Keywords
Colorectal Neoplasms; Neoplasm Metastasis; Pancreatectomy; Pancreatic Neoplasms
INTRODUCTION
The pancreas is an uncommon location for a solitary metastasis from other primary cancers [1]. In a large autopsy series, the prevalence of pancreatic metastasis was described to from approximately 6 to 11% [2]. The metastases are usually from a primary tumor of the kidney, lung, breast, gastrointestinal tract (stomach, small bowel and colorectum) or melanoma [3]. Reports of a solitary resectable pancreatic metastasis from colorectal cancer are rare [4, 5, 6]. In a recent review, only 24 cases of colorectal metastases to the pancreas were reported and, among these metastases, those from the colon were more frequent than those from the rectum (17:7) [7]. While some of the metastases from colorectal cancer to the liver and lung are being successfully treated by resection, the benefit of pancreatic resection appears unclear [5, 7].
CASE REPORT
On August 2000, a 58-year-old female presented with large bowel obstruction, secondary to a malignant growth in the descending colon. She underwent an emergency left hemicolectomy and made an uneventful recovery. Histology showed moderately differentiated adenocarcinoma involving the serosal fat. The resected margins were free of tumor; however, 3 of the 18 regional lymph nodes were positive. The pathological staging was T3 N1 M0 and she received adjuvant chemotherapy which involved 6 cycles of FOLFOX chemotherapy (5-flurouracil and folinic acid and oxaliplatin). She was monitored regularly with ultrasound of the abdomen, carcinoembryonic antigen levels biannually and colonoscopy yearly for 2 years. The ultrasound of the abdomen was normal, carcinoembryonic antigen levels ranged between 2.2 and 4.7 μg/L (reference range: 0-2.5 μg/L) and colonoscopy showed small polyps which were benign. In March 2009 there was a sharp rise in carcinoembryonic antigen levels to 25 μg/L associated with a vague backache. A CT scan of the abdomen revealed a mixed density mass lesion with soft tissue and cystic components, measuring 6.8x4.8 cm in the area of the tail of the pancreas with possible left perinephric fat infiltration (Figure 1). No other metastasis was detected. A CT-guided biopsy suggested the possibility of adenocarcinoma. In April 2009, she underwent an exploratory laparotomy which revealed that the tumor in the distal pancreas was infiltrating the perinephric fat, the posterior wall of the stomach and the great omentum. She underwent a distal pancreatectomy and excision of the involved segment of the stomach, omentum and perinephric fat (Figures 2 and 3). Histology was reported as moderately differentiated adenocarcinoma with infiltration into the perinephric fat and the resected segment of the stomach. The adenocarcinoma was metastatic tumor from the colon confirmed by its histological appearance and strong positivity to cytokeratin 20 (Figures 4 and 5). The margins of the resected pancreas and stomach were clear of the tumor. She made an uneventful recovery. She received palliative chemotherapy in the form of 5 cycles of 5- flurouracil, oxaliplatin and bevacizumab. In October 2009, she presented with a mass in the left hypochondrium which on CT of the abdomen was found to be recurrent disease. She was provided care for the terminally ill and she ultimately died in January 2010, nine months after the resection of the metastatic tumor.
Figure 1. Mixed density lesion seen in the tail of the pancreas:
metastatic tumor from cancer of the descending colon.
Figure 2. Distal pancreatectomy specimen with a metastatic
pancreatic tumor from cancer of the descending colon.
Figure 3. Cut section of the distal pancreatectomy specimen
revealing the cystic necrotic center of the metastatic tumor from
cancer of the descending colon.
Figure 4. Metastatic adenocarcinoma of the pancreas (H&E x20).
Figure 5. Metastatic adenocarcinoma of the pancreas positive for
cytokeratin 20, confirming the colon as the primary site o the tumor.
