Takahiro Osuga1, Tsuyoshi Hayashi1, Hirotoshi Ishiwatari1, Michihiro Ono1, Makoto Yoshida1, Yasutoshi Kimura2, Tadashi Hasegawa3, Yasushi Sato1, Tsutomu Sato1, Koji Miyanishi1, Rishu Takimoto1, Masayoshi Kobune1 and Junji Kato1
Departments of 1Medical Oncology and Hematology, 2Surgery, Surgical Oncology and Science, and
3Pathology, Sapporo Medical University School of Medicine. Sapporo, Japan
- *Corresponding Author:
- Tsuyoshi Hayashi
Department of Medical Oncology and Hematology; Sapporo
Medical University School of Medicine; South-1, West-16,
Chuo-ku; Sapporo, Hokkaido; 060-8543, Japan
Phone: +81-11.611.2111 (ext. 3254)
Fax: +81-11.612.7987
E-mail: thayashi69@sapmed.ac.jp
Received July 2nd, 2013 – Accepted October 16th, 2013
Keywords
Endoscopic Ultrasound-Guided Fine Needle Aspiration; Immunochemistry; Neoplasm Metastasis; Pancreas; Solitary Fibrous Tumors
INTRODUCTION
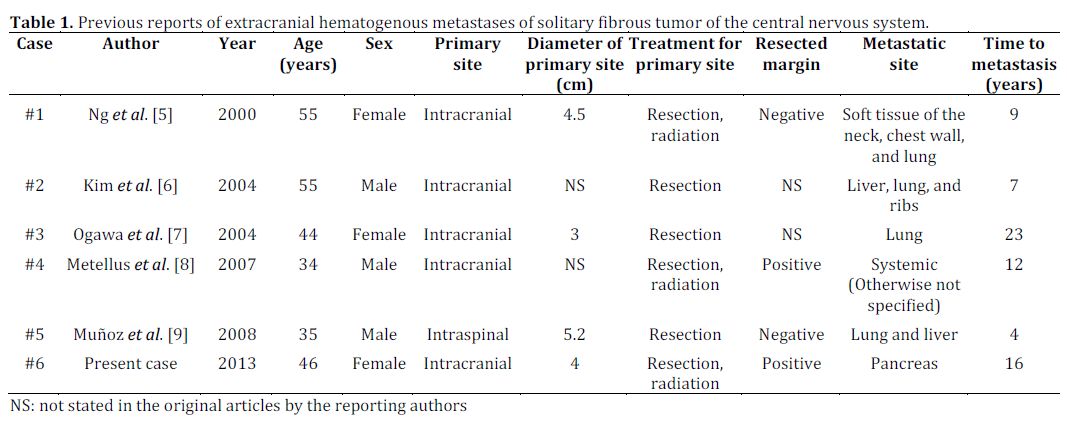
Solitary fibrous tumor of the central nervous system was firstly reported by Carneiro et al. in 1996 [1] and subsequent reports are limited, with around 200 described cases [2, 3, 4], of which only five extracranial hematogenous metastases including lung, liver, bone, soft tissue, and a combination of two or more regions have been reported thus far [5, 6, 7, 8, 9] (Table 1). We here report a case of pancreatic metastasis from solitary fibrous tumor of the central nervous system diagnosed by endoscopic ultrasound-guided fine needle aspiration (EUS-FNA).
