Keywords
Pancreaticoduodenectomy; Pancreaticojejunostomy; Pancreatitis; Surgery
Abbreviations
CJ: cystojejunostomy; CP: chronic pancreatitis; DPPHR: duodenumpreserving pancreatic head resection by Beger; PCJ: pancreo-cystojejunostomy; PD: pancreaticoduodenectomy by Whipple; PJ: pancreaticojejunostomy by Partington- Rochelle; PLP: left-pancreatectomy with pancraeticojejunostomy by Puestow with or without splenectomy; PPPD: pancreaticoduodenectomy pylorus-preserving by Longmire-Traverso
INTRODUCTION
Writing about the surgical treatment of chronic pancreatitis (CP) would seem to be relatively simple. Many have contributed to the published literature. One MEDLINE (PubMed) search, combining “chronic pancreatitis” and “surgical treatment" found 1,917 publications [1]. The major part of these quote results on series of patients treated with a definitive surgical procedure, drainage or resection, in accordance with the preference of the Center [2-15]. The indications for treatment are contingent upon the presence of pain defined by severity and degree of incapacity, the presence of pseudocysts, the involvement of the biliary tree and duodenum or the preoperative suspicion of neoplasia. Less common indications include hemorrhage, colonic obstruction, pancreatic ascites and pleural effusion [16-18]. Because morbidity and mortality are generally acceptable and longterm results are excellent regardless of the procedure performed, the symptomatic control of pain is of primary importance [2-15]. Furthermore, various studies report that more than 70% of patients are pain-free 5 years after surgery [3-6, 8-12, 15]. Although the results of surgical intervention are good, many questions still remain on the indications and choice of operation [19]. In addition, in the last few years, many things have changed in the nosologic framework of the disease. Certain etiological factors have been discovered, and new endoscopic interventions have added to the therapeutic armamentarium. All of these factors have resulted, at least in part, in the re-evaluation of the role of surgery in the treatment of CP and ultimately the choice of intervention. The purpose of this work, although possibly ambitious, is to illuminate which points are still controversial, old and new, and finally attempt to find a systematic approach to the surgical management of CP.
Indications for Surgical Treatment
As is well known, CP is a disease that results in the unrelenting destruction of the pancreas [20]. Histopathologically, this manifests itself as a progressive substitution of the gland with fibrotic tissue. On a functional level, there is a decrease in exocrine and endocrine pancreatic function [21]. Given its dynamic evolution, the histologic alterations of the parenchyma can be differentiated into various degrees which can improve the choice of treatment. Clearly, there are some symptoms that absolutely require surgical intervention, sometimes even urgently [22]. There are, however, other situations that need a step by step strategy, such as the management of intractable pain. In these cases, the therapeutic approach must focus on the etiological agents, alcohol and tobacco [23]. Numerous studies have demonstrated that at least one half of the patients with symptomatic pain who are treated conservatively will become pain free once they stop or reduce their alcohol intake [24-25]. Although there are programs to encourage rehabilitation in surgical centers, often, once a patient is sent to surgery, they are subjected to an operation without any future attempt at conservative management. In addition, it can become very difficult to convince both the patient and internist to wait when there is the presence of significant pain. A further problem exists: the definition of significant symptomatic pain and disability and how to interpret the pathogenesis. As is already known, the problem is not insignificant, the pain is the indication for treatment in the majority of cases and its trend is of fundamental importance in validating the results regardless of the treatment chosen.
