Keywords
Diabetes Mellitus; Genes, Suppressor, Tumor; Oncogenes; Pancreatic Neoplasms; Diagnosis; Tumor Markers, Biological
Abbreviations
CDK4: cyclin-dependent kinase 4; CEA: carcinoembryonic antigen; DPC4: deleted in pancreatic carcinoma-locus 4; GAP: GTPase-activating protein; POA: pancreatic oncofetal antigen; TGF: transforming growth factor
In the field of laboratory medicine, efforts are being made to provide clinicians with evidence conducive to correct clinical decision-making in patients with pancreatic diseases. In patients with pancreatic head mass, the diagnosis can only be made by deciding whether or not pancreatic cancer is present. The diagnostic work-up may start with the study of different biological samples, including sera and/or urine which are easy to collect, unlike pancreatic juice, bile or pancreatic tissue samples, which require invasive techniques, and are therefore less widely used. The serological diagnosis of pancreatic head mass depends mainly on the use of tumor markers, which must have a sensitivity and a specificity of almost 100% if they are to be clinically effective, allowing a differential diagnosis between cancer and benign diseases of the pancreas (which are mainly chronic pancreatitis). Several families of molecules have been studied as possible tumor markers, including oncofetal antigens (CEA and POA), pancreatic enzymes, blood group-related antigens and, more recently, oncogenes and tumor suppressor genes [1, 2]. Neither pancreatic enzymes nor CEA are useful in clinical practice, since they have a sensitivity and specificity of below 50%. Blood group related antigens, CA 19-9 in particular, have the highest diagnostic efficacy in distinguishing between pancreatic cancer and chronic pancreatitis. Figure 1 shows the biochemistry of the Lewis blood group-related antigens [3].
Figure 1. Blood group related antigens
The sensitivity and the specificity of CA 19-9 in diagnosing pancreatic cancer range from 70 to 95% and 72 to 90% respectively. Although most pancreatic cancers cause an increase in serum CA 19-9 levels, this tumor marker does not approach 100%. This results from two main pathophysiological aspects: 1) since individuals with Lewis a-/b- status (7-10% of the general population) cannot synthesize sialyl Lewis a antigenic determinant (Figure 1), even if they have a large tumor they will have low circulating CA 19-9 levels; 2) the release of CA 19-9 antigen in cell culture media is correlated with the number of neoplastic cells in culture, and this phenomenon is reflected “in vivo” by the association between CA 19-9 levels and the tumor stage. The clinical effect of this is that CA 19-9 has a low sensitivity in the diagnosis of circumscribed tumors and when used for screening programs. Regarding specificity, the lack of absolute results is due to several factors: 1) tumors of non-pancreatic origin may cause an increase in CA 19-9 serum levels (biliary: sensitivity 55-79%; hepatocellular and cholangiocellular: sensitivity 22-51%; gastric; colorectal; ovarian; lung; breast and uterine); 2) benign diseases of the pancreo-biliary tree (chronic pancreatitis and obstructive jaundice) may also cause significant increases in serum CA 19-9. An altered hepatic function, whether caused by cancer or a benign disease, may give rise to increased serum CA 19-9 levels, due to its reduced molecular clearance, which occurs mainly through the hepatic metabolism [4].
CA 19-9 may also be useful in monitoring pancreatic cancer since it correlates closely with the clinical course of the disease after surgery and chemotherapy and/or radiotherapy. It reaches normal levels within 2 to 4 weeks after radical surgery: there is a transient decrease after successful palliative therapy and an increase before clinical relapse [2, 5].