CASE REPORT
A 62-year-old woman had chest discomfort and was examined by computed tomography (CT) with knowledge of her history of coronary heart disease. There were no findings of coronary arterial stenosis; however, a pancreatic mass with hypervascularity was incidentally detected, and she was subsequently referred to our hospital for evaluation of the mass. She had no clinical symptoms related to pancreas or hormonal hypersecretion. Her medical history included surgical resection for intracranial meningioma 16 years ago and γ-knife radiosurgery for intracranial recurrence 9 and 4 years ago. Blood examination upon admission showed normal serum levels of amylase (47 IU/L; reference range: 37-125 IU/L) and lipase (5 IU/L; reference range: 11-53 IU/L). Fasting blood sugar (206 mg/dL; reference range: 70-109 mg/dL) and glycated hemoglobin (6.6%; reference range: 4.6-6.2%) were increased, as she had previously been diagnosed with diabetes. Serum levels of tumor markers, including carcinoembryonic antigen and carbohydrate antigenic 19-9 determinant were within normal ranges. Abdominal contrast enhanced CT revealed a mass, 3.3 cm in diameter, with main pancreatic duct stenosis at the junction of the head and body of the pancreas (Figure 1a). Magnetic resonance imaging and cholangiopancreatography clearly showed cystic degeneration in the central portion of the mass and pancreatic duct stenosis due to the mass (Figure 1bcd). At that time, the lesion was suspected as non-functioning neuroendocrine tumor (NET) of the pancreas with indication of possible malignancy; therefore, pancreaticoduodenectomy with lymph node dissection was scheduled. For definitive diagnosis, the patient underwent EUSFNA using a 22-gauge ExpectTM needle (Boston Scientific Japan, Tokyo, Japan) (Figure 1ef). However, pathological examination of the EUS-FNA specimen showed an unexpected finding: there were a large number of elongated cells with collagenous fibers that were positive for CD34, CD99, and bcl-2, but negative for chromogranin A, synaptophysin, and epithelial membrane antigen (EMA) by immunohistochemical staining (Figure 2a-g). On the basis of her medical history, we conducted a pathological review of the brain specimen obtained by the first operation and found that it showed the same histological findings and immunohistochemical profile as our current EUSFNA specimen (Figure 2a’-d’). Consequently, the final diagnosis of the brain specimen was changed from meningioma to solitary fibrous tumor of the central nervous system, and the pancreatic mass was diagnosed as metastasis from solitary fibrous tumor of the central nervous system. A previous report suggested that gross resection is the most important key to a good prognosis [2]. There was no evidence of further metastasis to other organs in this case, so the patient underwent middle pancreatectomy as a limited surgery. The cut surface of the resected specimen demonstrated a noncapsulated solid mass, 3.4×3.1×2.8 cm in size, with a clear border (Figure 3). The resected pancreatic specimen was negative for surgical margin, vessel invasion, and lymph node metastasis. Further, it also had the same histological findings and immunohistochemical profile as the brain specimen (Figure 2a’’-d’’), thus, finally diagnosed as pancreatic metastasis of solitary fibrous tumor of the central nervous system.
Figure 1. Findings of image examinations. Curved planar reformation of computed tomography made by tracing the main pancreatic duct
showed a well-defined mass of the pancreas with strong enhancement, stenosis of the main pancreatic duct, and central cystic change (a.).
Magnetic resonance imaging showed an iso-intensity mass with a central cystic portion and capsule like rim on (b., c.). MR
cholangiopancreatography clearly showed cystic degeneration in the central portion of the mass and pancreatic duct stenosis due to the
mass (d.). Endoscopic ultrasound demonstrated a well-demarcated hypoechoic mass with a central hyperechoic area, which indicated
intratumoral hemorrhage or degeneration (e.). Fine needle aspiration was performed using a 22-gauge needle (f.).
Figure 2. Histological findings and immunohistochemical profiles (400×). H&E staining of the EUS-FNA specimen showed presence of
elongated cells containing oval or spindle shaped nuclei in a “patternless pattern” in EUS-FNA, surgically resected brain, and pancreatic
specimen (a, a’, a’’). The atypical feature of high mitotic rate (>4 mitoses/10 HPF) was found only in the resected pancreatic specimen (high
magnification images of the boxed area from a’’). Immunohistochemical profile of the EUS-FNA specimen demonstrated CD34, CD99, and
bcl-2 positivity (b, c, d), but chromogranin A, synaptophysin, and EMA negativity (e, f, g,), which were identical in the surgically resected
brain and pancreatic specimen (b’, c’, d’, b’’, c’’, d’’).
Figure 3. Photograph of the cut surface of the middle
pancreatectomy specimen demonstrating a well-defined
noncapsulated solid mass, 3.4×3.1×2.8 cm in size, with a central
hemorrhage.
Solitary fibrous tumor is a rare spindle neoplasm arising from pleura as first reported by Klemperer and Rabin in 1931 [10]. However, in the 1990s they were also found in various sites besides pleura, such as subcutaneous soft tissue, retroperitoneum, orbit, salivary gland, pharynx, thyroid gland, mammary gland, kidney, liver, pancreas, bladder, prostate, and adrenal gland. Although the histogenesis of solitary fibrous tumor is still controversial, it is assumed that solitary fibrous tumor is a mesenchymal neoplasm of probable fibroblastic origin [11].
