Keywords
Everolimus; lanreotide; Octreotide; Streptozocin; sunitinib;
temozolomide
Abbreviation
PNETs pancreatic neuroendocrine tumors
INTRODUCTION
Somatostatin Analogues
Somatostatin is a peptide hormone that regulates the
endocrine system, affects cell proliferation, and inhibits
the secretion of hormones in vivo. Somatostatin and its
analogs will act by binding to somatostatin receptors,
and inhibiting the secretion of peptides from NET cells
through somatostatin receptor SSTR-2 and SSTR-5.
The presence of these receptors is determined through
diagnostic imaging with either an Octreoscan or Gallium-
Ga DOTATATE. For those with positive imaging, symptoms
can be well controlled with somatostatin analogs. They
are highly effective in controlling symptoms in functional
PNETs including VIPomas, glucagonomas, as well as
somatostatinomas [1, 2, 3].
Current available Somatostatin analogues include
Octreotide and Lanreotide. These analogues can mimic
the physiological activities of somatostatin and can
therefore inhibit secretion of hormones including gastrin,
glucagon, insulin, TSH, VIP, thereby working to reduce
secretion of fluids by the intestine and pancreas, reduce
gastrointestinal motility, inhibit hormone action from the
anterior pituitary and reduce portal pressure in bleeding
varices [1, 2, 3]. A depot preparation known as Sandostatin
LAR is considered the standard approach for symptomatic
treatment. It is typically initiated a dose of 20 mg IM with
dose-escalation. Patients may sometimes use short-acting octreotide for symptoms while doses are being titrated.
Lanreotide is another synthetic analogue of somatostatin,
binding to the same receptors as somatostatin, with a
longer half-life and prolonged effects [3, 4, 5, 6, 7].
While Somatostatin analogs have a favorable safety
profile, and are able to treat symptoms associated with
hormone hypersecretion, the anti-proliferative effects
to control tumor growth have continued to be examined.
They are recommended in patients with unresectable,
somatostatin receptor positive, well differentiated PNETs,
with a high tumor burden [4, 5, 6, 7]. In the Controlled
Study of Lanreotide Anti-proliferative Response
in Neuroendocrine Tumors (CLARINET), the antiproliferative
effects of Lanreotide were examined in 200
patients with nonfunctioning, somatostatin receptorpositive,
unresectable locally advanced tumor or metastatic
enteropancreatic neuroendocrine tumors, with Ki-67
values <10% [7, 8, 9, 10, 11]. In this 96-week, randomized,
double-blind, placebo-controlled, multicenter, phase 3
study, an extended-release aqueous-gel formulation of
Lanreotide at a dose of 120 mg, was compared with placebo
through means of deep subcutaneous injection every 28
days. At 24 months, there was a significantly increased
progression free survival (PFS) in the Lanreotide group at
65% (95% CI, 54.0 to 74.1) vs. 33% (95% CI, 23.0 to 43.3)
in the placebo group. There were no significant differences
in quality of life or overall survival [7, 8, 9, 10, 11].
In a separate trial from the PROMID Study Group,
Octreotide LAR 30 mg intramuscularly was evaluated for
tumor progression and survival in a placebo controlled,
double blind, phase IIIB study performed in patients
with well-differentiated metastatic midgut NETs. Results
indicated that the median time to tumor progression,
which was the primary efficacy end point in the octreotide
LAR and placebo groups, was 14.3 and 6 months,
respectively (hazard ratio [HR]=0.34; 95% CI, 0.20 to 0.59;
P=0.000072). After 6 months of treatment, stable disease
was observed in approximately 66% of patient in the octreotide group vs. 37% of patients in the placebo group.
The HR for overall survival was 0.81 (95% CI, 0.30 to 2.18)
[9, 10, 11, 12]. In order to then investigate whether this
beneficial effect also affected overall survival patients
in the PROMID trial, patients were then followed until
January 2013 at least once a year. Between July 2001 and
January 2008, 42 and 43 patients were randomly assigned
to receive Octreotide or Placebo groups. Median OS for all
85 patients was 85 months, “not reached” in the Octreotide
arm and 84 months in the Placebo arm (p=0.59, HR=0.85
[CI 0.46; 1.56. Median OS in the HL (hepatic tumor load)
≤ 10% subgroup was “not reached” (Octreotide) vs. 80.5
months (placebo) (p=0.14, HR=0.56 [CI 0.25; 1.23]). In the
HL>10% subgroup the respective numbers were 35 vs. 84
months (p=0.14, HR=2.18 [CI 0.75; 6.33]). Conclusions from
this follow up study indicated that Octreotide LAR not only
prolonged Time to Progression, but also extended Overall
Survival in the subgroup of patients with metastatic midgut
and a low Hepatic Tumor Load (≤ 10% at study entry) but
not in the high Hepatic Tumor Load (HL>10%) subgroup.
Patients who had been randomized at study entry in the
placebo group then received octreotide LAR after disease
progression, but these experienced a less favorable OS in
the low HL subgroup [10, 11, 12, 13, 14, 15].
Overall, somatostatin analogs have been effective
in controlling symptoms associated with hormone
hypersecretion in functional neuroendocrine tumors.
In addition, they have also been shown to control tumor
growth. Guidelines from the European Neuroendocrine
Tumor Society and the North American Neuroendocrine
Society suggest that in the asymptomatic setting these
medications should be initiated for unresectable,
somatostatin receptor positive, well differentiated
PNETs with high tumor burden. Although progression
free survival has been correlated with treatment, overall
survival with somatostatin analogs continues to be under
clinical investigation [12, 13, 14, 15, 16, 17, 18].