In this era of molecular biology, numerous oncogenes and tumor suppressor genes have been described, several of which are often altered in patients with pancreatic cancer. The genes most frequently found to be altered in patients with pancreatic adenocarcinoma are K-ras, p53, p16 and they are deleted in pancreatic carcinoma-locus 4 (DPC4) [6]. More than 90% of pancreatic tumors bear codon 12 K-ras point mutations. To our knowledge, this is the highest frequency to be reported for any tumor type. Such mutations have been observed in the early phases of pancreatic carcinogenesis, determining the synthesis of an altered p21 protein [3, 4]. Normal p21 shifts from an active (bound to GTP) to an inactive (bound to GDP) state via its intrinsic GTPase activity and via its sensitivity to the activity of GTPase activating protein (GAP). The transformed p21 becomes insensitive to GAP, thus leading this protein to a constitutive and permanent activation stimulating cell growth [7-9]. Another gene frequently altered in pancreatic cancer is p16 (homozygously deleted in about 40% of pancreatic carcinomas), an inhibitor of cyclindependent kinase 4 (CDK4) which promotes the progression of the cell division cycle through the late G1 phase to G1/S [10]. The genetic alterations involving p16 may be the methylation of the promoter region (15% of cases), homozygous deletion (40%) or deletion accompanied by intragenic mutations in the other allele (40%). The tumor suppressor gene p53, which controls the cell cycle and induces apoptosis, is altered in 50 to 70% of different types of pancreatic cancer, and is usually inactivated by the loss of one allele accompanied by a intragenic mutation of the other allele [10, 11]. The gene DPC4 is altered in about 50% of pancreatic tumors, and encodes a protein belonging to the SMAD family, which is involved in the nuclear translocation of the inhibitory signal for cell growth starting from the interaction between transforming growth factor (TGF) beta1 and its membrane receptor, TGF-beta1R [10, 12, 13].
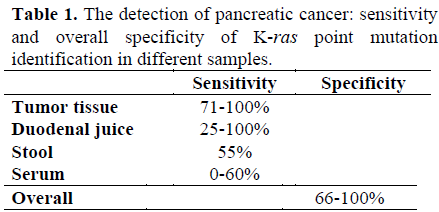
The above-mentioned genes have been studied in tissue samples and some, K-ras in particular, have also been evaluated in biological samples (not only pancreatic tissue) in order to enable the identification, in easily obtained samples, of gene alterations indicating the presence of a pancreatic tumor. K-ras point mutations have been studied in duodenal juice, in stools and in serum samples [14-21]. Overall, its sensitivity in the detection of pancreatic tumors decreases when a search is made for K-ras in samples other than from the tumor tissue (Table 1).
In laboratory medicine, serum and/or stools should be satisfactory for use as samples for diagnostic purposes, since they are easily obtained, thus favouring patient compliance. However, the sensitivity of K-ras point mutation identification is unsatisfactory in diagnosing pancreatic cancer using these samples, perhaps partly due to methodological problems (presence of Taq polymerase inhibitors in faecal samples and low amounts of mutated K-ras in a wide background of normal serum K-ras). It cannot therefore as yet be used in clinical practice, although it may be routinely used in the future, in line with improvements in molecular biology techniques.
The identification of lymph node or distant metastasis, routinely made with histology on surgical specimens, is a crucial step in staging gastrointestinal tumors, pancreatic cancer in particular. In recent years, in the attempt to improve upon the sensitivity of histology in identifying lymph-node metastasis, various techniques have been studied, including immunocytochemical analysis, with antibodies elicited towards cancer-specific antigenic determinants, and the molecular detection of cancer cells [22]. The latter approach has received particular attention, not only in the identification of lymph-node cancer cells, but also in their identification in blood and bone marrow [23-27]: as the molecular approach is highly sensitive, it is of great potential in the identification of scarce cancer cells (1 cell in a population of 107- 108). The molecular detection of cancer cells in a population of benign cells must target molecular determinants commonly expressed by tumoral, but not by non-tumoral, cells.
Among these determinants, considering tumors of epithelial origin, such as those of the gastrointestinal tract, are the mRNA encoding for CEA which are not usually expressed by normal lymph nodes, circulating and bone marrow cells [22-27]. It has been suggested that CEA mRNA detection in lymph nodes, blood and bone marrow is of prognostic value in patients with colorectal and pancreatic cancer, since it probably indicates the presence of micrometastatic foci that cannot be identified by microscopy [28].
