Keywords
Pancreas; Pancreatic Cyst; Review
Abbreviations
ELISA enzyme linked immunosorbent assay
INTRODUCTION
Pancreatic cysts are heterogeneous groups of diseases
with a wide spectrum of pathologies which can be divided
as non-neoplastic post-inflammatory cysts and benign
and malignant neoplastic cystic tumors [1]. There are also
other classifications which divide the pancreatic cysts
according to the presence or absence of epithelial lining.
They are divided in to true cysts (with epithelial lining)
and pseudocysts (without the epithelium) [2].
The vast majority of pancreatic cysts are pseudocysts
with no epithelial lining. One of the most important cysts
in this category is infection-related pseudocysts, which are
mainly composed of parasitic cysts such as hydatid cysts
[3]. There are sporadically reported cases of hydatid cyst
in the pancreas. Hydatid cyst (caused by the larval stage
of Echinococcus granulosus) should be investigated in all
pancreatic cysts, especially in the geographical regions
where the disease is endemic (Middle East and other parts
of world including India, New Zealand, Australia, Turkey
and South Europe), which uncommon organs can be
involved by the cysts of Echinococcus granulosus [4]. The
most common organ which is involved in hydatid disease is liver (65-70% of the cases) followed by the lungs (25%).
Pancreatic location of hydatid disease is extremely rare
with a reported incidence of less than 1% [5].
In our experience in one of the largest referral centers
in the South of Iran, unusual sites of this disease such as
breast, adrenal, appendix have been reported [5, 6, 7]
which can mimic other more common diseases and causes
increased risk of diagnostic delay and potentially serious
complications [8].
The aim of this study is to review the English literature
in the past 20 years concerning the rare occurrence of
pancreatic hydatid cyst and its clinicopathologic findings.
Essential findings such as demographic findings, presenting
symptoms, method of primary diagnosis, laboratory
findings, operative findings, treatment modalities, and
follow-up studies will be separately included in all of the
cases.
To the best of our knowledge, during the last 20 years,
there have been less than 130 reported cases of pancreatic
hydatid cysts in the English literature so far.
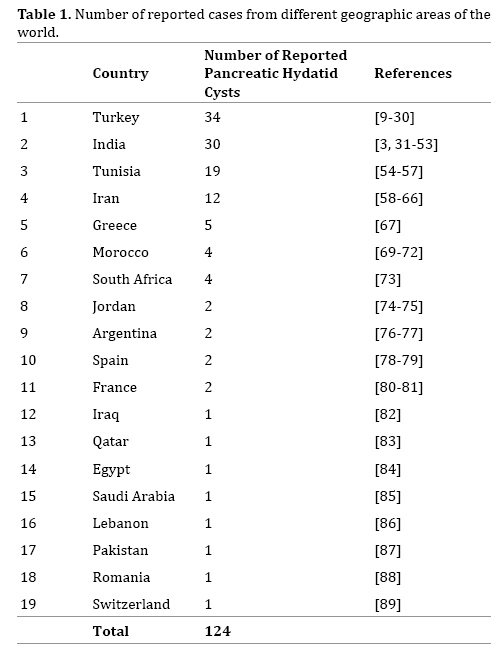
GEOGRAPHIC DISTRIBUTION
Table 1 shows the number of cases from different
parts of the world. Most common geographic locations are
in Asia (India) and mediterranean sheep-raising countries
such as Turkey and Iran [4, 9]. This disease in the pancreas
has also been reported from South Africa and African
countries such as Tunisia and Egypt [9, 10, 11, 12, 13]. In
Europe most of the reported cases have been from Spain,
Romanian and Greece [14, 15, 16], however it seems that
pancreatic hydatid cyst should be expected to occur in every country in the world and even reports have been
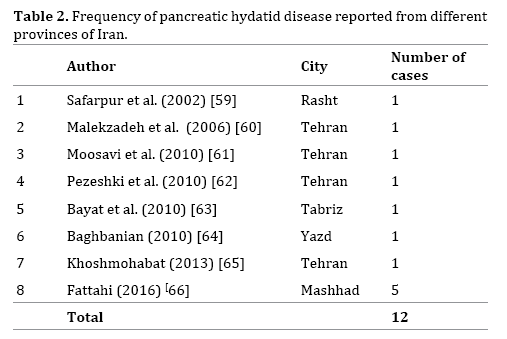
published form France and Switzerland [17, 18]. Table 2 shows pancreatic hydatid cysts reported in the literature
from different geographic areas of Iran.