DISCUSSION
Metastatic cancers to the pancreas have been reported in about 2% of all pancreatic malignancies, metastasis from renal cancer being predominant [8]. However, in an autopsy study of 690 cases in patients with malignant tumors, metastasis to the pancreas was found in 15% of cases [1]. Metastatic lesions to the pancreas from colorectal cancer account for 1.7% of all metastases [9]. Pancreatic resection for a metastatic tumor was carried out in 3.3% (18 of 546 pancreatic resections for pancreatic tumors) in one of the reports of which 50% were from colorectal cancer [7]. Patients with pancreatic metastases from colorectal cancer could be either symptomatic or asymptomatic; suspicion is usually raised when a pancreatic mass is detected during routine follow-up of patients following a colectomy for colorectal cancer whose CEA levels are rising as in our patient. The widespread usage of imaging techniques in asymptomatic patients together with greater awareness of these entities may explain the increasing number of pancreatic resections for metastatic tumors to the pancreas in high volume centers [10].
The time interval between the diagnosis of colorectal cancer and the detection of pancreatic metastasis varies widely [7]. Although a long disease-free interval may be frequent for renal cell carcinoma, it is unusual for colon cancer [7, 8]. The median interval in a recent review of 24 cases for colorectal metastasis to the pancreas was found to be 24 months in sharp contrast to metastasis from renal cell carcinoma where it was 120 months [7, 8]. The interval of 9 years in our patient was the second longest interval, following another report of 11 years [11]. Synchronous pancreatic metastasis from colorectal cancer is rare [7].
Metastasis to the pancreas can be completely asymptomatic as has been documented in 35% of patients with metastasis from renal cell carcinoma [8]. However, in patients with metastasis from colorectal cancer, the rate of being asymptomatic is approximately 17% (4/24 cases) [7]. Metastasis in these asymptomatic patients is likely to be detected when a patient with previous colorectal cancer is found to have rising CEA levels during follow-up and, on further investigation, a pancreatic mass is detected [5, 6]. Investigations of a pancreatic mass both in symptomatic and asymptomatic patients would include abdominal ultrasonography and a CT scan which could reveal a hypodense lesion [8, 10]. While a contrast CT scan in renal cell carcinoma metastasis had either intense homogenous enhancement (in small lesions) or rim enhancement (in large lesions), with colorectal metastasis there was no difference in the outer region of the metastasis and the adjoining pancreatic tissue while the inner areas showed hypo-enhancement due to central necrosis [10]. Endoscopic ultrasound can b particularly useful for lesions in the head of the pancreas which would reveal a hypoechoic mass in comparison to the adjacent pancreatic tissue [11]. However, in view of the diagnostic difficulties in individual cases, many authors recommend establishing tissue diagnosis with fine needle aspiration biopsy which could be guided either by US, CT or endoscopic ultrasonography [8, 12]. Endoscopic ultrasonography assisted by fine needle aspiration cytology has been reported as a safe and minimally invasive method for diagnosing non-primary neoplasms [8, 12]. An accurate diagnosis is further facilitated by careful evaluation of the clinical history, cytomorphology and ancillary techniques, especially of those applied to cell block material including immunohistochemistry [8, 12]. The above investigations facilitate definitive tissue diagnosis and establish an assessment of resectability.