In the diagnosis of pancreatic head tumors, diabetes mellitus has received particular attention. This metabolic alteration is, in fact, associated with pancreatic cancer in more than 80% of cases, and in some it is characterized by reduced glucose tolerance and reduced insulin secretion [29-32]. There is a body of clinical and experimental data demonstrating that pancreatic-cancerassociated diabetes mellitus is due to the cancer itself rather than pancreatic islet destruction. It has been suggested that soluble mediators released by pancreatic cancer cells play a role in interfering with the metabolism of glucose. Pancreatic-cancer-associated diabetes mellitus or glucose intolerance are improved, or cured, following surgical removal of the pancreatic mass [33]. This indicates that diabetes mellitus is not correlated with islet cell destruction, but to the presence of the tumor itself. Furthermore, in pancreatic cancer patients, the release of insulin after glucagon stimulation indicates a reduced beta cell function [34]. In agreement with this clinical data, the treatment of isolated islets of Langerhans with pancreatic cancer conditioned media dissociates insulin from amylin secretion [35]. Moreover, it has been demonstrated in clinical series that besides the presence of an altered function of Langerhans islets, there is also a peripheral insulin resistance [32, 33]. In this respect it has been demonstrated that pancreatic tumor extracts determine an altered glycogen synthesis in isolated rat muscles [36]. Furthermore, pancreatic cancer conditioned media can also induce fasting hyperglycaemia in SCID mice [37] as well as inhibiting hepatic glycolysis, thus possibly favouring the synthesis of tryglycerides [38, 39]. It has been suggested that, one of the possible pancreatic cancer-associated diabetogenic products, soluble low molecular weight peptides play a role [39, 40]. A further valuable laboratory tool in the diagnosis of pancreatic head mass might be the identification of this/these substances and their determination in serum or urine.
References
- Plebani M, Basso D, Panozzo MP, Fogar P, Del Favero G, Naccarato R. Tumor markers in the diagnosis, monitoring and therapy of pancreatic cancer: state of the art. Int J Biol Marker 1995; 10:189-99.
- Lamerz R. Role of tumor markers, cytogenetics. Ann Oncol 1999; 10(Suppl. 4):S145-9.
- Brockhausen I. Pathways of O-glycan biosynthesis in cancer cells. BiochemBiophysActa 1999; 1473:67-95.
- Basso D, Fabris C, Meggiato T, Del Favero G, Fogar P, Panozzo MP, et al. Serum levels of CA 19-9 and tissue polypeptide antigen (TPA) are related to the presence of a benign extra-hepatic cholestasis. Med Sci Res 1989; 17:13-4.
- Halm U, Schumann T, Schiefke I, Witzigmann H, Mossner J, Keim V. Decrease of CA 19-9 during chemotherapy with gemcitabine predicts survival time in patients with advanced pancreatic cancer. Br J Cancer 2000; 82:1013-6.
- Friess H, Kleef J, Kork M, Buchler MW. Molecular aspects of pancreatic cancer and future perspectives. Dig Surg 1999; 16:281- 90.
- Lemoine NR, Jain S, Hughes CM, Staddon SL, Maillet B, Hall PA, et al. Ki-ras oncogene activation in preinvasive pancreatic cancer. Gastroenterology 1992; 102:230-6. [92090629]
- Hruban RH, van Mansfeld AD, Offerhaus GJ, van Weering DH, Allison DC, Goodman SN, et al. K-ras oncogene activation in adenocarcinoma of the human pancreas. A study of 82 carcinomas using a combination of mutant-enriched polymerase chain reaction analysis and allele-specific oligonucleotide hybridization. Am J Pathol 1993; 143:545-54. [93343212]
- Schaeffer BK, Glasner S, Kuhlmann E, Myles JL, Longnecker DS. Mutated c-Ki-ras in small pancreatic adenocarcinoma. Pancreas 1994; 9:161-5.