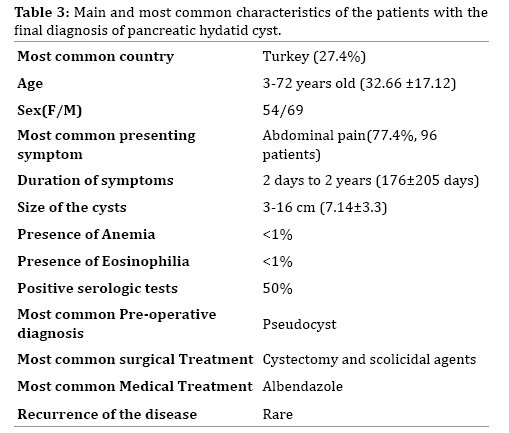
DEMOGRAPHIC CHARACTERISTICS
Among 124 cases of pancreatic hydatid cyst which have
been reported in the last 20 years, there were 54 female
and 70 male patients. Age range has been from 3-72 years
old (32.66±17.12). Table 3 shows a brief review of the
high lights of the clinicopathologic findings in these 124
patients.
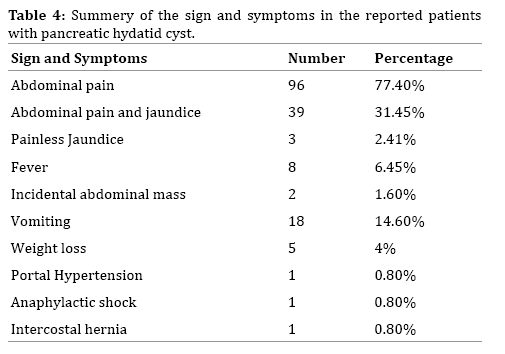
SIGNS AND SYMPTOMS
The most common presenting symptom in pancreatic
hydatid cyst is abdominal pain which has been reported in
77.4% of the cases (96 patients); some of which have been
radiating pain to back. Many of the cases have presented
with abdominal pain and jaundice which have been
reported in 39 patients (31.45%). Painless jaundice is very
rare in pancreatic hydatid cyst and has been reported in
three of the previous cases of pancreatic hydatid cyst [19, 20, 21].
Fever has not been a common finding in hydatid cyst of
pancreas, reported in 8 cases (6.45%) [11, 22, 23, 24, 25, 26, 27, 28].
Some of the previous cases have been presented with
abdominal pain, and during physical examination, an
epigastric or left upper quadrant pain have been detected.
However incidental finding of a mass in the absence of pain is very rare and have been only two cases in which
the mass was discovered incidentally with no abdominal
pain [29, 30].
There have been also a few (5 patients) reported cases
who has been presented with acute abdomen and sign and
symptoms of acute pancreatitis or acute appendicitis [13, 22, 25, 31].
Duration of the disease has been variable and the
patients have been presented with 2 days to 2 years of on
and off abdominal pain. Also there have been cases with the
history vague abdominal pain and discomfort which has
been started years before their current episode [21, 28].
Eighteen patients (14.6%) had accompanied vomiting and
rarely loss of appetite (3 cases) and weight loss (5 cases)
have also been reported [4, 9]. There have been one case
report of the presentation of pancreatic hydatid cyst as
portal hypertension [18]. Another very rare presentation
has been anaphylactic shock secondary to rupture of a
missed pancreatic hydatid cyst [14, 32].
There is another extremely rare case report of a
pancreatic hydatid cyst which has been presented as an
intercostal hernia [33]. Table 4 shows the summery of the
different sign and symptoms of the reported pancreatic
hydatid cysts.
LABORATORY FINDINGS
Complete blood count has been normal in most of
the pancreatic hydatid cysts. Anemia and leuckocytosis
have been very uncommon and has been just reported in
5 (4.06%) cases [22, 28, 33, 34, 35]. Also mild to severe
eosinophilia (2.6-25%) has only been reported in 9 cases
(7.3%) [19, 22, 32, 36, 37].
Biochemical studies have been normal in the majority
of the cases. Tumor markers have been reported as normal
(CA 19-9) and also even amylase has been rarely increased
only in 8 cases from 165-4965 IU/L (normal 17-115 IU/L)
[17, 19, 23, 26, 38, 39, 40, 41, 42]. Also lipase has been
rarely abnormal only in 4 reports from 165-757 IU/L
(normal 8-70) [17, 27, 37, 40].
Liver enzymes have been abnormal in some of the
cases with pancreatic hydatid cysts without any evidence
of liver involvement. Aspartate aminotransferase
(AST) and alanine aminotransferase (ALT) and alkaline
phosphatase (ALP) have been abnormal in 10, 8 and 14
cases respectively. AST has been 17 to 235 (normal <28
IU/L) and ALT was 55 to 336 (normal <28 IU/L). High ALP
has been reported from 488-2742 IU/L (normal <300IU/L)
[19, 20, 22, 23, 26, 35, 37, 38, 43, 44, 45, 46, 47, 48].
Serologic studies for hydatid cysts are indirect
hemagglutination assay (IHA), ELISA and Casoni tests.
Serologic tests have been performed in 50 cases, out of
which 25 cases (50%) were reactive. Most of the reports
have used ELISA and HIA and only two reports have
performed Casoni test [4, 9].