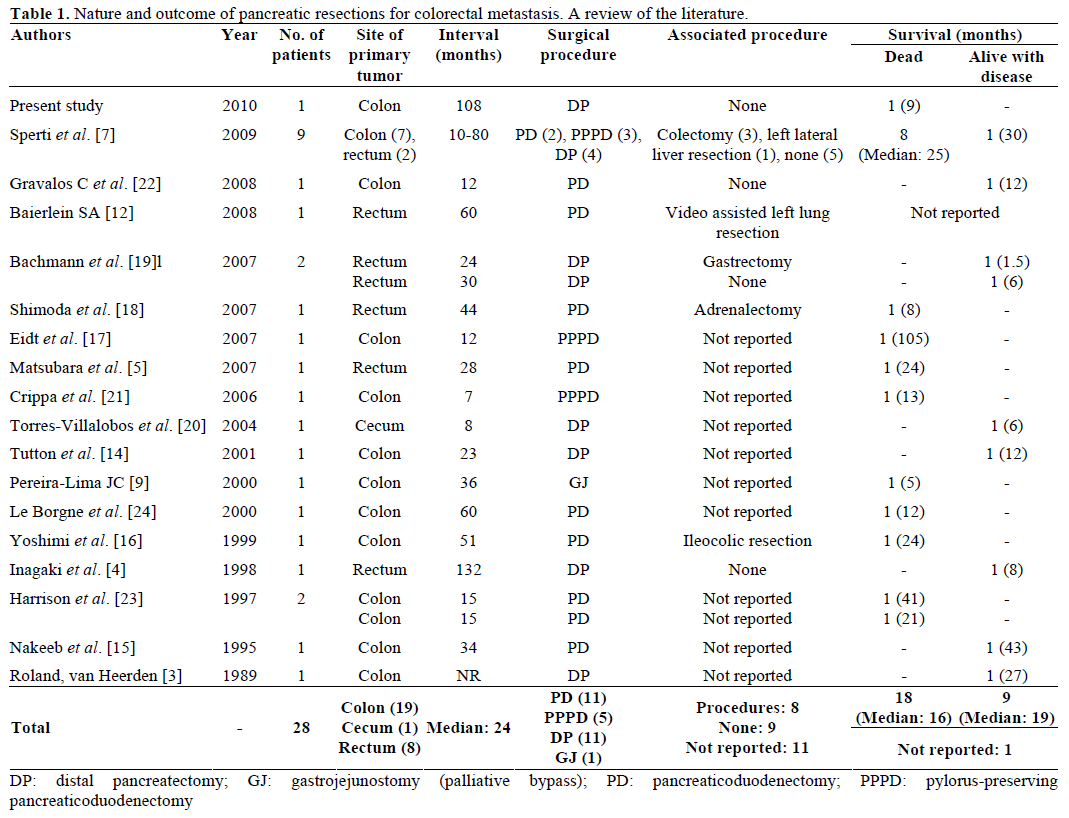
However, the need for a pretreatment tissue diagnosis of pancreatic tumors has been controversial. Although the predominant tissue type of a solid tumor is adenocarcinoma, tumors with cystic components, as in our patient, could represent other pathologies including metastatic tumor, serous cystadenoma, mucinous cystadenoma and intraductal mucinous neoplasia. While there are some who believe a negative biopsy would not change management in terms of resection, a tissue diagnosis could prove malignancy before a major operation, exclude unusual histology and possibly provide the surgeon and the patients with a strong rationale for taking an aggressive intraoperative approach. The risk of peritoneal seeding following fine needle aspiration cytology, though potential, is very minimal compared to that following a trucut biopsy. This is further reduced with endoscopic ultrasoundguided fine needle aspiration cytology feasible in pancreatic head lesions. Recently, 18-flurodeoxyglucose positron emission tomography has been reported to be useful not only in detecting pancreatic metastases but even in detecting incidental colon cancer while staging a pancreatic mass [7, 12, 13, 14]. The role of pancreatic resections for metastatic colorectal tumors is not well defined due to a paucity of such cases reported in the literature. Among the 28 cases reviewed (Table 1), the resections included pancreaticoduodenectomy, pylorus-preserving pancreaticoduodenectomy, distal pancreatectomy and palliative gastrojejunostomy in 11, 5, 11 and 1 patients, respectively. The primary tumor was located in the colon and rectum in 20 and 8 patients, respectively (Table 1). In a recent review, solitary pancreatic metastases were present in 17 patients, and 7 had other metastases which required an associated surgical procedure [7]. No perioperative mortality was reported in these patients [7]. Sixteen patients died from recurrent disease, the median survival time being 16.5 months (range 8-105 months) [7]. Only 5 studies reported cases of disease-free survival which ranged from 1.5 to 43 months (median 10 months) [14, 15, 16, 17, 18]. However, symptomatic patients had complete relief of symptoms (pain and jaundice) after surgery and continued to do so until recurrence of the disease [7].