Small Molecule Tyrosine Kinase Inhibitors (TKI)
Sunitinib: Vascular endothelial growth factor (VEGF)
is a crucial driver of angiogenesis in PNETs [19, 20]. Tissue
from malignant PNETs has widespread expression of
platelet-derived growth factor receptors (PDGFRs) α and
β, stem-cell factor receptor (c-kit), and vascular endothelial
growth factor (VEGF) receptors VEGFR-2 and VEGFR-3
[21, 22, 23]. Preclinical studies have shown that Sunitinib
malate (Sutent, Pfizer) inhibits the aforementioned
kinases [24, 25], and delays tumor growth of pancreatic
islet-cell tumors in transgenic mouse models [26, 27]. In
phase 1 and 2 trials, Sunitinib showed antitumor activity in
patients with PNETs [26, 27]. In a phase III trial in patients
with advanced, well-differentiated, progressive PNETs,
a total of 171 patients were randomly assigned (in a 1:1
ratio) to receive best supportive care (BSC) with either
Sunitinib at a dose of 37.5 mg per day or placebo [28]. The
study was discontinued early because the independent
data and safety monitoring committee observed more
serious adverse events and deaths in the placebo group as well as a difference in progression-free survival (PFS)
favoring Sunitinib. Sunitinib improved investigatorassessed
PFS versus placebo (11.4 vs. 5.5 months; HR, 0.42;
P<0.001). Median OS was not reached, however the HR for
death was 0.41 (95% CI, 0.19 to 0.89; P=0.02) in favor of
Sunitinib. Hand-foot skin reaction and hypertension of
any grade occurred in 23 and 26% of patients receiving
Sunitinib, respectively, and the most common grade 3 or 4
adverse events in this group were neutropenia (12%) and
hypertension (10%). Despite these side effects, there were
no differences in the quality-of-life index with Sunitinib.
Based upon these data, Sunitinib was approved by the U.S.
Food and Drug Administration (FDA) in May 2011 for the
treatment of progressive, well-differentiated pancreatic
neuroendocrine tumors in patients with unresectable,
locally advanced, or metastatic disease. In a later report,
5 years after study closure median OS was 38.6 months in
the Sunitinib group versus 29.1 months for placebo (HR,
0.73; 95% CI 0.50-1.06; P=0.094). Although the observed
median OS improved by nearly 10 months, it did not reach
statistical significance, potentially due to crossover from
placebo to Sunitinib in 69% of the patients in the control
group [29].
Mammalian Target of Rapamycin (mTOR)
Inhibitors
Everolimus: Everolimus (Afinitor, Novartis
Pharmaceuticals) inhibits mammalian target of rapamycin
(mTOR), a serine–threonine kinase which stimulates
cell growth, proliferation, and angiogenesis [30, 31, 32].
Autocrine activation of the mTOR signaling pathway,
mediated through insulin-like growth factor 1, has been
implicated in the proliferation of PNETs [33]. Inhibition of
mTOR has anti-proliferative effect on PNET cell lines [34, 35]. Everolimus has demonstrated promising antitumor
activity in phase 2 studies involving patients with PNETs
[30, 31].
The RAD001 in Advanced Neuroendocrine Tumors,
third trial (RADIANT-3) study was an international,
multicenter, double-blind, phase 3 study that compared
Everolimus monotherapy (10 mg daily) to placebo both
in conjunction with BSC in 410 patients with advanced
PNETs [36]. The median PFS was 11.0 months with
Everolimus as compared with 4.6 months with placebo
(HR for disease progression or death from any cause
with Everolimus, 0.35; 95% confidence interval [CI], 0.27
to 0.45; P<0.001), representing a 65% reduction in the
estimated risk of progression or death. Median OS was not
reached at the time of study reporting, and no significant
difference between the groups was observed (HR for death
with Everolimus, 1.05; 95% CI, 0.71 to 1.55; P=0.59). The
most common grade 3 or 4 drug-related adverse events
were stomatitis (7%), anemia (6%), and hyperglycemia
(5%). Based upon these data Everolimus was approved
in the United States for the treatment of progressive NETs
of pancreatic origin in patients with unresectable, locally
advanced, or metastatic disease in May 2011. In a later
analysis, median OS favored Everolimus (44 versus 37.7 months), but the difference was not statistically significant
(hazard ratio, 0.94; 95% CI, 0.73 to 1.20; P=0.30), likely
secondary to the high rate of crossover of patients from
placebo to Everolimus (85 percent) which may have
confounded the ability to detect a difference in OS [37].
Somatostatin analogs, Everolimus, and Sunitinib all
extend PFS compared with BSC alone, although none of
these agents have been compared directly with each other.
In the absence of comparative trials, the choice of initial
agent is influenced by the adverse effect profile. Due to a
favorable toxicity profile; somatostatin analogue may be
an appropriate first choice for many patients with use
of targeted agents such as Sunitinib or Everolimus upon
disease progression [38, 39]. Since Everolimus causes
hyperglycemia, it has an additional therapeutic benefit
in patients with functioning insulinomas and refractory
hypoglycemia [40, 41].
CYTOTOXIC CHEMOTHERAPY
Streptozocin (STZ)
Although the results of chemotherapy in extrapancreatic
NETs are often disappointing resulting in
objective response rates (ORR) of less than 20% in most
trials, PNETs are known to be chemosensitive [39, 42].