IMAGING MODALITIES
Majority of the previous cases of pancreatic
hydatid cyst have been diagnosed by modalities such
as ultrasonography (US), CT scan and rarely magnetic
resonance imaging (MRI).
Most of the reported US findings have been unilocular
thin or thick-walled hypoechoic or anechoic masses in
body, tail or head of the pancreas. According to the imaging
classification [30, 49], most of them can be categorized
as type I or II and rarely type III [50]. Calcification has
been rarely reported [12, 17, 51]. Sometimes location of the cyst cannot be accurately determined by US findings
and the patient has been operated with the preoperative
assumption of left lobe liver hydatid cyst. CT scan of the
pancreatic hydatid cysts has been mostly reported as
spherical, single, and well-delineated hypodense nonenhancing
cystic masses with no communication with the
main pancreatic duct. Location of the cyst can be accurately
determined by CT scan [27, 52]. There have been only three
cases of pancreatic hydatid cyst with connections to main
pancreatic duct of Wirsung which can be best detected
by CT scan [10, 43, 53]. Some of the cases have been
accompanied with cysts in other parts of the body such as
liver [11, 52], kidney [17, 27], breast [54]. In some cases,
presence of free floating membrane and daughter cysts
has been very helpful for the diagnosis of hydatid cyst [55].
However many of the cases have been reported without a
definite diagnosis of hydatid cyst. Radiologically, according
to US and CT scan findings the most common differential
diagnoses have been cystic neoplasms especially serous
cystadenoma and chronic pancreatitis-related pseudocyst
[6, 28, 40, 56, 57]. Some of the previous cases especially
in the pediatric age group have been operated with
the imaging diagnosis of choledochal cyst [26, 33, 58].
Preoperative diagnoses such as duplication cyst has also
been reported [26]. Exceptionally rare patients have been
operated with the imaging diagnosis of ductal carcinoma
or cystadenocarcinoma [59, 60].
There have been rare cases with MRI study (5 case
reports), with no additional information to US and CT scan.
Reported findings in MRI in pancreatic hydatid cyst have
been mostly double lining membrane [17, 36, 37, 43, 61].
Other Diagnostic Methods
Endoscopic Ultrasonography: As a pancreatic mass, EUS
has been reported in some cases with the final diagnosis
of pancreatic hydatid cyst, to know the exact origin of the
cysts and to perform FNA (fine needle aspiration). This
modality has been used in less than 5 cases of pancreatic
hydatid cyst [17, 40, 58, 62].
Magnetic Resonance Cholangiopancreaticography (MRCP),
Endoscopic Retrograde Cholangiopancreaticography (ERCP):
According to imaging studies, some of the pancreatic hydatid
cysts have been erroneously diagnosed as biliary cysts,
especially when a connection with biliary and pancreatic
ducts has been expected, so MRCP and ERCP have been
performed [17, 19, 43, 58, 63]. The most common finding
has been biliary tract dilatation in some cases because of the
pressure effects of the large pancreatic cyst [19].
Fine Needle Aspiration (FNA): One of the most available
and accurate diagnostic methods is FNA of the pancreatic
mass, however In hydatid cyst should be performed
with caution, because of the possibility of spillage and
fluid leak which can cause severe allergic reaction and
anaphylactic shock. This diagnostic method has been
performed in 12 cases [10, 25, 26, 30, 33, 43, 54, 61, 62, 64, 65, 66, 67] both before surgery and during surgery or
even rarely percutaneous [57]. The aspirated fluid has been transparent and eight (61%) FNAs showed scolices
or hooklets or both as characteristic finding [10, 26, 33, 57, 61, 66, 67]. Also in some of the cases the levels of amylase
and lipase have been tested in the punctured fluid [23, 33, 40, 54, 66]. However in most of them, these levels have
been normal and high amylase and lipase in the aspirated
fluid of pancreatic hydatid cyst has been extremely rare in
2 cases [23].
TREATMENT
Majority of the reported cases of pancreatic hydatid
cyst in the English literature have been finally operated.
The most common reported operative procedure has been
cystectomy. Majority of the cases has been planned for
laparotomy without a preoperative diagnosis of hydatid
cyst, however during surgery, inspection of the laminated
membrane has been documented and after puncture of the
fluid and injection of different types of scolicidal agents
such as cetrimide (5-3%), hypertonic sailine (20%),
H2O2, ethanol (95%) or formaldehyde, the cyst has been
unroofed and excised. In some cases omenoplasty has
been done as well [16, 38, 42, 47, 67, 68, 69]. Also in some
hydatid cysts with a connection to main pancreatic ducts
or large-sized cyst, distal pancreatectomy with or without
splenectomy have been performed [17, 28, 59, 62, 70].
In the hydatid cysts located in the head of pancreas, the
reported procedure has been pancreaticoduodenectomy
or cyst excision and Roux-en-Y [10, 20, 31, 58].
Some authors have claimed that there has not been any
risk of spillage, so they didn’t use scolicidal agents [66].