However, the question arises as to whether these patients should be managed by a more conservative approach, such as chemotherapeutic management, and whether it may offer the same results as pancreatic resection with less morbidity. What makes this decision more difficult is the fact that the natural history of untreated patients with pancreatic metastases from colorectal cancer is unknown. Therefore, it is impossible to compare the survival rate of resected and unresected patients treated with surgical and chemotherapeutic agents as sufficient information about them is not yet available. The chemotherapeutic agents generally used would include 5-flurouracil, oxaliplatin and folinic acid (FOLFOX) or 5-flurouracil and folinic acid with irinotecan included (FOLFIRI) [3, 5, 14, 19, 20]. The response of the recurrent disease to chemotherapeutic agent is rarely reported; however, in one report, it was observed in only 1 of the 9 cases treated [7]. Chemotherapy does not generally provide the same encouraging results in pancreatic metastasis from colorectal cancer as are obtained in liver metastasis [7].
A review of the literature suggests that, while longterm survival following pancreatic resection for metastatic colorectal cancer is unlikely, a good quality of life is reported by most authors until recurrence occurs. Added to this is the fact that there were no perioperative mortalities [3, 4, 5, 6, 7, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24] and the morbidity reported was minimal [4, 15, 17, 19, 20, 22, 23, 24]. In one report in a patient with metastasis in pancreatic divisum, where only gastrojejunostomy was performed without a resection, the patient died in 5 months [9]. The median survival of patients following resection however has been reported to be 16.5 months [7]. Hence it is reasonable to believe that resection of a pancreatic metastasis from colorectal cancer is only a palliative procedure with long-time survival being an exceptional event. This is true both for solitary pancreatic metastases and for associated extrapancreatic tumor relapses. Good palliation and acceptable survival may be achieved even when a resection may involve both pancreatic and limited extrapancreatic masses when performed in patients with a good performance status.
CONCLUSION
Metastases to the pancreas from colorectal cancer are rare. They should be suspected in a patient presenting with a pancreatic mass following a previous colorectal resection for colonic malignancy especially if the CEA levels rise during follow-up. The usual interval between colorectal surgery and pancreatic metastasis is short, and a long duration of more than five years is exceptional. In the absence of widely metastatic disease, an aggressive surgical approach may offer good palliation and may play a role in the multimodality management of colorectal cancer.
Conflict of interest
The authors have no potential conflict of interest
References
- Nakamura E, Shimizu M, Itoh T, Manabe T. Secondary tumors of the pancreas: clinicopathological study of 103 autopsy cases of Japanese patients. PatholInt 2001; 51:686-90. [PMID 11696171]
- Rumancik WM, Megibow AJ, Bosniak MA, Hilton S. Metastatic disease to the pancreas: evaluation by computed tomography. J Comput Assist Tomogr 1984; 8:829-34. [PMID 6470248]
- Roland CF, van Heerden JA. Nonpancreatic primary tumors with metastasis to the pancreas.SurgGynecolObstet 1989; 168:345- 7. [PMID 2928909]
- Inagaki H, Nakao A, Ando N, Kotake K, Imaizumi T, Okuda N, et al. A case of solitary metastatic pancreatic cancer from rectal carcinoma: a case report. Hepatogastroenterology 1998; 45:2413-7. [PMID 9951934]
- Matsubara N, Baba H, Okamoto A, Kurata M, Tsuruta K, Funata N, Ashizawa K. Rectal cancer metastasis to the head of the pancreas treated with pancreaticoduodenectomy. J HepatobiliaryPancreatSurg 2007; 14:590-4. [PMID 18040627]
