acute nonalcoholic pancreatitis: incidence and natural history. Dig Dis Sci 1999; 44:1669-73. [PMID 10492151]
- Aranha GV, Prinz RA, Esguerra AC, Greenlee HB. The nature and course of cystic pancreatic lesions diagnosed by ultrasound. Arch Surg 1983; 118:486-8. [PMID 6830440]
- London NJ, Neoptolemos JP, Lavelle J, Bailey I, James D. Serial computed tomography scanning in acute pancreatitis: a prospective study. Gut 1989; 30:397-403. [PMID 2651228]
- Kojima M, Yamaguchi K, Chijiiwa K, Tanaka M. A vanishing pseudocyst in the remnant pancreas after pylorus-preserving pancreatoduodenectomy. J Gastroenterol 2002; 37:479-82. [PMID 12108685]
- Bradley EL, Clements JL Jr, Gonzalez AC. The natural history of pancreatic pseudocysts: a unified concept of management. Am J Surg 1979; 137:135-41. [PMID 758840]
- Vitas GJ, Sarr MG. Selected management of pancreatic pseudocysts: operative versus expectant management. Surgery 1992; 111:123-30. [PMID 1736380]
- O'Malley VP, Cannon JP, Postier RG. Pancreatic pseudocysts: cause, therapy, and results. Am J Surg 1985; 150:680-2. [PMID 3907380]
- Gouyon B, Levy P, Ruszniewski P, Zins M, Hammel P, Vilgrain V, et al. Predictive factors in the outcome of pseudocysts complicating alcoholic chronic pancreatitis. Gut 1997; 41:821-5. [PMID 9462217]
- D?Egidio A, Schein M. Pancreatic pseudocysts: a proposed classification and its management implications. Br J Surg 1991; 78:981-4. [PMID 1913122]
- Andersson R, Janzon M, Sundberg I, Bengmark S. Management of pancreatic pseudocysts. Br J Surg 1989; 76:550-2. [PMID 2667688]
- Ravelo HR, Aldrete JS. Analysis of forty-five patients with pseudocysts of the pancreas treated surgically. Surg Gyn Obstet 1979; 148:735-8. [PMID 432787]
- Beebe DS, Bubrick MP, Onstad GR, Hitchcock CR. Management of pancreatic pseudocysts. Surg Gynecol Obstet 1984; 159:562-4. [PMID 6390759]
- Forsmark CE, Grendell J. Complications of pancreatitis. Semin Gastrointest Dis 1991; 2:165-76.
- Nguyen BL, Thompson JS, Edney JA, Bragg LE, Rikkers LF. Influence of the etiology of pancreatitis on the natural history of pancreatic pseudocysts. Am J Surg 1991; 162:527-31. [PMID 1670219]
- Neoptolemos JP, London NJ, Carr-Locke DL. Assessment of main pancreatic duct integrity by endoscopic retrograde pancreatography in patients with acute pancreatitis. Br J Surg 1993; 80:94-9. [PMID 8428306]
- Yeo CJ, Bastidas JA, Lynch-Nyhan A, Fishman EK, Zinner MJ, Cameron JL. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990; 170:411-7. [PMID 2326721]
- Tan MH, Kirk G, Archibold P, Kennedy P, Regan MC. Cardiac compromise due to a pancreatic mediastinal pseudocyst. Eur J Gastroenterol Hepatol 2002; 14:1279-82. [PMID 12439127]