There has been other reported procedure such as
central pancreatectomy which has been used in different
pancreatic lesions as well as pancreatic hydatid cysts [70].
MEDICAL TREATMENT
In the majority of the reported cases, medical therapy
has been Albendazole (800 mg/day or 10-15 mg/Kg/day)
after surgery for 3 months, 3 courses each 21 days with
one week gap between the courses [33, 32, 38, 58].
Preoperative Albendazole has rarely been used in
some case reports to decrease the risk of recurrence when
pancreatic hydatid cyst has been diagnosed before surgery
[23, 48, 71].
FOLLOW UP AND COMPLICATIONS
In the majority of the reported cases of pancreatic
hydatid cyst, no recurrence has been happened; however
there have been cases that hydatid cyst has been missed at
the time of preliminary operation [14, 38, 60]. Recurrence,
acute pancreatitis, pancreatic fistula to other organs and
anaphylactic shock secondary to rupture and spillage of the
daughter cysts has been occurred and the patient presented
with acute abdomen, fever and chills [13, 14, 17, 34, 38, 72].
DISCUSSION
Hydatid cyst is a common cystic disease in some of the
Asian and African countries. It’s rare in North America and Europe, However in some European countries such
as Spain and Greece it’s not very uncommon. Hydatid
cyst of pancreas is an extremely rare occurrence even in
the above-mentioned endemic geographic areas and to
the best of our knowledge less than 130 cases have been
reported in the English literature so far [73, 74 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89].
This disease is more common in men and usually
presents with abdominal pain and discomfort with or
without jaundice [50, 88, 90, 91, 92, 93, 94].
Preoperative diagnosis of pancreatic hydatid cyst
is very difficult and needs high degree of suspicion.
Clinical sign and symptoms are nonspecific and usual
laboratory tests are nonspecific however antibody against
Echinococcus granulosus can be diagnostic and in the
patients with pancreatic hydatid cysts when this antibody
has been tested, more than 60% have been positive [89].
Ultrasonography has a critical role in the preoperative
diagnosis of pancreatic hydatid cyst if characteristic
finding such as water-lily sign are present. CT scan has
added little information to US finding except for more
accurate localization [53, 56]. ERCP and MRCP have been
performed in the cases with suspicion to biliary disease.
These two modalities can accurately determine the exact
location of the cyst within the pancreas [48].
FNA during EUS or percutaneous have been rarely
positive but detection of scolices and hooklets are definite
for the diagnosis of hydatid cyst [95, 96]. The goal of all the
therapeutic modalities are to decrease the complications,
recurrence, and preventing the spillage of daughter cysts
[18].
The surgical procedure can be conservative or
radical. In some uncomplicated cases with no connection
to main pancreatic duct, pericystectomy, unroofing
accompanied by using scolicidal agents with or without
omenoplasty has been performed. However in some
other cases with large size, or with the connection to main
duct, according to the location, distal pancreatectomy
with or without splenectomy, Whipple’s operation, and
pancreaticoduodenectomy have been done [7, 94].
Most of the complicated cases have been occurred
secondary to missed pancreatic hydatid cyst during
laparotomy for excision of intra-abdominal hydatid cysts
in the more usual sites such as liver [18, 22, 32].
The best medical treatment option is prescribing
Albendazole before and after surgery which needs
preoperative diagnosis of hydatid cyst [7].
CONCLUSION
Accurate preoperative diagnosis of pancreatic hydatid
cyst is very important to lower the rate of complications
and recurrence. Unfortunately in most of the previously
published cases, serologic tests have not been done,
so many of the patients have been operated with the
preliminary diagnosis of pseudocyst or neoplastic cysts and diagnosis of hydatid cyst have been made during the
surgery.
As a conclusion, hydatid cyst should be considered in
the patients with pancreatic cysts in all of the endemic
countries and determination of serologic tests in
conjunction with US findings can be very helpful for
accurate diagnosis.
Conflict of Interest
The authors declare no conflict of interest.
References
- Jabłońska B. Pancreatic cysts: etiology, diagnosis and management. Cent Eur J Med 2014; 9:92-107.