Streptozocin (STZ) based combination therapy has
been a historical treatment standard for patients with
advanced PNETs [42]. In retrospective studies, STZ-based
chemotherapy regimens, in which STZ is combined with
doxorubicin, fluorouracil, or both, have been associated
with ORR of 30% to 40% [43, 44]. However, widespread
use of STZ which is an alkylating agent has been limited by
the cumbersome administration schedule and by concerns
about toxicity [42]. In addition, with the availability
of targeted agents, the role of systemic chemotherapy
for PNETs remains controversial and the sequence of
treatment remains unclear [44].
Temozolomide
Recently, several retrospective series and small
prospective studies have explored another alkylating
agent Temozolomide –based regimens in patients with
advanced PNETs, and demonstrated ORR to be comparable
to those observed with STZ-based therapy [39]. In a small
retrospective study of 30 patients, the combination of
Temozolomide with Capecitabine (CAPTEM) showed an
impressive ORR of 70% [45]. More recently several small
retrospective studies with CAPTEM demonstrate an ORR
of 43%–70%, corresponding to a clinical benefit of 12–18
months in terms of PFS and a very impressive disease
control rate (DCR) of 70%–97% [46, 47, 48, 49, 50, 51, 52].
A preliminary report of a prospective phase II trial reported
at the 2014 American Society of Clinical Oncology (ASCO)
Gastrointestinal Cancers Symposium noted an objective
partial response in 4 of 11 patients with advanced PNETs
(36%) and an ongoing PFS in PNETs of >18.2 months which
is 150% greater than reported with Everolimus and Sutent
[48]. A trial conducted by Eastern Oncology Cooperative
Group (ECOG) which has completed enrollment, is evaluating the relative efficacy of the Temozolomide plus
Capecitabine versus Temozolomide alone (ClinicalTrials.
gov Identifier: NCT01824875). Why some PNETs and not
others are susceptible to treatment with alkylating agents
remains uncertain. Several small retrospective series have
suggested that O6-methylguanine DNA methyltransferase
(MGMT) deficiency may predict response to Temozolomide
in PNETs as well; however expression of MGMT has not
been validated as a predictive biomarker [39, 53]. The
question whether MGMT status could be a response
predictor to CAPTEM therapy was updated at the ASCO
meeting in 2015. In a trial with 144 PNETs, MGMT status
was not predictive of response (P=0.358) [54]. Conversely,
MGMT methylation was correlated with PFS prolongation
(16.3 vs. 5.4 months) in PNET patients in another study
presented at the same meeting [53]. Due to lack of
prospective validation as a predictor of response in NETs,
and variability in the techniques used to assess MGMT
status, it cannot be put to routine clinical use to select
patients for Temozolomide therapy.
Dacarbazine
Dacarbazine, an alkylating agent, has also been used to
treat PNETs. It has been assessed alone and in combination
with 5-FU, epirubicin, leucovorin, and other agents. A
phase II study of Dacarbazine alone was conducted in 50
PNET patients with a response rate of 34% and a survival
time of 19.3 months. However, not unlike STZ, the toxicity
of Dacarbazine has limited its widespread use [55, 56].
Other Drugs
In addition to the alkylating agents described above,
other antineoplastic drugs, including 5-FU, paclitaxel,
gemcitabine, and oxaliplatin, have been used in clinical
studies to treat PNETs. However these studies were not
randomized and were conducted using small numbers of
patients. Some studies have described the use of oxaliplatin
in combination with capecitabine in PNETs, with response
rates of about 30%, a median PFS of 9.8 months, and a
median survival time of more than 24 months [56].
Sequence of Therapies and Future Direction
As discussed in other sections of this review, for
patients with potentially resectable metastatic disease,
resection may provide control of symptoms and prolong
survival. For patients with unresectable disease, options
to control tumor growth and symptoms related to
hormonal hypersecretion include somatostatin analogues,
nonsurgical liver-directed therapy, and systemic antitumor
therapy [38]. Some patients with PNETs may feel
relatively well despite the presence of metastatic disease.
Such patients with asymptomatic advanced pancreatic
NETs, who otherwise have low-grade tumor histology
and a minimal volume of metastatic disease, can likely
be managed by diligent observation alone rather than
committing them to a lifetime of antineoplastic therapy.
Patients with symptoms of hormone hypersecretion
should be managed with somatostatin analogs and
other agents, as appropriate to the specific syndrome as detailed in other sections of this review [38, 39]. Moreover,
somatostatin analogs also have an anti-proliferative tumor
effect in functional and non-functional PNETs [8].
For patients with a larger disease volume or evidence
of tumor progression, treatment should be initiated even
if the patient is asymptomatic. Somatostatin analogs,
Everolimus, and Sunitinib all extend PFS compared with
BSC alone, although none of these agents have been
compared directly with each other. In the absence of
comparative trials, the choice of initial agent is influenced
by the adverse effect profile. Due to a favorable toxicity
profile; somatostatin analog may be an appropriate first
choice for many patients with use of targeted agents such
as Sunitinib or Everolimus upon disease progression [38, 39].
With the proven benefit of molecularly targeted
drugs, including Everolimus and Sunitinib in large-scale
randomized controlled studies, these agents have been
accepted as a standard therapy, and the place of cytotoxic
chemotherapy in the treatment of PNETs has become even
more uncertain. As such cytotoxic chemotherapy should
be used for patients who cannot tolerate Everolimus or
Sunitinib or have failed to respond to these drugs. Due to
lack of data from large prospective randomized trials, no
cytotoxic chemotherapy regimen has been established as
a global standard [38, 39, 56]. Most frequently employed
regimens include alkylating agents, such as Streptozocin
and Temozolomide, of which Temozolomide based
regimens (for example CAPTEM) appear to have a better
side effect profile [53].
