Mohamedtaki Abdulaziz Tejani1, Muhammad Wasif Saif2
1Division of Hematology and Oncology, University of Rochester. Rochester, NY, USA. 2Section of GI Cancers and Experimental Therapeutics, Tufts University School of Medicine. Boston, MA, USA
- *Corresponding Author:
- Mohamedtaki Abdulaziz Tejani
Division of Hematology and Oncology
University of Rochester Medical Center
610 Elmwood Avenue, Box 704
Rochester, NY 14642; USA
Phone: +1-585.275.9484
Fax: +1-585.276.0350
E-mail: mohamed_tejani@urmc.rochester.edu
Keywords
capecitabine; Neuroendocrine Tumors; temozolomide
Abbreviations
CAPTEM: capecitabine and temozolomide
INTRODUCTION
Well-differentiated tumors of neuroendocrine origin within the digestive system usually arise in the gastrointestinal tract (predominantly small bowel) or pancreas. Pancreatic neuroendocrine tumors (pNETs), formerly known as islet cell tumors, are rare and make up about 1% of newly diagnosed pancreatic cancers. pNETs tend to have a worse prognosis that carcinoid tumors [1] and have a higher response rates with most antineoplastic agents. pNETs can be non-functional or functional (insulinoma, glucagonoma and gastrinoma being among the most common).
Treatment approach is dependent on stage and symptom status. For resectable tumors, surgery will generally provide prolonged survival. Metastasectomy, when feasible, can also provide prolonged control of symptoms and disease-free survival for patients with well-differentiated tumors. For patients with symptomatic disease, treatment with a somatostatin analog is recommended which also offers a progression-free survival benefit [2]. Recent trials have demonstrated benefit in outcomes with the use of sunitinib [3] and everolimus [4] among patients with pNETs.
The benefit of conventional cytotoxic chemotherapy is less clear. Small studies have shown modest response rates with agents such as fluoropyrimidines, doxorubicin and streptozocin and these are generally reserved for patients for whom there are no other treatment options. In this article, we review data presented at the 2014 ASCO Gastrointestinal Cancers Symposium about use of chemotherapy in pNETs.
What We Have Learned at the 2014 ASCO Gastrointestinal Cancers Symposium
Prospective Phase II Study of Capecitabine and Temozolomide (CAPTEM) for Progressive Moderately and Well-Differentiated Metastatic Neuroendocrine Tumors (Abstract #179 [5]).
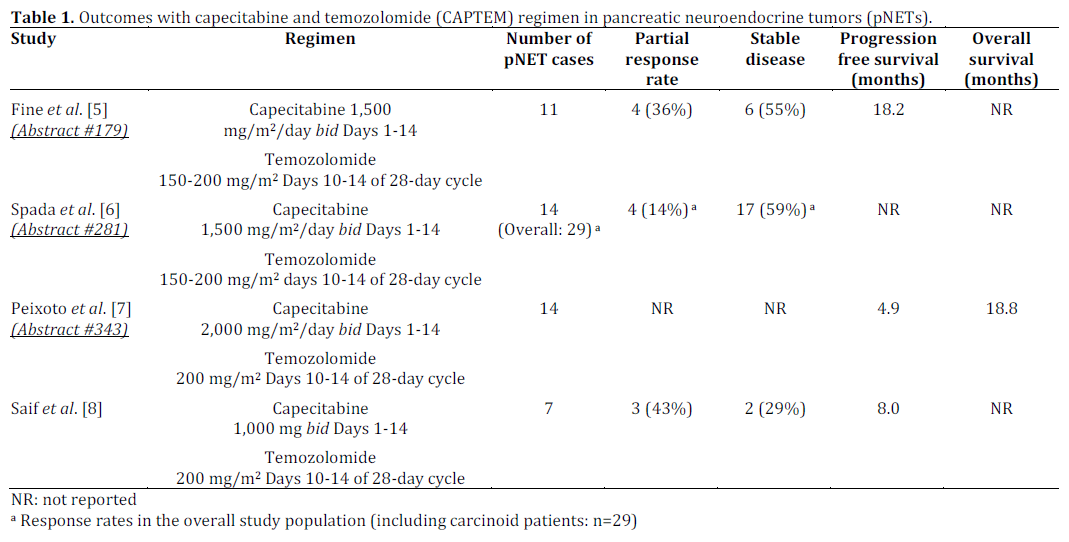
In this oral presentation, Fine et al. presented results from an interim analysis of their ongoing phase II trial utilizing capecitabine and temozolomide among 28 patients with metastatic well-moderately differentiated neuroendocrine tumors. Doses used were capecitabine 1,500 mg/m2/day divided bid (maximum 2,500 mg/day) on days 1-14 and temozolomide 150-200 mg/m2 divided bid on Days 10-14, with two weeks off in a 28-day cycle. Eleven patients with pNET were included in their study: 4 patients (36%) had partial responses, an additional 6 patients (55%) had stable disease and one had progressive disease (9%). Ongoing progression free survival for these patients was excellent (longer than 18.2 months). Most common grade 3 and 4 toxicities were lymphopenia, thrombocytopenia and diarrhea. The authors concluded that CAPTEM is an effective, well-tolerated regimen for patients with progressive neuroendocrine tumors.