- Basturk O, Coban I, Adsay NV. Pancreatic Cysts. Pathologic Classification, Differential Diagnosis, and Clinical Implications. Arch Pathol Lab Med 2009; 133:423–438. [PMID: 19260748]
- Wani NA, Shah OJ, Zargar JI, Baba KM, Dar MA. Hydatid disease of pancreas. Dig Surg 2000; 17:188-190. [PMID: 10781989
- Geramizadeh B, Maghboul M, Ziyaian B. Primary hydatid cyst of the adrenal gland: a case report and review of the literature. Iran Red Crescent Med J 2011; 13:346–7. [PMID: 22737492]
- Bolandparvaz S, Baezzat SR, Geramizadeh B, Salahi R, Lotfi M, Paydar S. Appendiceal hydatid cyst: a case report and review of literature. Clin J Gastroenterol 2010; 3:182–5. [PMID: 26190244]
- Geramizadeh B, Makarempour A, Talei A. Primary isolated hydatid cyst of breast. Breast J 2011; 17:314–6. [PMID: 21545436]
- Geramizadeh B. Isolated Peritoneal, Mesenteric, and Omental Hydatid Cyst: clinicopathologic Narrative Review. Iran J Med Sci 2017; 42: 517–523. [PMID: 29184259]
- Geramizadeh b. Unusual Locations of the Hydatid Cyst: A Review from Iran. Iran J Med Sci 2013; 38:2-14. [23645952]
- Elsorogy M, El-Hemaly M, Aboelenen A. Pancreatic hydatid cyst. A case report. Int J Surg Case Report 2015; 6:68-70. [PMID: 25528027]
- Abid M, Guirat A, Amar MB. Hepatobiliary and Pancreatic: Isolated hydatid cyst of the pancreas. J Gastroenterol Hepatol 2008; 23:1773. [PMID: 19120866]
- Derbel F, Zidi MK, Mtimet A, Hamida MBH, Mazhoud J, Youssef, et al. Hydatid cyst of the pancreas: A report on seven cases. Arab J Gastroenterol 2010; 11:222.
- Makni A, Chebbi F, Jouini M, Kacem M, Safta ZB. Left pancreatectomy for primary hydatid cyst of the body of pancreas. Ann African Surg 2011;8:52-55.
- Mabrouk MB, Waad F, Malek B, Jafar M, Fatiha H, Ahlem S, et al. Hydatid cyst of the pancreas: A report of 10 cases. JOP 2015:591-6.
- Safioleas MC, Moulakakis KG, Manti C, Kostakis A. Clinical consideration of primary hydatid disease of the pancreas. Pancreatology 2005; 5:45461. [PMID: 15985772]
- Azouara MV, Dorado JJ, Garcia-Diaz M, Zapata J, Plasencia A, Tellez F. Obstructive jaundice associated with a hydatid cyst of the pancreas. Pancreas 1997; 14:309-321. [PMID: 9094164]
- Echenique-Elizondo M, Arratibel JAA. Hydatid disease of the pancreas. JOP 2004; 5:51-4. [PMID: 14730124]
- Diop SP, Costi R, Le Bion A, Carloni A, Meduri B, Smadja C. Acute pancreatitis associated with a pancreatic hydatid cyst: understanding the mechanism by EUS. Gastrointest Endosc 2010; 72:1312-14. [PMID: 20630507]
- Szanto P, Goian I, Al Hajjar N, Badea R, Seicean A, Manciula D, ET AL. Hydatid cyst of the pancreas causing portal hypertension. Maedica (Buchar) 2010; 5:139-141. [PMID: 21977139]
- Yattoo GN, Khuroo MS, Zargar SA, Bhat FA, Sofi BA. Percutaneous drainage of the pancreatic cyst. Case Report: Percutaneous drainage of pancreatic head cyst with obstructive jaundice. J Gastroenterol and hepatol 1999; 14: 931-934. [PMID: 10535478]
- Krige JEJ, Mirza K, Bornman PC. Primary hydatid cysts of the pancreas. SAJD 2005; 43:37-40.
- Diego T, Gonzalo C, Carlos ST, Gaston M, Fabian C, Paul EL, et al. Primary hydatid of the pancreas. Rev Fac Cien Med Univ Nac Cordoba 2017; 74:33-36. [PMID: 28379129]
- Ozmen MW, Moran M, Karakahya M, Coskun F. Recurrent acute pancreatitis due to a hydatid cyst of pancreatic head: A case report and review of the literature. JOP 2005; 6; 354-8. [PMID: 16006687]
- Karakas E, Tuna Y, Basar O, Koklu S. Primary pancreatic hydatid disease associated with acute pancreatitis. Hepatobiliary Pancreat Dis Int 2010; 9:441. [PMID: 20688612]
- Sinha AN, Rao ASN, Vyas HG. Hydatic cyst in head of pancreas presenting with obstructive jaundice. Indian J Gastroenterol 1997; 16:32. [PMID: 9167380]
- Dalal U, Dalal AK, Singal R, Naredi B, Gupta S. Primary hydatid cyst masquerading as pseudocyst of the pancreas with concomitant small gut obstruction-an unusual presentation. Kaohsiung J Med Sciences 2011; 27:32-35. [PMID: 21329890]
- Mondelia A, Wahal A, Solanki S, Srinivas M, Bhatnagar V. Pancreatic hydatid cyst maduederating as a choledochal cyst. J Ped Surg 2012; 47:E41-E44. [PMID: 23164030]
- Baghbanian M, Salmanroghani H, Karegar S, Binesh F, Baghbanian A. Pancreatic tail hydatid cyst as a rare cause for severe acute pancreatitis. A case report. Govaresh 2013; 18:194-8.