The response rates to molecularly targeted drugs are
relatively low (Sunitinib, 9.3%; Everolimus, 5%), and
a cytoreductive effect cannot be expected. Conversely,
cytotoxic chemotherapy is associated with higher tumor
response rates than either somatostatin analogues or
the targeted therapies. As a result, for patients who are
highly symptomatic from tumor bulk or who have rapidly
enlarging metastases, and for whom tumor shrinkage
rather than tumor stabilization is the primary objective,
front line cytotoxic chemotherapy is the preferred option
rather than molecularly targeted therapy or a somatostatin
analog [38, 39, 56, 57].
Several critical questions remain unanswered
and need to be elucidated via large scale multi center
randomized studies given the rarity of this disease.
Sunitinib, Everolimus and somatostatin analogues should
be compared directly to each other in a prospective
trial. At the present time, the evidence for cytotoxic
chemotherapy as a standard therapy is inadequate, but
there is a strong possibility that its usefulness will be
demonstrated, and diligent evaluation using high-quality
clinical trials is needed. Although there is no head-to-head
comparison between CAPTEM and molecularly targeted
drugs in PNETs, and cross trial comparison is not prudent,
the median PFS and ORR achieved by CAPTEM (12–18
months, 43-70%) is superior to that produced by targeted
drugs (11 months, <10%). Therefore CAPTEM should be tested against Sunitinib and Everolimus in the first-line
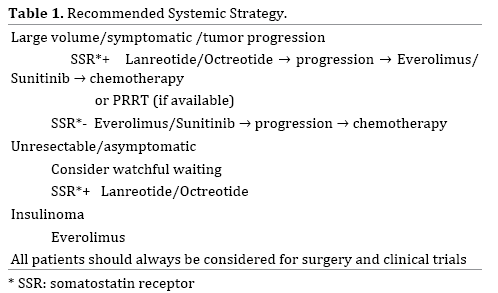
setting [53]. Trials on the best sequence of treatments, e.g.
the SEQTOR trial, a European randomized phase III study
investigating STZ+5-FU followed by Everolimus versus
the reverse sequence, are ongoing (ClinicalTrials.gov
Identifier: NCT02246127) (Table 1).
Therapeutic resistance involving a multitude of
mechanisms is often encountered with targeted agents.
Concurrent inhibition of VEGF and the mTOR pathway
may be an effective strategy to overcome resistance [38].
In a Phase II study, combination therapy with mTOR
inhibitor temsirolimus and VEGF-A antibody bevacizumab
showed an RR of 41% [58]. Another phase II study that
randomized patients with metastatic PNETs to receive
everolimus with or without bevacizumab showed a higher
RR in the combination group (31% vs. 12%, P=0.005) [58].
However, severe adverse events were more frequent in
the combination group, highlighting the need for less toxic
regimens. The antiangiogenic TKI pazopanib demonstrated
promising results in a phase II trial where PNET patients
who received pazopanib combined with depot octreotide
had a median PFS of 14.4 months [59].
Although these new agents give patients multiple
therapeutic options, treatment stratification becomes
critical. To date, no established predictive markers are
available to facilitate treatment decisions and to identify
the optimum agent for each patient. Clarifying which
patients should be treated and the optimal timing of the
treatment should also be addressed in the future trials. The
proliferation marker Ki-67 is well known as a prognostic
marker; however its role as a predictor of response to
treatment is less well defined [42]. In a study by Turner et
al. both the mitotic index and Ki67 were associated with
a response to chemotherapy consisting of 5-fluorouracil,
cisplatin, and streptozocin [60]. In another study of PNET
patients, 28 tumor with ki67>5% showed an ORR of 64%
versus 29% for the 31 PNETs with ki67<5%, P=0.006
[53,54]. Similarly, another trial of NETs described an ORR
of 29% in tumors with ki-67<2% and 39% in NETs with ki-
67>2% to 20% [52]. However definite conclusions cannot
be made from these small retrospective studies.
Peptide Receptor Radionuclide Therapy (PRRT)
PRRT is a form of systemic radiotherapy that allows
targeted delivery of radionuclides to tumor cells expressing high levels of somatostatin receptors. Historically, the first
therapeutic experiences in NET were performed using
111ln-pentetreotide and produced a clinical benefit but
rarely a radiological response [61]. The two radiopeptides
most commonly used for PRRT, 90Y-DOTA0-Tyr3-octreotide
(90Y-DOTATOC) and 177Lu-DOTA0-Tyr3-octreotide (177Lu-
DOTATATE), have been successfully employed for more
than a decade for the treatment of advanced NET. They
differ from one another in terms of emitted particles,
particle energy, and tissue penetration [62, 63, 64].
90Y is a high-energy β-particle emitter. The most
extensive experience with 90Y-DOTATOC comes from a large
single institution series of 1109 patients with metastatic
gastroenteropancreatic NET and disease progression
within 12 months of study entry, with visible tumor uptake
on pretreatment somatostatin receptor scintigraphy
[65]. The median number of courses administered was
two, range 1 to 10. Overall, 378 patients (34%) had a
"morphologic" response, 172 (15%) had a biochemical
response, and 329 (29.7%) improved symptomatically.
The median survival from diagnosis was 94.6 months.
Longer survival correlated with responses by any of the
above criteria. Transient grade 3 or 4 hematologic toxicities
developed in 142 (12%), and loss of renal function was
the main dose limiting toxicity. In all, 103 patients (9%)
had permanent grade 4 or 5 (fatal, n=35) renal toxicity. 177-Lu emits both β and γ rays. Data from non-randomized
trials of 177-Lu-Dotatate have consistently shown high
response rates and long durations of median progressionfree
survival in heterogeneous patient populations with
gastroenteropancreatic neuroendocrine tumors [66, 67, 68, 69]. Response rates were particularly high in
PNETs, ranging from 36% for nonfunctioning tumors, to
approximately 40 to 60% for functioning gastrinomas,
insulinomas, and VIPomas.
