Alexios S Strimpakos1, Konstantinos N Syrigos1, Muhammad Wasif Saif2
1Oncology Unit, Third Department of Medicine, University of Athens, Sotiria General Hospital. Athens, Greece
2Columbia University College of Physicians and Surgeons and New York Presbyterian Hospital. New York, NY, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Columbia University College of Physicians and Surgeons
New York Presbyterian Hospital
MHB, 6N-435; New York, NY 10032; USA
Phone: +1-212.305.4954
Fax: +1-212.3050.3035
E-mail: mws2138@columbia.edu
Neuroendocrine tumors of pancreas (PNET) are very rare, consisting of heterogeneous histological subtypes with a variable natural history and different clinical manifestations. Although the vast majority of these neoplasms are sporadic, it is possible to be part of a genetic syndrome such as multiple endocrine neoplasia 1 (MEN-1) or tuberous sclerosis (TSC). When systemic treatment is required the options are limited and management strategy is generally based on experts’ consensus or clinical experience. The prognosis is usually better than in pancreatic adenocarcinoma, though poorly differentiated PNET behave aggressively and survival is shortened. Since last year, there has been a significant advance in the management of PNET, after reported data confirmed the efficacy of everolimus, an mTOR inhibitor, in patients with advanced disease. At the 2011 American Society of Clinical Oncology (ASCO) Gastrointestinal Symposium, updated results of the phase III trial (RADIANT-3) regarding the efficacy of everolimus in PNET (Abstract #158) were reported, along with the results of a subgroup analysis of the Japanese patients enrolled in this study (Abstract #289). Another agent with promising activity in PNET which will be discussed in this review is sunitinib, a biological agent with multikinase inhibitor properties (Abstract #244).
Keywords
everolimus; Molecular Targeted Therapy; Neuroendocrine Tumors; Pancreatic Neoplasms; sunitinib; TOR Serine-Threonine Kinases
Abbreviations
NET: neuroendocrine tumor; RADIANT: RAD001 In Advanced Neuroendocrine Tumors
What Did We Know Before the 2011 ASCO GI Cancer Symposium?
Pancreatic neuroendocrine tumors (PNET) consist of a variety of histological subtypes, including insulinoma, gastrinoma, non functioning PNETs and poorly differentiated neuroendocrine tumors (NETs) which show a high malignant potential [1]. Providing the disease is diagnosed at an early stage, resection if feasible offers the best chances of cure. At advanced stages systemic treatment is opted. Traditionally, chemotherapy based on etoposide, platinum agents, anthracycline, streptozocin and 5-fluoropyrimidine had been the choice of most oncologists in advanced disease. At the European Society of Medical Oncology 2010 Annual Meeting, the results of a phase III study on PNET (RAD001 In Advanced Neuroendocrine Tumors; RADIANT-3) were presented and suggested a significant clinical benefit and improvement of progression free survival of patients treated with everolimus (also known as RAD001) as compared to the control group [2]. Apart from the mTOR inhibitor, it has been suggested previously that small molecule multikinase inhibitors (sunitinib or sorafenib) or antibodies targeting angiogenesis (bevacizumab) may be of value and deserve further testing in this disease [3, 4].
What Did We Learnt from the 2011 ASCO GI Cancer Symposium?
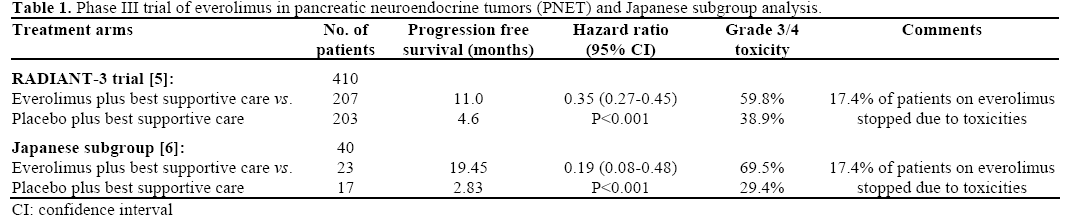
Herein, we present findings and updated results of studies testing novel targeted agents in a poorly understood and diverse disease as PNET. In Table 1, we summarize the results from the phase III trial (RADIANT-3) on PNET.
RADIANT-3 Trial: Updated Results and Subgroup Analysis (Abstracts #158 and #289) [5, 6]
Shah et al. [5] reported the results of this randomized, double-blind, phase III study that was designed for patients with advanced PNET (low or intermediate grade). Four hundred and ten patients were randomized to either everolimus (10 mg/day orally) plus best supportive care or placebo plus best supportive care. Patients were allowed to somatostatin analogs if symptomatic. Progression free survival was the primary end-point. At progression, patients were unblinded and if on the placebo arm were offered the investigational drug. The authors reported a 6.4 months improvement of progression free survival (hazard ratio, HR: 0.35; 95% CI: 0.27-0.45; P<0.0001) which met the predefined criteria. The progression free survival prolongation was observed in all patients’ subgroups and independent from use of somatostatin analogues or other factors. The commonest toxicities observed were stomatitis, rash, diarrhea, fatigue, and chest infections whereas the most serious but of low frequency were stomatitis, anemia, and hyperglycemia.