Capecitabine plus Temozolomide in Patients with Advanced Neuroendocrine Neoplasms: An Italian Multicenter Retrospective Analysis (Abstract #281 [6]).
Spada et al. presented a retrospective study looking at the use of CAPTEM among their patients with well-differentiated neuroendocrine tumors. Clinical data from 29 patients were reviewed of whom 14 had pNET. Doses used were capecitabine 1,500 mg/m2/day divided bid on Days 1-14 and temozolomide 150-200 mg/m2/day on Days 10-14 of each 28-day cycle. The overall response rate was 14% and stable disease rate was 59%. Most common grade 3 toxicity was thrombocytopenia. Of note, all patients with partial response had MGMT gene inactivation and TS-polymorphism which the authors conclude could serve as a predictive biomarker.
Outcome of Patients Treated with Capecitabine and Temozolomide for Advanced Pancreatic Neuroendocrine Tumors (pNETs) and non-pNETs (Abstract #343 [7]).
Another retrospective study came from Peixoto et al. who described characteristics and outcomes among patients treated with CAPTEM for welldifferentiated neuroendocrine tumors at 6 provincial cancer treatment centers in Canada. Twenty-nine patients were included and 14 had tumors originating in the pancreas. Doses were capecitabine 2,000 mg/m2/day divided bid on Days 1-14 and temozolomide 200 mg/m2 on Days 10-14 of each 28-day cycle. Response rates were not provided in this abstract. Progression free survival and overall survival for patients with pNET was 4.9 months and 18.8 months, respectively. The authors concluded that CAPTEM shows good activity among patients with well-differentiated neuroendocrine tumors.
Discussion
All the three abstracts reviewed here present outcomes of similarly dosed CAPTEM regimen for pancreatic neuroendocrine tumors. Limitations of these studies are relatively small numbers, retrospective nature (Abstracts #281 and #343) and non-randomized study design (Abstract #179). Also, despite a similar patient population, response rates reported by Fine et al. are much higher than those reported in other studies and reasons for this are unclear. Results observed in these abstracts are in line with our group’s previously reported experience with CAPTEM among 7 patients with pNET [8] (Table 1). We used a similar dosing regimen with 3 patients achieving partial response and 2 patients with stable disease. More definitive data about activity of this regimen will emerge from the ongoing cooperative group trial “Temozolomide With or Without Capecitabine in Treating Patients With Advanced Pancreatic Neuroendocrine Tumors” [9]. In the interim, it is our opinion that these studies demonstrate that CAPTEM combination is a reasonable choice for fit patients with advanced, progressive disease who have exhausted all other standard and protocol treatment options.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Panzuto F, Nasoni S, Falconi M, et al. Prognostic factors and survival in endocrine tumor patients: comparison between gastrointestinal and pancreatic localization. Endocr Relat Cancer 2005; 12: 1083.
- Rinke A, Muller HH, Schade-Brittinger C, et al. Placeb-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009; 27: 4656.
- Raymond E, Dahan L, Raoul JL, et al. Sunitinib maleate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364: 501.
- Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011; 364: 514.
- Fine RL, Gulati AP, Tsushima D, et al. Prospective Phase II study of capecitabine and temozolamide for progressive, moderately and well-differentiated metastatic neuroendocrine tumors. J Clin Oncol 2014; 32: abstract 179
- Spada F, Fumagalli C, Antonuzzo L, et al. Capecitabine and temozolamide in patients with advanced neuroendocrine neoplasms: An Italian multicenter retrospective analysis. J Clin Oncol 2014; 32: abstract 281.
- Peixoto RD, Noonan K, Kennecke HF, et al. Outcomes of patients treated with capecitabine and temozolamide for advanced pancreatic neuroendocrine tumors (pNETs) and non-pNETs.J Clin Oncol 2014; 32: abstract 343.
- Saif MW, Kaley K, Brennan M, Garcon MC, Rodriguez G, Rodriguez T. A retrospective study of capecitabine/temozolamide (CAPTEM) regimen in the treatment of metastatic pancreatic neuroendocrine tumors after failing previous therapy. JOP. J Pancreas (Online) 2013; 14:498-501.
- U.S. National Institutes of Health. Temozolomide with or without capecitabine in treating patients with advanced pancreatic neuroendocrine tumors. ClinicalTrials.gov (NCT 01824875). Accessed January 28, 2014 https://www.clinicaltrials.gov/ct2/show/NCT01824875?term=0 1824875&rank=1