As in the present case, some cases may have been misdiagnosed as intracranial meningioma because the features of solitary fibrous tumor of the central nervous system were not established until the seminal report by Carnerio et al. which was published in 1996 [1]. Nowadays, this problem can be resolved by immunohistochemistry. Solitary fibrous tumor of the central nervous system is strongly positive for CD34, CD99, and bcl-2, but not epithelial membrane antigen (EMA), whereas meningioma demonstrates positivity for EMA, but not CD34 [12, 13, 14].
In general, biological behavior of solitary fibrous tumor of the central nervous system is indolent, with 33 recurrent cases, including 28 intracranial recurrences and 5 extracranial hematogenous metastases, of 220 cases in total documented in a survey conducted between August 1996 and July 2011 as reported by Bisceglia et al. [2]. Further, they concluded that the best predictors of an unfavorable outcome are incomplete surgical resection, brain infiltration, and atypical histological features, defined as the presence of nuclear atypia and/or cellular pleomorphism, hypercellularity, high mitotic rate (>4 mitoses/10 HPF), and necrosis. In order to better understand the background of the metastasis to the pancreas in the present case, we additionally reviewed the pathological findings of the brain and pancreatic specimens obtained by surgery. Atypical histological features and brain infiltration of the brain specimen were not seen, but its margin was evidently positive; therefore, first brain surgery was interpreted as an incomplete resection which may have been the main cause of the two intracranial recurrences and the pancreatic metastasis. Further, investigation of the pancreatic specimens revealed an atypical histological feature, that of high mitotic rate (>4 mitoses/10 HPF) (Figure 2a’’), which indicated that this patient should be carefully observed due to high risk of recurrence.
The pancreatic mass of present case showed a welldemarcated round shape with hypervascularity, considered as representative findings of NET of the pancreas, by contrast enhanced CT, which has high specificity, with a mean of 96% (range 83-100%) for diagnosis of NET [15]. However, these features may also indicate several other diseases such as metastatic pancreas tumor from renal cell carcinoma [16], pancreatic solitary fibrous tumor [17, 18], pancreatic schwannoma [19], and intrapancreatic accessory spleen [20]. It is difficult to distinguish these diseases from NET by imaging examination alone. However, these issues can be resolved by EUS-FNA in some diseases, such as intra-pancreatic accessory spleen [20] and metastatic tumor of pancreas. Cause of which were confirmed by histology and/or immunohistochemistry [21].
Meanwhile, NETs with larger size (>2cm in diameter) and main pancreatic stenosis indicate malignancy, thus necessitating typical pancreatic resection such as pancreaticoduodenectomy or distal pancreatectomy with lymph node dissection [22]. However, in our case the diagnosis obtained using image examination was overturned from NET of the pancreas to pancreatic metastasis of solitary fibrous tumor of the central nervous system by EUSFNA. The manner of metastasis was hematogenous spread, so the patient underwent limited surgery instead. Selection of an adequate method of surgical resection is very important for patients with suspected low-grade malignancy or borderline malignancy, except for pancreatic ductal carcinoma, because pancreaticoduodenectomy is too invasive for such patients. Lately, limited surgery such as enucleation [23], middle pancreatectomy [24], and duodenum-preserving pancreas head resection [25] has been widely performed. Its advantages are preservation of duodenal function and both endocrine and exocrine functions of the pancreas.
CONCLUSION
We showed here the case of pancreatic metastasis from solitary fibrous tumor of the central nervous system. Even in such rare pancreatic masses, histological findings and immunohistochemical profile obtained by EUS-FNA are invaluable for the correct diagnosis to avoid excessive surgical procedures.
Financial support
The authors did not receive financial support for this article
Conflict of interests
The authors declare no conflict of interest
Note
The patient has provided permission to publish these features of her case, and the identity of the patient has been protected
References
- Carneiro SS, Scheithauer BW, Nascimento AG, et al. Solitary fibrous tumor of the meninges: a lesion distinct from fibrous meningioma. A clinicopathologic and immunohistochemical study. Am J Clin Pathol.1996; 106: 217-224.
- Bisceglia M, Galliani C, Giannatempo G et al. Solitary fibrous tumor of the central nervous system: a 15-year literature survey of 220 cases (August 1996-July 2011). Adv Anat Pathol. 2011; 18: 356-392.