- Regan JK, Brown RD, Marrero JA, Malik P, Rosenberg F, Venu RP. Chronic pancreatitis resulting from primary hydatid disease of the pancreas: a case report and review of the literature. Gastrointest Endosc 1999; 49:791-3. [PMID: 10343231]
- Borisa AD, Bakhshia GD, Tayade MB, Pawar NH, Nikam NN, Pathrikar S. Hyadtid cyst of pancreas . Bombay Hospital J 2009; 51: 88-90.
- Hiremat B, Subramaniam N, Boggavarapu M. Primary pancreatic hydatid cyst: an unexpected differential diagnosis. BMJ Case Reports 2015. [PMID: 26336187]
- Trigui A, Rejab H, Guirat A, Mizouni A, Amar MB, Mzali R, et al. Hydatid cyst of the pancreas (about 12 cases). Ann Ital Chir 2013; 84: 165-170. [PMID: 23697975]
- Birlutiu V, Birlutiu RM. The management of abdominal hydatidosis after the rupture of a pancreatic hydatid cyst: a case report. J Med Case Rep 2015; 9:77. [PMID: 25890012]
- Erdener A, Sahin AH, Ozcan C. Primary pancreatic hydatid disease in a child: case report and review of the literature. J Ped Surg 1999; 34:491-2. [PMID: 10211664]
- Cankorkmaz L, Gumuo C, Celiksoz A, Koyluoglu G. Primary hydatid disease of pancreas mimicking pancreatic pseudocyst in a child: case report and review of the literature. Turkiye Parazitol Derg 2011; 35: 50-2. [PMID: 21618194]
- Turkyilmaz Z, kapisiz A, Sonmez K, Karabulut R, Basaklar AC. Obstructive jaundice resulted from hydatid cyst of pancreatic head. Hippokratia 2013; 17:378-79. [PMID: 25031523]
- Shah OJ, Robbani I, Zargar SA, Yattoo GN, Shah P, Ali S, et al. Hydatid cyst of the pancreas. An experience with six cases. JOP 2010; 11:575-581. [PMID: 21068489]
- Bakkaly AE, Merouane N, Dalero O, Oubeja H, Erraji M, Ettayebi F, et al. Primary hydatid cyst of the pancreas. Pan Afr Med J 2017; 28:229.
- Suryawanshi P, Khan AQ, Jatal S. Primary hydatid cyst of pancreas with acute pancreas. Int J Surg Case Reports 2011; 2:122-4. [PMID: 22096702]
- Patil DS, Jadhar KV, Ahire PP, Patil SR, Shaikh TA, Bakhshi GD. Pancreatic hydatid presenting as an intercostal hernia. Int J Med Appl Sci 2013; 2:255-258.
- Ahmed Z, Chhabra S, Massey A, Vij V, Yadar R, Bugalia R, et al. Primary hydatid cyst of the pancreas: Case report and review of literature. Int J Surg Case Rep 2016; 27:74-77. [PMID: 27552034]
- Pezeshki A, Kia EB, Gholizadeh A, Koohzare A. An analysis of hydatid cyst surgeries in Tehran, Milad Hospital, Iran, during 2001-4. Pak J Med Sci 2007; 23:138-140.
- Fattahi AS, Maddah G, Yousefi Y. Primary hydatid disease of pancreas. JOP 2016; 17:494-497.
- Agrawal S, parag P. Hydatid cyst of head of pancreas mimicking choledochal cyst. BMJ Case Reports 2011. [PMID: 22693192]
- Yarlagadda P, Yenigalla BM, Penmethsa U, Myneni RB. Primary pancreatic echinococcosis. Trop Parasitol 2013; 3:151-4. [PMID: 24471002]
- Bhat NA, Rashid KA, Wani I, Wani S, Syeed A. Hydatid cyst of the pancreas mimicking choledochal cyst. Ann Saudi Med 2011; 31:536-8. [PMID: 21911995]
- Ousadden A, Elbouhaddouti H, Ibnmajdoub K, Mzaz K, Aitaleb K. Primary hydatid cyst of pancreas with a hepatic pedicle compression. Cases Journal 2009; 2:201. [PMID: 20062706]
- Boubbou M, Boujraf S, Sqalli NH, Maaroufi M, Tizniti S. Large pancreatic hydatid cyst presenting with obstructive jaundice. Arab J Gastroenterol 2010; 11:47-49.