A high prevalence of somatostatin receptor expression
in NETs provides the rationale for PRRT. The role of PRRT
in patients with progressive advanced PNETs is unclear. In
the United States, radiolabeled somatostatin analogs are
not widely available, and this form of treatment for PNETs
remains investigational. Here are reports of several PRRT
studies in PNETs.
A prospective phase II study published in 2013
used 177Lu-octreotateina cohort (n=52) with advanced
well or moderately differentiated PNETs. Patients were
divided into two groups treated with different levels of
activity based on possible existence of risk factors for renal
toxicity, such as hypertension and diabetes. Thus, full dose
(21-28 GBq) was compared with a reduced dose (11-20
GBq) for a normal and risk subset of subjects, respectively.
Both regimens resulted in antitumor efficacy. PFS was not
reached at the time of the analysis in the cohort treated
with the full-dose regimen, whereas it was 20 months in
individuals treated with a reduced dose. This suggests
the full-dose scheme should be recommended, whenever
possible [70]. After three more years follow up of the same
study, 60 consecutive patients with PNETs were enrolled.
Eligible patients were treated with two different total cumulative activities (18.5 or 27.8 GBq in 5 cycles every 6–8
weeks), according to kidney and bone marrow parameters.
28 patients received a mean full activity (FA) of 25.9 GBq
and 32 a mean reduced activity (RA) of 18.5 GBq. The DCR,
defined as the sum of CR+PR+SD was 85.7% in the FA
group and 78.1% in the RA group. Median PFS was 53.4
months in the FA group and 21.7 months in the RA group
(P=0.353). Median OS was not reached in FA patients and
was 63.8 months in the RA group (P=0.007). Furthermore,
55 patients underwent an FDG PET scan before Lu-PRRT,
32 (58%) showing an increased FDG uptake in tumor sites.
mPFS was 21.1 months in FDG PET positive patients and
68.7 months in the FDG PET-negative group (P<0.0002),
regardless of the total activity administered. Although FA
and RA are active in patients undergoing Lu-PRRT, a FA
of 27.8 GBq of Lu-PRRT prolongs PFS and OS compared
to an RA of 18.5 GBq. Also it indicated that FDG PET is an
independent prognostic factor [71].
A retrospective study evaluated a cohort with metastatic
PNETs (n=68, 52% at their first systemic treatment)
treated with 177Lu-octreotate (four intended cycles, 8 GBq
each, at 3-month intervals). Partial responses were noted
in 60%, with a median PFS of 34 months. Multivariate
analysis indicated that G1 tumors had a longer PFS [68].
Even individuals with Ki67>10% benefited from PRRT,
with a median PFS of 19 months as opposed to 26 months
for the entire cohort [72].
Another separate study by van Vliet et al. included 29
non-resectable or borderline resectable or oligometastatic
(≤3 liver metastases) nonfunctioning PNETs. This group
was treated with 177Lu-octreotate with neoadjuvant intent.
After PRRT, successful surgery could be performed in 9
patients (31%). PFS was significantly longer in operated
patients (69 vs. 49 months). A further comparison with
90 pluri-metastatic subjects treated in the same fashion
provided a PFS of 25 months [73]. This study supports the
proposal of early treatment and the possibility of down
staging tumors with PRRT.
CONCLUSION
Where available, PRRT could be considered for patients
with tumors that express somatostatin receptors and are
otherwise refractory to medical therapy. Randomized,
prospective studies to better define anti-tumor activity and
long-term toxicity of radiolabeled somatostatin analogs in
PNETs are needed.
Conflict of Interest
We declare that we have no conflict of interests.
References
- Rindi G, Arnold R, Bosman FT.Nomenclature and classification of neuroendocrine neoplasms of the digestive system. In:WHO classification of Tumours of the Digestive System, 4th ed. Bosman TF, Careneiro F, Hruban RH, Theise ND, International Agency for Research on cancer (IARC), Lyon 2010. P. 13.
- Klimstra DS, Modlin IR, Coppola D. The pathologic classification of neuroendocrine tumors:a review of nomenclature, grading, and staging systems. Pancreas 2010; 39:707. [PMID: 20664470].
- Saltz L, Trochanowski B, Buckley M.Octreotide as an antineoplastic agent in the treatment of functional and nonfunctional neuroendocrine tumors. Cancer 1993; 72:244. [PMID: 8389666].
- Eriksson B, Renstrup J, Imam H, Oberg K.High-dose treatment with Lanreotide of patients with advanced neuroendocrine gastrointestinal tumors:clinical and biological effects. Ann Oncol 1997; 8:1041. [PMID: 9402179].
- Toumpanakis C, Caplin ME.Update on the role of somatostatin analogs for the treatment of patients with gastroenteropancreatic neuroendocrine tumors. Semin Oncol 2013; 40:56. [PMID: 23391113] .
- Panzuto F, Di Fonzo M, Iannicelli E, Sciuto R, Maini CL, Capurso G, et al. Long-term clinical outcome of somatostatin analogues for treatment of progressive, metastatic, well differentiated entero-pancreatic endocrine carcinoma. Ann Oncol 2006; 17:461. [PMID: 16364959].
- Ricci S, Antonuzzo A, Galli L. Long-acting depot lanreotide in the treatment of patients with advanced neuroendocrine tumors. Am J Clin Oncol 200; 23:412. [PMID: 10955874].