Regarding the definition of pain, numerous scoring systems have been proposed in order to try to make this parameter objective, and, as of now, no system has currently been universally accepted [26-27]. It must also be remembered that the pain can be of nonpancreatic origin [22]. Regarding the genesis of pain, there are two principle pathogenic hypotheses. The basis of the first is that the pain is caused by increased intraductal and or parenchymal pressure due to decreased drainage of pancreatic juice into the duodenum [28-30]. The other more recent theory asserts that the symptomatology is due to the release of neurotransmitters into the inflammatory mass, usually located in the head of the pancreas [31]. Belief in either theory has important therapeutic implications. Supporting the first hypothesis is the belief that the palliation of pain can be obtained by improving pancreatic drainage, endoscopically or surgically. Meanwhile, supporters of the second theory maintain that palliation can only be obtained by resection of as much of the diseased gland as possible. Actually, the concepts are probably complementary: long-term results of resection and drainage on pain relief and patient well being are similar. However, the ability to distinguish which patients will benefit from which procedure still exists. Beger et al. noted that more than two thirds of their patients presented with a mass forming CP; yet in our experience, this ratio is reversed [7, 15, 26]. In the determination of various morphological features, perhaps the diverse types of alcoholic intake, beer or wine are significant; however, this has never been investigated. Complicating things further is the fact that in the course of the disease, pain tends to have a variable progression [32]. The initial years of the illness are characterized by a progressive exacerbation of pain that eventually leads to spontaneous remission corresponding morphologically to complete atrophy of the gland [33]. This aspect truly makes it difficult to ascertain the real benefit of surgical intervention on the treatment of pain [34], especially since about 50% of the patients that undergo surgical therapy benefit from it [7, 35]. These are old issues; today, there are two other problems that cloud the indications for surgery.
substantially to the understanding of the disease process and its complications; on the other, they have added other elements to the classification of the disease and its pathogenesis. Radiologists are now not merely diagnosticians because their descriptions can influence the choice of therapy. They not only comment on the presence of pseudocysts and the presence or absence of biliary and pancreatic ductal dilatation, but also on whether the pathology is diffuse or localized, uniform or chain-like or whether there is "groove pancreatitis" [36]. This last issue deserves further consideration. It has been noted that in about 20% of cases with CP there is a scar in the region of the "groove," between the C-loop of the duodenum and the head of the pancreas [37, 38]. This corresponds with our experience with cystic dystrophy in the duodenal wall, a lesion that necessitates surgical resection [15, 39, 40]. As a result, the correct therapeutic response is closely linked to the expertise of the radiologist.
Diagnostic imaging, aside from being fundamentally helpful, brings up another problem. Frequently, patients are sent to surgery with the radiographic finding of ductal dilatation but few episodes of pain. In these cases, the indications for treatment are born out of the hypothesis that decompression of the ductal system can lessen the progression of disease [41, 42]. In reality,at this time, there isn't sufficient clinical data to sustain such hypotheses. The surgeon must remember that the current therapeutic approaches are limited in their ability to control the symptoms.
One last aspect that partially modifies the need for surgery is the possibility of endoscopic treatment. In fact, endoscopy, which was initially used cautiously, has subsequently become more prevalent and is now a viable alternative to surgical intervention [43]. One realistic compromise is to consider the two approaches complementary instead of alternative. In fact, guidelines have been emerging that guide the clinician in the best therapeutic approach [44]. If there are no associated pathologies, surgery for pseudocysts that impinge on the stomach and duodenum or for the symptomatic relief of pain in association with obstructive chronic pancreatitis with calculi or para-papillary stenoses.should disappear from modern surgical practice. In all of these cases, initial therapeutic intervention should always be endoscopic with or without extracorporeal lithotripsy because it is minimally invasive; however, the stents must be temporary [45, 46]. In endoscopic studies, the long-term published results are promising [47-49]. These patients should only be sent to surgery in the event that the endoscopic procedure fails [43, 44].
Besides these last examples, there are still those patients who remain the exclusive domain of the surgeon. For example, surgery is indicated in patients having chronic pancreatitis associated with hemorrhage, duodenal or biliary stenosis, or with pseudocysts that are untreatable endoscopically. In addition, when it is impossible to preoperatively exclude the presence of neoplasia, whether solid or cystic, operative resection is required [43]. Finally, surgery is required in patients who suffer from pain refractory to medical treatment or those with a “chain of lakes” dilation of Wirsung’s duct in which the number of calculi and stenoses would make endoscopic intervention tenuous. Therefore, in the above-mentioned pathologies, as is often the case, surgery offers the advantage of resolving all the problems in one step.