- Lenz A, Brunner A, Metzger J. A painless mass in the pancreas, incidental finding. Jama Surgery 2015; 150:1189-90. [PMID: 26509326]
- Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics 2003; 23:475-494. [PMID: 12640161]
- Glossis KJ, Kontoyiannis DS, Dascalogiannaki M, Gourtsoyiannis NC. Uncommon locations of hydatid disease: CT appearances. Eur Radiol 1997; 7:1303-1308. [PMID: 9377519]
- Chatterjee S, Roy MK, Banerjee S, Mukhopadhaya S, Sen S, Mallahath MK. Hydatid cyst mimicking x=cystic neoplasm of the pancreatic tail: an endoscopic ultrasound diagnosis. Endoscopy 2014; 46:E318-E319. [PMID: 25058831]
- Chinya A, Khanolkar A, Kumar j, Sinha SK. Isolated hydatid cyst of the pancreas masquerading as pancreatic pseudocyst. BMH Case Report 2015. [PMID: 26264949]
- Aksakal N, Kement M, Okkabaz N, Altunatas YE, Oncel M. Unusually located primary hydatid cyst. Ulus Cerrahi Derg 2016; 32:130-133. [PMID: 27436938]
- Erkan N, Haciyanli M, Yildirim M, Yilmaz C. A case report of unusual presence of hydatid disease in the presence of hydatid disease in the pancreas and breast. JOP 2004; 5: 368-372. [PMID: 15365205]
- Koylooglu G, Oztoprak I. Unusual Localizations of Hydatid Disease. Pancreas 2002; 24: 410-11. [PMID: 11961495]
- Arikan A, Sayan A, Erikçi VS. Hydatid cyst of the pancreas: a case report with 5 years' follow-up. Pediatr Surg Int 1999; 15: 579-581. [PMID: 10631740]
- Karaman B, Battal B, Ustunsoz B, Ugurel MS. Percutaneous treatment of a primary pancreatic hydatid cyst using a catheterization technique. Korean J Radiol 2012; 13:232-6. [PMID: 22438691]
- Somani k, Desai AA. An unusual case of pancreatic hydatid cyst mimicking choledochal cyst. Bombay hospital J 2011; 53:103-5.
- Khoshmohabat h, Moqadam JH, Sohrabi SZ, Motamedi MHK, Azizi T. Hydatid cyst of the pancreas mimicking neoplasm. J Coll Physicians Surg Pak 2014; 24(Suppl 2): S84-85. [PMID: 24906281]
- Astiz JM, Astiz L, Buzzi A. Primary hydatid cyst mistaken for carcinoma of the pancreas. J Royal Society of Med 1997; 90:334. [PMID: 9227383]
- Jai SR, El Hattabi K, Bensardi F, Chehab F, Khaiz D, Bouzidi A. Primary hydatid cyst of pancreas causing obstructive jaundice. The Saudi J Gastroenterol 2007; 13:191-3. [PMID: 19858645]
- Coudhary NS, Kumar N, Puri R. An unusual cause of pancreatic space-occupying lesion. Gastroenterol 2014; 146:e12-e13. [PMID: 24468166]
- Khanna AK, Prasanna GV, Khanna R, Kunna A. Unusual sites of hydatid cysts in India. Trop Doct 2005; 35:233-5. [PMID: 16354481]
- Yorganci K, Iret D, Sayek I. A case of primary hydatid disease of the pancreas simulating cystic neoplasm. Pancreas 2000; 21:104-5. [PMID: 10881942]
- Yildirim M, Erkan N, Vardar E. Hydatid cysts with unusual localization. Diagnostic and treatment dilemmas for surgeons. Ann Trop Med Parasitol 2006; 100:137-42. [PMID: 16492361]
- Varshney M, Shahid M, Maheshuari V, Siddiqui MA, Alam K, Mubeen A, et al. Hydatid cyst in tail of pancreas. BMJ Case Reports 2011. [PMID: 22673711]
- Kaushik K, Garg P, Aggrawal S, Narang A, Verma S, Singh J, et al. Isolated pancreatic tail hydatid cyst. Is distal pancreatectomy always necessary. The Internet J Gastroenterol 2013; 13:1-3.
- Singh R, Khullar A. Pancreatic hydatic cyst. Indian J Gastroenterol 1999; 18:35. [PMID: 10063748]
- Heis HA, Bani-hani KE, Elheis MA. Primary hydatid cyst of the pancreas. Acta Chirurgia Belgica 2009; 109:626-628. [PMID: 19994808]
- Adham M, Guinippero A, Hervierru V, Courbiere M, Partensky C. Central pancreatectomy(Single center experience of 50 cases). Arch Surg 2008; 143:175-180. [PMID: 18283143]
- Malekzadeh R, Pezeshki B, Mormazdi M, Rakhshani N, Soroush Z. Primary hydatid cyst of the pancreas(Photoclinic). Arch Iran Med 2006; 9:291-2. [PMID: 16859072]
- Elaffand A, Vijay A, Mohamed S, Al Battah HH, Yousef A, Farahet A. Echinococcal cyst of the pancreas with cytopancreatic duct fistula successfully treated by partial cystectomy and cystogastrectomy. J Surg Tech Case 2015; 7:48-50. [PMID: 27512554]
- Col C, Col M, Lofci H. Unusual localization of hydatid disease. Acta Medica Austriaca 2003; 30:61-64. [PMID: 12752092]
- Hamamci E, Basim H, Korkmaz A, Unusual locations of hydatid disease and surgical approach. ANZ J Surg 2004; 74:356-60. [PMID: 15144257]
- Zeybek N, Tas H, Kaymakcioglu N, Azcan A, Cetiner S, Tufan T. Hydatid cyst in the head of the pancreas in an adult. Case report. Med J Kocatepe 2006; 7:9-12.