- Caplin ME, Pavel M, Cwikla JB. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N Engl J Med 2014; 371:224. [PMID: 25317881].
- Rinke A, Muller HH, Schade-Brittinger C. Placebo-controlled, double-blind, prospective randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors:a report from the PROMID Study Group. J Clini Oncol 2009; 27:4656. [PMID: 19704057] .
- Rinke A, Wittenberg M, Schade-Brittinger C, Aminossadati B, Ronicke E, Gress TM, et al.Placebo-controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors (PROMID):Results of Long-Term Survival. Neuroendocrinology 2017; 104:26-32. [PMID: 26731483].
- Michael M, Garcia-Caronero R, Weber MM. The Anti-proliferative Role of Lanreotide in Controlling Growth of Neuroendocrine Tumors:A Systematic Review. Oncologist 2017; 22:272. [PMID: 28220021].
- Ducreux M, Ruszniewski P, Chayvialle JA.The anti-tumoral effect of the long-acting somatostatin analog Lanreotide in neuroendocrine tumors. Am J Gastroenterol 2000; 95:3276.[PMID: 11095353].
- Ramage JK, Ahmed A, Ardill J. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid tumours (NETs). Gut 2012; 61:6.[PMID: 22052063].
- Kunz PL, Reidy-Lagunes D. Anthony LB. Consensus guidelines for the management and treatment of neuroendocrine tumors. Pancreas 2013; 42:557. [PMID: 23591432].
- Aparicio T, Ducreuwx M, Baudin E. Antitumour activity of somatostatin analogues in progressive metastatic neuroendocrine tumours. Eur J Cancer 2001; 37:1014. [PMID: 11334727].
- Metz DC, Jensen RT. Gastrointestinal neuroendocrine tumors:pancreatic endocrine tumors. Gastroenterology 2008; 135:1469.[PMID: 18703061].
- Halfdanarson TR, Rabe KG, Rubin J. Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol 2008; 19:1727. [ PMID: 18515795].
- Strosberg J, Gardner N, Kvols L. Survival and prognostic factor analysis in patients with metastatic pancreatic endocrine carcinomas.Pancreas 2009; 38:255. [PMID: 19066493] .
- Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell 2005; 8:299-309. [PMID: 16226705].
- Inoue M, Hager JH, Ferrara N, Gerber HP, Hanahan D. VEGF-A has a critical, nonredundant role in angiogenic switching and pancreatic beta cell carcinogenesis. Cancer Cell 2002; 1:193-202. [PMID: 12086877].
- Fjallskog ML, Lejonklou MH, Oberg KE, Eriksson BK, Janson ET. Expression of molecular targets for tyrosine kinase receptor antagonists in malignant endocrine pancreatic tumors. Clin Cancer Res 2003; 9:1469-1473. [PMID: 12684421].
- Fjallskog ML, Hessman O, Eriksson B, Janson ET. Upregulated expression of PDGF receptor beta in endocrine pancreatic tumors and metastases compared to normal endocrine pancreas. Acta Oncol 2007; 46:741-746. [PMID: 17653895].
- Hansel DE, Rahman A, Hermans J. Liver metastases arising from well-differentiated pancreatic endocrine neoplasms demonstrate increased VEGF-C expression. Mod Pathol 2003; 16:652-659. [PMID: 12861060].
- Pietras K, Hanahan D. A multitargeted, metronomic, and maximum-tolerated dose “chemo-switch” regimen is antiangiogenic, producing objective responses and survival benefit in a mouse model of cancer. J Clin Oncol 2005;23:939-952. [PMID: 15557593].
- Yao VJ, Sennino B, Davis RB. Combined anti-VEGFR and anti-PDGFR actions of Sunitinib on blood vessels in preclinical tumor models. Eur J Cancer 2006; 4:27-28.
- Faivre S, Delbaldo C, Vera K. Safety, pharmacokinetic, and antitumor activity of SU11248, a novel oral multitarget tyrosine kinase inhibitor, in patients with cancer. J Clin Oncol 2006; 24:25-35. [PMID: 16314617].
- Kulke MH, Lenz HJ, Meropol NJ. Activity of Sunitinib in patients with advanced neuroendocrine tumors. J Clin Oncol 2008; 26:3403-3410. [PMID: 18612155].
- Raymond E, Dahan L, Raoul JL. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:501-513. [PMID: 21306237].
- Faivre S, Niccoli P, Castellano D, Valle JW, Hammel P, Raoul JL, et al. Sunitinib in Pancreatic Neuroendocrine Tumors: Updated Progression-Free Survival and Final Overall Survival from a Phase III Randomized Study. Ann Oncol 2016; 28:339-343 [PMID: 27836885].
- Yao JC, Lombard-Bohas C, Baudin E. Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 2010; 28:69-76 [PMID: 19933912].
- Yao JC, Phan AT, Chang DZ. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low- to intermediate-grade neuroendocrine tumors: results of a phase II study. J Clin Oncol 2008; 26:11-4318. [PMID: 18779618].
- O'Donnell A, Faivre S, Burris HA III. Phase I pharmacokinetic and pharmacodynamics study of the oral mammalian target of rapamycin inhibitor Everolimus in patients with advanced solid tumors. J Clin Oncol 2008; 26:1588-1595. [PMID: 18332470].
- von Wichert G, Jehle PM, Hoeflich A, Koschnick S, Dralle H, Wolf E, et al. Insulin-like growth factor-I is an autocrine regulator of chromogranin A secretion and growth in human neuroendocrine tumor cells. Cancer Res 2000; 60:4573-4581. [PMID: 10969809] .