A subgroup analysis was performed by Ito et al. on Japanese patients enrolled in the same RADIANT-3 study [6]. Forty patients were treated in this study (23 in the everolimus arm and 17 in the placebo arm). The authors tested the efficacy and safety profile in this genetically homogeneous subgroup population. They reported a statistically significant improvement of progression free survival by almost 17 months (19.45 vs. 2.83 months) and an 81% reduction of risk of progression or death (HR: 0.19; 95% CI: 0.08-0.48; P<0.001). The treatment was tolerated by the majority of patients (17% stopped everolimus due to toxicities), though about 74% of patients developed stomatitis of all grades and 17% grade 3 or 4 neutropenia. In summary, the observed benefit of everolimus in the RADIANT-3 trial was also confirmed in the Japanese patients, though the sample size was rather small for accurate conclusions. Of concern, was the increasing rate of adverse events (69% grade 3/4 toxicities in total) slightly higher than the reported in the trial (59.8%) but again it is not possible from the current data to suggest any particular pharmacogenetic causes for this difference.
Small Molecules Multikinase Inhibitors in PNET (Abstract # 244) [7]
Strosberg et al. from the Lee Moffitt Cancer Centre conducted a study on advanced NET patients who underwent a series of arterial chemoembolization for hepatic metastases. One week after each session of arterial chemoembolization patients were assigned to receive sunitinib 50 mg orally until disease progression or up to a maximum of 8 cycles. The working hypothesis was that sunitinib following arterial chemoembolization will delay tumor revascularization and extend progression-free survival which was the primary end point. Investigators also evaluated efficacy and overall survival. Out of the total 39 patients with NET, 10 were diagnosed with advanced pancreatic NET. The authors reported a 72% (28/39 patients) partial response by radiological criteria and 20% disease stabilization (8/39). The median progression free survival was 18 months and the progression free survival at one year as high as 72%. The overall survival at 1 and 2 years was also high at 94% and 78%, respectively.
An interesting observation that may explain in part the encouraging results was that the serum VEGF levels following arterial chemoembolization were increased by about 34%, hence the role of systemic anti-VEGF treatment in this setting.
Discussion
Pancreatic NET consist a diverse constellation of subgroups with variable clinical course, manifestations and of course management. The mTOR signaling pathway plays a significant role in many cellular functions. Dysregulation of mTOR pathway at some level, inactivation of tuberous sclerosis complex II (TSC II) and phosphatase and tensin homolog (PTEN) have been recognized to contribute in PNET pathophysiology as well the survival and progression of many solid tumor [8]. The concept of targeting a specific molecule of a deranged pathway has been very attractive but the results have been somehow disappointing as in most cases there is a significant crosstalk between the various molecular channels through which the aberrant signals travel. On the other hand, the efforts to combine a number of novel agents are often limited by the increasing risk of toxicities. Furthermore, the results are often modest in pharmacoeconomic terms, which restrict their clinical applications and final approval from the authorities. Finally, investigators and patients participating in clinical studies should be proud of the very significant advances that have taken place in oncology over the last decade or so. Through research, more exciting findings are expected in future, that will justify the efforts made at the multiple levels of science from bench to bedside.
Conflict of interest
The authors have no potential conflict of interest
References
- Ehehalt F, Saeger HD, Schmidt CM, Grutzmann R. Neuroendocrine tumors of the pancreas. Oncologist 2009; 14:456-67. [PMID 19411317]
- Yao J, Shah M, Ito T, Lombard-Bohas C, Wolin E, Van Cutsem E, et al. A randomized, double-blind, placebo-controlled, multicenter phase III trial of everolimus in patients with advanced pancreatic neuroendocrine tumors (PNET) (RADIANT-3). Ann Oncol 2010; 21(Suppl 8):viii4-5.
- Valle J, Faivre S, Raoul J, Bang Y, Patyna S, Lu D, et al. Phase III trial of sunitinib (SU) versus placebo (PLO) for treatment of pancreatic neuroendocrine tumors (NET): impact of somatostatin analogue (SSA) treatment on progression-free survival (PFS). Ann Oncol 2010; 21(Suppl 8):viii264.
- Castellano D, Capdevilla J, Salazar R, Sastre J, Alonso V, M. Llanos M, et al. Sorafenib and bevacizumab combination targeted therapy in advanced neuroendocrine tumor: a phase II study of Spanish neuroendocrine tumor group (GETNE-0801). Ann Oncol 2010; 21(Suppl 8):viii265.
- Shah MH, Ito T, Lombard-Bohas C, WolinEM, Van Cutsem E, Sachs C, et al. Everolimus in patients with advanced pancreatic neuroendocrine tumors (pNET): Updated results of a randomized, double-blind, placebo-controlled, multicenter phase III trial (RADIANT-3). J Clin Oncol 2011; 29(Suppl. 4):Abstract 278.
- Ito T, Okusaka T, Ikeda M, Tajima T, Kasuga A, Fujita Y, Furuse Y. Everolimus versus placebo in Japanese patients with advanced pancreatic neuroendocrine tumors (pNET): Japanese subgroup analysis of RADIANT-3. J Clin Oncol 2011; 29(Suppl. 4):Abstract 289.
- Strosberg JR, Cheema A, Campos T, Valone T, KvolsLK. Phase II study of sunitinib malate following hepatic artery embolization for metastatic neuroendocrine tumors. J Clin Oncol 2011; 29(Suppl. 4):Abstract 244.
- Strimpakos AS, KarapanagiotouEM, Saif MW, Syrigos KN. The role of mTOR in the management of solid tumors: an overview. Cancer Treat Rev 2009; 35: 148-59. [PMID 19013721]