- Bisceglia M, Dimitri L, Giannatempo G et al. Solitary fibrous tumor of the central nervous system: report of an additional 5 cases with comprehensive literature review. Int J Surg Pathol. 2011; 19: 476-486.
- Chen H, Zeng XW, Wu JS et al. Solitary fibrous tumor of the central nervous system: a clinicopathologic study of 24 cases. Acta Neurochir. 2012; 154: 237-248.
- Ng HK, Choi PC, Wong CW, et al. Metastatic solitary fibrous tumor of the meninges. Case report. J Neurosurg. 2000; 93: 490-3.
- Kim KA, Gonzalez I, McComb JG, et al. Unusual presentations of cerebral solitary fibrous tumors: report of four cases. Neurosurgery. 2004; 54: 1004-1009.
- Ogawa K, Tada T, Takahashi S, et al. Malignant solitary fibrous tumor of the meninges. Virchows Arch. 2004; 444: 459-464.
- Metellus P, Bouvier C, Guyotat J, et al. Solitary fibrous tumors of the central nervous system: clinicopathological and therapeutic consideration of 18 cases. Neurosurgery. 2007; 60: 715-722.
- Muñoz E, Prat A, Adamo B, et al. A rare case of malignant solitary fibrous tumor of the spinal cord. Spine. 2008; 33: E397-9.
- Klemperer P, Rabin CB. Primary neoplasms of the pleura; a report of five cases. Arch Pathol. 1931; 11: 385-412.
- Rodriguez-Gil Y, ZGonzalez MA, Carcavilla CB et al. Lines of cell differentiation in solitary fibrous tumor: an ultrastructural and immunohistochemical study of 10 cases. Ultrastruct Pathol. 2009; 33:274-85.
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO classification of tumours of the central nervous system. Lyon: IARC; 2007.
- Ambrosini-Spaltro A, Eusebi V. Meningeal hemangio-pericytomas and hemangiopericytoma/solitary fibrous tumors of extracranial soft tissues: a comparison. Virchows Arch. 2010; 456: 343-354.
- Cummings TJ, Burchette JL, McLendon RE. CD34 and dural fibroblasts: the relationship to solitary fibrous tumor and meningioma. Acta Neuropathol. 2001; 102: 349-354.
- Sundin A, Vullierme MP, Kaltsas G, et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: radiological examinations. Neuroendocrinology. 2009; 90: 167-83.
- Crippa S, Angelini C, Mussi C, et al. Surgical treatment of metastatic tumors to the pancreas: a single center experience and review of the literature. World J Surg. 2006; 30: 1536–1542.
- Srinivasan V, Wayne J, Rao M, et al. Solitary fibrous tumor of the pancreas: case report with cytologic and surgical pathology correlation and review of the literature. J Pancreas. 2008; 9: 526–30.
- Ishiwatari H, Hayashi T, Yoshida M, et al. A case of solitary fibrous tumor of the pancreas. Nippon Shokakibyo Gakkai Zasshi. 2009; 106: 1078-1085.
- Suzuki S, Kaji S, Koike N, et al. Pancreatic schwannoma: a case report and literature review with special reference to imaging features. JOP. 2010; 8: 31-35.
- Somashekar GK, Muhannad MH, Shree GS, et al. Intrapancreatic Accessory Spleen: Investigative Dilemmas and Role of EUS-Guided FNA for Diagnostic Confirmation. JOP. 2011; 12: 603-606.
- Gilbert CM, Monaco SE, Cooper ST, et al. Endoscopic ultrasound fine-needle aspiration of metastases to the pancreas: A study of 25 cases. Cytojournal. 2011; 8: 7.
- Falconi M, Bartsch DK, Eriksson B, Klöppel G, et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: well-differentiated pancreatic non-functioning tumors. Neuroendocrinology. 2012; 95: 120-134.
- Cauley CE, Pitt HA, Ziegler KM, et al. Pancreatic enucleation: improved outcomes compared to resection. J Gastrointest Surg. 2012; 16: 1347-53.
- Hirono S, Yamaue H. Middle pancreatectomy for pancreatic neoplasms. J Hepatobiliary Pancreat Sci. 2010;17: 803-807.
- Keck T, Adam U, Makowiec F, et al. Short- and long-term results of duodenum preservation versus resection for the management of chronic pancreatitis: a prospective, randomized study. Surgery. 2012; 152: S95-S102.