- Moreno A, Akcakanat A, Munsell MF, Soni A, Yao JC, Meric-Bernstam F. Antitumor activity of rapamycin and octreotide as single agents or in combination in neuroendocrine tumors. Endocr Relat Cancer 2008; 15:257-266. [PMID: 18310292].
- Missiaglia E, Dalai I, Barbi S, Beghelli S, Falconi M, della Peruta M, et al. Pancreatic endocrine tumors:expression profiling evidences a role for AKT-mTOR pathway. J Clin Oncol 2010; 28:245-255. [PMID: 19917848].
- Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:514-523. [PMID: 21306238] .
- Yao JC, Pavel M, Lombard-Bohas C. Everolimus for the Treatment of Advanced Pancreatic Neuroendocrine Tumors:Overall Survival and Circulating Biomarkers From the Randomized, Phase III RADIANT-3 Study. J Clin Oncol 2016; JCO680702. [PMID: 27621394].
- Ohmoto A, Rokutan H, Yachida S. Pancreatic Neuroendocrine Neoplasms: Basic Biology, Current Treatment Strategies and Prospects for the Future. Int J Mol Sci 2017; 13:18. [PMID: 28098761].
- Kulke MH. Sequencing and combining systemic therapies for pancreatic neuroendocrine tumors. J Clin Oncol 2015; 10:1534-8. [PMID: 25870092].
- Kulke MH, Bergsland EK, Yao JC. Glycemic control in patients with insulinoma treated with Everolimus. N Engl J Med 2009; 360:195. [PMID: 19129539].
- Fiebrich HB, Siemerink EJ, Brouwers AH. Everolimus induces rapid plasma glucose normalization in insulinoma patients by effects on tumor as well as normal tissues. Oncologist 2011; 16:783. [PMID: 21482586].
- Krug S, Boch M, Daniel H, Nimphius W, Müller D, Michl P, et al. Streptozocin-Based Chemotherapy in Patients with Advanced Neuroendocrine Neoplasms--Predictive and Prognostic Markers for Treatment Stratification. PLoS One 2015; 10:e0143822. [PMID: 26630134].
- Kouvaraki MA, Ajani JA, Hoff P, Wolff R, Evans DB, Lozano R, et al. Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 2004; 22:4762-4771. [PMID: 15570077].
- Dilz LM, Denecke T, Steffen IG. Streptozocin/5-fluorouracil chemotherapy is associated with durable response in patients with advanced pancreatic neuroendocrine tumours.Eur J Cancer 2015; 51:1253-62. [PMID: 25935542].
- Strosberg JR, Fine RL, Choi J. First-line chemotherapy with capecitabine and Temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer 2011; 117:268. [PMID: 20824724].
- Fine RL, Gulati AP, Krantz BA. Capecitabine and Temozolomide (CAPTEM) for metastatic, well-differentiated neuroendocrine cancers. The Pancreas Center at Columbia University experience. Cancer Chemother Pharmacol 2013; 71:663–670.[PMID: 23370660].
- Saif MW, Kaley K, Brennan M, Garcon MC, Rodriguez G, Rodriguez T. A retrospective study of capecitabine/Temozolomide (CAPTEM) regimen in the treatment of metastatic neuroendocrine tumors (pNETs) after failing previous therapy. JOP 2013; 14:498–501. [PMID: 24018594].
- Fine RL, Gulati AP, Tsushima D, Mowatt KB, Oprescu A, Bruce JN, et al. Prospective phase II study of capecitabine and Temozolomide (CAPTEM) for progressive, moderately, and well-differentiated metastatic neuroendocrine tumors; Abstract 179 presented at: Gastrointestinal Cancers Symposium 2014..
- Peixoto RD, Noonan KL, Pavlovich P, Kennecke HF, Lim HJ. Outcomes of patients treated with capecitabine and Temozolomide for advanced pancreatic neuroendocrine tumors (PNETs) and non-PNETs. J Gastrointest Oncol 2014; 5:247–252. [PMID: 25083296].
- Abbasi S, Kashashna A, Albaba H. Efficacy of capecitabine and Temozolomide combination in well-differentiated neuroendocrine tumors: Jordan experience. Pancreas 2014; 43:1303-1305. [PMID: 25036906].
- Ramirez RA, Boudreaux JP, Wang YZ. Combination capecitabine/Temozolomide (CAPTEM) in patients with neuroendocrine tumors (NETs): a single institution review. J Clin Oncol 2015; 33(Suppl) abstr e15184..
- Spada F, Antonuzzo L, Marconcini R. Chemotherapy with capecitabine plus Temozolomide (CAP-TEM) in patients with advanced neuroendocrine neoplasm (NENs):an Italian multicenter retrospective analysis. J Clin Oncol 2015; 33(Suppl) abstr e15174..
- Kotteas EA, Syrigos KN, Saif MW. Profile of capecitabine/Temozolomide combination in the treatment of well-differentiated neuroendocrine tumors. Onco Targets Ther 2016; 9:699–704. [PMID: 26929640].
- Strosberg JR, Cives M, Brelsford M. Identification of response predictors to capecitabine/Temozolomide in metastatic pancreatic neuroendocrine tumors. J Clin Oncol 2015; 33(Suppl) abstr 4099..
- Ramanathan RK, Cnaan A, Hahn RG, Carbone PP, Haller DG. Phase II trial of Dacarbazine (DTIC) in advanced pancreatic islet cell carcinoma. Study of the Eastern Cooperative Oncology Group-E6282. Ann Oncol 2001; 12:1139–43. [PMID: 11583197].