- Sperti C, Pasquali C, Chierichetti F, Ferronato A, Decet G, Pedrazzoli S. 18-fluorodeoxyglucose positron emission tomography in predicting survival of patients with pancreatic carcinoma. J GastrointestSurg 2003; 7:953-9. [PMID 14675704]
- Sperti C, Pasquali C, Berselli M, Frison L, Vicario G, Pedrazzoli S. Metastasis to the pancreas from colorectal cancer: is there a place for pancreatic resection? Dis Colon Rectum 2009; 52:1154-9. [PMID 19581861]
- Machado NO, Chopra P. Pancreatic metastasis from renal carcinoma managed by Whipple resection. A case report and literature review of metastatic pattern, surgical management and outcome. JOP. J Pancreas (Online) 2009; 10:413-8. [PMID 19581746]
- Pereira-Lima JC, Coral GP, Bayer LR, da Silva CP. Metastasis from colon carcinoma in the dorsal pancreas of a patient with pancreas divisum: report of a case. Hepatogastroenterology 2000; 47:554-5. [PMID 10791236]
- Palmowski M, Hacke N, Satzl S, Klauss M, Wente MN, Neukamm M, et al. Metastasis to the pancreas: characterization by morphology and contrast enhancement features on CT and MRI. Pancreatology 2008; 8:199-203. [PMID 18434757]
- Schauer M, Vogelsang H, Siewert JR. Pancreatic resection for metastatic renal cell carcinoma: a single center experience and review of the literature. Anticancer Res 2008; 28:361-5. [PMID 18383870]
- Baierlein SA, Wistop A, Looser C, Bussmann C, von Fl?e M, Peterli R. Primary pancreatic neoplasia or metastasis from colon carcinoma? ActaGastroenterolBelg 2008; 71:401-8. [PMID 19317283]
- Fletcher JW, Djulbegovic B, Soares HP, Siegel BA, Lowe VJ, Lyman GH, et al. Recommendations on the use of 18F-FDG PET in oncology. J Nucl Med 2008; 49:480-508. [PMID 18287273]
- Tutton MG, George M, Hill ME, Abulafi AM. Solitary pancreatic metastasis from a primary colonic tumor detected by PET scan: report of a case. Dis Colon Rectum 2001; 44:288-90. [PMID 11227949]
- Nakeeb A, Lillemoe KD, Cameron JL. The role of pancreaticoduodenectomy for locally recurrent or metastatic carcinoma to the periampullary region. J Am CollSurg 1995; 180:188-92. [PMID 7850053]
- Yoshimi F, Asato Y, Kuroki Y, Shioyama Y, Hori M, Itabashi M, et al. Pancreatoduodenectomy for locally advanced or recurrent colon cancer: report of two cases. Surg Today 1999; 29:906-10. [PMID 10489134]
- Eidt S, Jergas M, Schmidt R, Siedek M. Metastasis to the pancreas - an indication for pancreatic resection? Langenbecks Arch Surg 2007; 392:539-42. [PMID 17242893]
- Shimoda M, Kubota K, Kita J, Katoh M, Iwasaki Y. Is a patient with metastatic pancreatic tumor from rectal cancer a candidate for resection? Hepatogastroenterology 2007; 54:1262-5. [PMID 17629084]
- Bachmann J, Michalski CW, Bergmann F, B?chler MW, Kleeff J, Friess H. Metastasis of rectal adenocarcinoma to the pancreas. Two case reports and a review of the literature. JOP. J Pancreas (Online) 2007; 8:214-22. [PMID 17356246]
- Torres-Villalobos G, Podgaetz E, Anthon FJ, Remes-Troche JM, Robles-Diaz G, Nu?ez CC. Single pancreatic metastasis from a previously resected carcinoma of the ceacum: a case report. CurrSurg 2004; 61:328-30. [PMID 15165777]
- Crippa S, Angelini C, Mussi C, Bonardi C, Romano F, Sartori P, et al. Surgical treatment of metastatic tumors to the pancreas: a single center experience and review of the literature. World J Surg 2006; 30:1536-42. [PMID 16847716]
- Gravalos C, Garc?a-Sanchez L, Hernandez M, Holgado E, Alvarez N, Garc?a-Escobar I, et al. Surgical resection of a solitary pancreatic metastasis from colorectal cancer: a new step to a cure? Clin Colorectal Cancer 2008; 7:398-401. [PMID 19036693]
- Harrison LE, Merchant N, Cohen AM, Brennan MF. Pancreaticoduodenectomy for nonperiampullary primary tumors. Am J Surg 1997; 174:393-5. [PMID 9337160]
- Le Borgne J, Partensky C, Glemain P, Dupas B, de Kerviller B. Pancreaticoduodenectomy for metastatic ampullary and pancreatic tumors.Hepatogastroenterology 2000; 47:540-4. [PMID 10791233]