- Kern SE. Advances from genetic clues in pancreatic cancer. Current Opinion in Oncology 1998; 10: 4-80.
- Yamaguchi Y, Watanabe H, Yrdiran S, Ohtsubo K, Motoo Y, Okai T, Sawabu N. Detection of mutations of p53 tumor suppressor gene in pancreatic juice and its application to the diagnosis of patients with pancreatic cancer: comparison with K-ras mutation. Clin Cancer Res 1999; 5:1147-53. [99280217]
- Le Dai J, Schutte M, Bansal RK, Wilentz RE, Sugar AY, Kern SE. Transforming growth factor-beta responsiveness in DPC4/SMAD4-null cancer cells. Mol Carcinogenesis 1999; 26:37-43.
- Schutte M. DPC4/SMAD4 gene alterations in human cancer, and their functional implications. Ann Oncol 1999; 10(Suppl. 4):S56-9.
- Kondo H, Sugano K, Fukayama N, Kyogoku A, Nose H, Shimada K, et al. Detection of point mutations in the K-ras oncogene at codon 12 in pure pancreatic juice for diagnosis of pancreatic carcinoma. Cancer 1994; 73:1589-94. [94207930]
- Caldas C, Hahn SA, Hruban RH, Redston MS, Yeo CJ, Kern SE. Detection of K-ras mutations in the stool(s) of patients with pancreatic adenocarcinoma and pancreatic ductal hyperplasia. Cancer Res 1994;54:3568- 73.
- Abbruzzese JL, Evans DB, Raijman I, Larry L, King T, Leach SD, et al. Detection of mutated c-Ki-ras in the bile of patients with pancreatic cancer. Anticancer Res 1997; 17:795-801. [97283277]
- Wilentz RE, Chung CH, Sturm PD, Musler A, Sohn TA, Offerhaus GJ, et al. Kras mutations in the duodenal fluid of patients with pancreatic carcinoma. Cancer 1998; 82:96-103. [98088760]
- Ito R, Tamura K, Ashida H, Nishiwaki M, Nishioka A, Yamamoto Y, et al. Usefulness of K-ras gene mutation at codon 12 in bile for diagnosing biliary strictures. Int J Oncol 1998;12:1019-23.
- Mulcahy HE, Lyautey J, Lederrey C, Qi Chen X, Anker P, Alstead EM, et al. A prospective study of K-ras mutations in the plasma of pancreatic cancer patients. Clin Cancer Res 1998 ;4:271-5. [98177554]
- Shibata K, Mori M, Kitano S, Akiyoshi T. Detection of ras gene mutations in peripheral blood of carcinoma patients using CD45 immunomagnetic separation and nested mutant allele specific amplification. Int J Oncol 1998;12:1333-8. [98256480]
- Mulcahy H, Farthing MJG. Diagnosis of pancreatico-biliary malignancy: detection of gene mutations in plasma and stool. Annals Oncol 1999; 10:S114-7.
- Gerhard M, Juhl H, Kalthoff H, Schreiber HW, Wagener C, Neumaier M. Specific detection of carcinoembryonicantigenexpressingtumor cells in bone marrow aspirates by polymerase chain reaction. J ClinOncol 1994; 12:725-9.
- Funaki NO, Tanaka J, Kasamatsu T, Ohshio G, Hosotani R, Okino T, Imamura M. Identification of carcinoembryonic antigen mRNA in circulating peripheral blood of pancreatic carcinoma and gastric carcinoma patients. Life Sci 1996; 59:2187-99. [97107583]
- Funaki NO, Tanaka J, Hosotani R, Kogire M, Suwa H, Imamura M. Quantitative analysis of carcinoembryonic antigen messenger RNA in peripheral venous blood and portal blood of patients with pancreatic ductal adenocarcinoma. Clin Cancer Res 1998; 4:855-60.