- Okusaka T, Ueno H, Morizane C. Cytotoxic chemotherapy for pancreatic neuroendocrine tumors. J Hepatobiliary Pancreas Sci 2015; 22:628-33. [PMID: 25940377].
- Hobday TJ, Qin R, Reidy-Lagunes D, Moore MJ, Strosberg J, Kaubisch A, et al. Multicenter phase II trial of temsirolimus and bevacizumab in pancreatic neuroendocrine tumors. J Clin Oncol 2015; 33:1551-1556. [PMID: 25488966].
- Kulke MH, Niedzwiecki D, Foster NR, Fruth B, Kunz PL, Kennecke HF, et al. Randomized phase II study of everolimus (E) versus everolimus plus bevacizumab (E + B) in patients (pts) with locally advanced or metastatic pancreatic neuroendocrine tumors (pNET), CALGB 80701 (Alliance). J Clin Oncol 2015; 33 (Suppl.) abstr 4005.
- Phan AT, Halperin DM, Chan JA, Fogelman DR, Hess KR, Malinowski P, et al. Pazopanib and depot octreotide in advanced, well-differentiated neuroendocrine tumours:A multicentre, single-group, phase 2 study. Lancet Oncol 2015; 16:695–703. [PMID: 25956795].
- Turner NC, Strauss SJ, Sarker D, Gillmore R, Kirkwood A, Hackshaw A, et al. Chemotherapy with 5-fluorouracil, cisplatin and streptozocin for neuroendocrine tumours. Br J Cancer 2010; 102:1106–12. [PMID: 20234360].
- Valkema R, De Jong M, Bakker WH, Breeman WA, Kooij PP, Lugtenburg PJ, et al. Phase I study of peptide receptor radionuclide therapy with [In-DTPA]octreotide:the Rotterdam experience. Semin Nucl Med 2002; 32:110-22. [PMID: 11965606].
- Schillaci O, Corleto VD, Annibale B, Scopinaro F, Delle Fave G. Single photon emission computed tomography procedure improves accuracy of somatostatin receptor scintigraphy in gastro-entero pancreatic tumours. Ital J Gastroenterol Hepatol 1999; 31 Suppl 2:S186. [PMID: 10604127] .
- Gibril F, Reynolds JC, Doppman JL, Chen CC, Venzon DJ, Termanini B, et al. Somatostatin receptor scintigraphy:its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas. A prospective study. Ann Intern Med 1996; 125:26. [PMID: 8644985] .
- Hörsch D, Ezziddin S, Haug A, Gratz KF, Dunkelmann S, Miederer M, et al. Effectiveness and side-effects of peptide receptor radionuclide therapy for neuroendocrine neoplasms in Germany:A multi-institutional registry study with prospective follow-up. Eur J Cancer 2016; 58:41. [PMID: 26943056].
- Imhof A, Brunner P, Marincek N, Briel M, Schindler C, Rasch H, et al. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J Clin Oncol 2011; 29:2416. [PMID: 21555692].
- Kwekkeboom DJ, de Herder WW, Kam BL, van Eijck CH, van Essen M, Kooij PP, et al. Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3] Octreotide: toxicity, efficacy, and survival. J Clin Oncol 2008; 26:2124-2130. [PMID: 18445841].
- Bodei L, Kwekkeboom DJ, Kidd M, Modlin IM, Krenning EP. Radiolabeled Somatostatin Analogue Therapy Of Gastroenteropancreatic Cancer. Semin Nucl Med 2016; 46:225-238. [PMID: 27067503].
- Ezziddin S, Khalaf F, Vanezi M, Haslerud T, Mayer K, Al Zreiqat A, et al. Outcome of peptide receptor radionuclide therapy with 177Lu-octreotate in advanced grade 1/2 pancreatic neuroendocrine tumours. Eur J Nucl Med Mol Imaging 2014; 41:925-33. [PMID: 24504504].
- Delpassand ES, Samarghandi A, Zamanian S, Wolin EM, Hamiditabar M, Espenan GD, et al. Peptide receptor radionuclide therapy with 177Lu-DOTATATE for patients with somatostatin receptor-expressing neuroendocrine tumors: the first US phase 2 experience. Pancreas 2014; 43:518-25. [PMID: 24632546] .
- Sansovini M, Severi S, Ambrosetti A, Monti M, Nanni O, Sarnelli A, et al. Treatment with the radiolabelled somatostatin analog Lu-DOTATATE or advanced pancreatic neuroendocrine tumors. Neuroendocrinology. 2013; 97:347-54. [PMID: 23392072].
- Sansovini M, Severi S, Ianniello A, Nicolini S, Fantini L, Mezzenga E, et al. Long-term follow-up and role of FDG PET in advanced pancreatic neuroendocrine patients treated with 177Lu-D OTATATE. Eur J Nucl Med Mol Imaging 2017; 44:490-499. [PMID: 27807661].
- Ezziddin S, Attassi M, Yong-Hing CJ, Ahmadzadehfar H, Willinek W, Grünwald F, et al. Predictorsof long-term outcome in patients with well-differentiated gastroenteropancreatic neuroendocrine tumors after peptide receptorradionuclide therapy with 177Lu-octreotate. J Nucl Med 2014; 55:183-90. [PMID: 24434296].
- van Vliet EI, van Eijck CH, de Krijger RR, Nieveen van Dijkum EJ, Teunissen JJ, Kam BL, et al. Neoadjuvant Treatment of Nonfunctioning Pancreatic Neuroendocrine Tumors with [177Lu-DOTA0,Tyr3] Octreotate. J Nucl Med 2015; 56:1647-53. [PMID: 26272813].