- Ibis C, Albayrak D, Altan Y. Primary hydatid disease of pancreas mimicking cystic neoplasm. Southern Med J 2009; 102:529-30. [PMID: 19373169]
- Orug T, Okdogan m, Atalay F, Sakaogullari Z. Primary hydatid disease of pancreas mimicking cystic pancreatic neoplasm: Report of two cases. Turkiye Klinikleri Med Sci 2010; 30:2057-60.
- Caglayan K, Celik A, Koc A, Kutlul AC, Altinli E, Celik AS, et al. Unusual location of hydatid disease: Diagnostic and surgical management of a case series. Surg Infections 2010; 11:350-3.
- Kisaoglu A, Ozogul B, Atamanalp SS, Pirimoglu B, Aydinli B, Kokut E. Incidental isolated pancreatic hydatid cyst. Turkiye Parazitol 2015; 49:75-7. [PMID: 25917590]
- Canbak T, Acar A, Kivanc AE, Basak F, Kulali L, Bas G. Sinistral portal hypertension due to pancreatic hydatid cyst. Turkiye Parazitol Derg 2017; 41:226-8. [PMID: 29318995]
- Rayate A, Prabhu R, Kantharia C, Supe A. Isolated pancreatic hydatid cyst. Preoperative prediction on contrast-enhanced computed tomography case report and review of literature. Med J Dr D Y Patil University 2012; 5:66-8.
- Mushtaque M, Mir MF, Malik AA, Arif SH, Khanday SA, Dur RA. Atypical localization of hydatid disease: experience from a single institution. Nigerian J Surg 2012; 18:2-7. [PMID: 24027383]
- Mohamadnejad M, Eloubeidi MD. Cystic lesions of the pancreas. Arch Iran Med 2013; 16: 233-39. [PMID: 23496368]
- Safarpour F. Pancreatic hydatid cyst surgery with internal drainage. Med J Iran Hosp 2002; 5:43-44.
- Moosavi SR, Kermany HK. Epigastric mass due to a hydatid cyst of the pancreas. A case report and review of literature. JOP 2007; 8:232-4. [PMID: 17356249]
- Bayat AM, Azhough R, Hashemzadeh S, Barband A, Yaghoubi AR, Gargari RM. Hydatid cyst of pancreas presented as a pancreatic pseudocyst. Am J Gastroenterol 2009; 104:1325-7. [PMID: 19319123]
- Yuksel M, Demirpalat G, Sever A, Bakaris S, Bulbuloglu E, Elmas N. Hydatid disease involving some rare locations in the body: a pictorial essay. Korean J Radiol 2007; 8:531-40. [PMID: 18071284]
- Jonkov A, Todorov R, Katibova S.Clinical case of echinococcus of the pancreas. Khirurgiia (Sofiia) 2014; 3:46-50. [PMID: 25799623]
- Massodi I, Nabi G, Kumar R, Lone MA, Khan BA, Al Sayani KN. Hydatid cyst of the pancreas. A case report and brief review. Turk J Gastroenterol 2011; 22:430-432. [PMID: 21948577]
- Faraj W, Selmo F, Khalefeh M, Jamali F. Laparoscopic resection of pancreatic hydatid disease. Surgery 2006; 139:438-441. [PMID: 16546510]
- Zaidi SH. Some rare presentation of hydatid cysts. Two case reports. Cases J 2009; 2:62. [PMID: 19149905]
- Inan N, Arslan A, Akansel G, Arik Y, Demirci A. Diffusion-Weighted imaging in the differential diagnosis of cystic lesions of the pancreas. AJR 2008; 191:1115-1121. [PMID: 18806153]
- Sayek I, Tirnaksiz MB, Dogan R. Cystic hydatid disease. Current trends in diagnosis and management. Surg Today 2004; 34:987-996. [PMID: 15580379]
- Dziri C, Dougaz W, Bouasker I. Surgery of pancreatic cystic echinoccosis:Systematic review. Transl Gastroenterol 2017; 2:105. [PMID: 29354762]
- Sharma S, Sarir H, Guleria M, Agrawal K. Endoscopic ultrasounded-guide fine needle aspiration: Emerging technique to diagnosis hydatid cyst of pancreas. J Cytol 2015; 32:211-12. [PMID: 26729989]
- Geramizadeh B, Boob R, Talei AR, Rasekhi A. Fine needle aspiration cytology in hydatid cyst of breast. Acta Cytol 2003; 47:710-2. [PMID: 12920772]