- Thorban S, Roder JD, Siewert JR: Detection of micrometastasis in bone marrow of pancreatic cancer patients. Ann Oncol 1999; 10(Suppl. 4):S111-3.
- Miyazono F, Takao S, Natsugoe S, Uchikura K, Kijima F, Aridome K, et al. Molecular detection of circulating cancer cells during surgery in patients with biliarypancreatic cancer. Am J Surg 1999; 177:475- 9. [99341663]
- Roder JD, Thorban S, Pantel K, Siewert JR. Micrometastases in bone marrow: prognostic indicators for pancreatic cancer. World J Surg 1999; 23:888-91.
- Liefers GJ, Cleton-Jansen AM, van de Velde CJ, Hermans J, van Krieken JH, Cornelisse CJ, Tollenaar RA. Micrometastases and survival in stage II colorectal cancer. N Engl J Med 1998; 339:223-8. [98328629]
- Rosa JA, Van Linda BM, Abourizk NN. New-onset diabetes mellitus as a harbinger of pancreatic carcinoma. J ClinGastroenterol 1989; 11:211-5.
- Permert J, Larsson J, Ihse I, Pour PM. Diagnosis of pancreatic cancer. Alteration of glucose metabolism. Int J Pancreatol 1991; 9:113-7.
- Fogar P, Basso D, Panozzo MP, Del Favero G, Briani G, Fabris C, et al.: C-peptide pattern in patients with pancreatic cancer. Anticancer Res 1993; 13:2577-80. [94182895]
- Permert J, Ihse I, Jorfeldt L, von Schenck H, Arnqvist H J, Larsson J. Pancreatic cancer is associated with impaired glucose metabolism. Eur J Surg 1993; 159:101-7.
- Fogar P, Pasquali C, Basso D, Sperti C, Panozzo MP, Tessari G, et al.: Diabetes mellitus in pancreatic cancer follow-up. Anticancer Res 1994; 14:2827-30. [95177591]
- Basso D, Plebani M, Fogar P, Del Favero G, Briani G, Meggiato T, et al. Beta cell function in pancreatic adenocarcinoma. Pancreas 1994; 3:332-5. [94294342]
- Wang F, Larsson J, Abdiu A, Gasslander T, Westermark P, Adrian TE, Permert J. Dissociated secretion of islet amyloid polypeptide and insulin in serum-free culture media conditioned by human pancreatic adenocarcinoma cell lines. Int J Pancreatol 1997; 21:157-64. [97353716]
- Permert J, Adrian T E, Jacobsson P, JorfeltFruin B, Larsson J. Is profound insulin resistance in patients with pancreatic cancer caused by a tumor-associated factor? Am J Surg 1993; 165:61-7.
- Basso D, Brigato L, Veronesi A, Panozzo MP, Amadori A, Plebani M. The pancreatic cancer cell line MIA PaCa 2 produces one or more factors able to induce hyperglycemia in SCID mice. Anticancer Res 1995; 15:132-8.
- Basso D, Valerio A, Brigato L, Panozzo MP, Miola M, Lucca T, et al. An unidentified pancreatic cancer cell product alters some intracellular pathways of glucose metabolism in isolated rat hepatocytes. Pancreas 1997; 15:132-8. [97406815]
- Valerio A, Basso D, Brigato L, Ceolotto G, Baldo G, Tiengo A, Plebani M. Glucose metabolic alterations in isolated and perfused rat hepatocytes induced by pancreatic cancer conditioned medium: a low molecular weight factor possibly involved. BiochemBiophys Res Commun 1999; 257:622-8. [99216328]
- Ding X, Flatt PR, Permert J, Adrian TE. Pancreatic cancer selectively stimulates islet b cells to secrete amylin. Gastroenterology 1998; 114:130-8.