The Choice of Surgical Intervention
Rarely are the indications for surgery obvious; even less so is the choice of procedure. Table 1 lists the main surgical operations in the treatment of symptomatic CP.
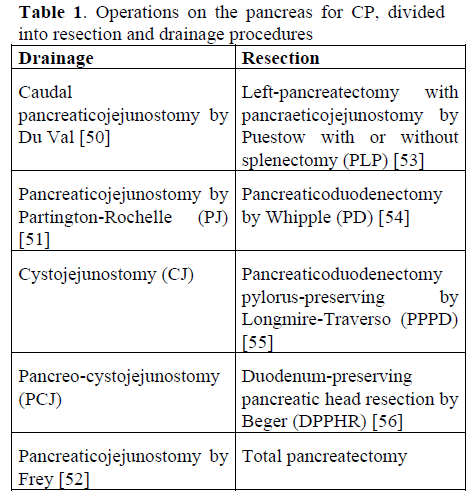
There are many options, even if some have more historical relevance, for example, the pancreaticojejunostomy by Du Val and the total pancreatectomy have been essentially abandoned. The others represent variations in technique of the same procedure; the evolution of another PD or PPPD often relies on the presence of a pseudocyst or a significant dilatation of the duct of Wirsung (PJ, CJ, and PCJ).
The surgeon must have several fundamental facts before deciding on a procedure. The progression of chronic pancreatitis on exocrine and endocrine insufficiency should advise the surgeon to preserve as much parenchyma as possible [2, 7]. All resective procedures must account for PD, PPPD, DPPHR and PLP drainage of the pancreatic ductal system. The length of the anastamosis seems to be directly proportional to painrelief. Morbidity and mortality, although very low in experienced centers, is proportional to the complexity of the operation, more so for resective than drainage procedures [7]. As already noted, after both drainage and resection, the percentage of patients that are pain-free in the long-term is nearly equal [2-6, 8-12, 15]. Due to the various morphologic presentations of CP, there will never be one optimal procedure for all patients [36].
All things considered, the choice of surgical intervention must be based on the morphology of the disease that can be gleaned from diagnostic imaging. A pseudocyst that involves the spleen must be treated by a PLP [19]. Mass forming CP in the head of the pancreas in which pre-operative diagnosis is impossible is best managed by a PPPD. From an oncologic point of view, this approach is not superior to the standard Whipple procedure; however, the post-operative course, return of bowel function and maintenance of nutritional status is significantly improved [57, 58]. This is also true in the event that the final histology reveals CP [59]. It is inadvisable to use a DPPHR when neoplasia is suspected, even when the histology of the removed pancreatic head is checked via frozen section [60]. If cancer is present, there is the theoretical possibility that neoplastic cells can be disseminated into the operative field and the peritoneal cavity. Because “groove pancreatitis” is often due to a cystic dystrophy of the duodenal wall, a PPPD would also be the operation of choice because a DPPHR would leave the source of the disease in the duodenum. When the diagnosis is known preoperatively, and there is a dilated pancreatic duct with or without an enlarged pancreatic head, drainage must be performed. This allows for the preservation of the maximum amount of pancreatic parenchyma. Among the various options, the pancreaticojejunostomy using the Frey procedure, consisting of a pancreaticojejunostomy with local excision of a small portion of the superior part of the head (approximately 5-gm. of the head), is superior. The pancreaticojejunostomy using the Frey procedure conserves the pancreaticobiliary- duodenal axis and the anastamosis is the largest drainage of the duct possible. The long-term results are similar to the DPPHR with less morbidity [60]. The difference between these last two procedures is that with the pancreaticojejunostomy by Frey, the transection of the pancreas in front of the portal vein, which is often difficult, is not necessary. The conservation of the duodenum, moreover, ensures better long-term control of glucose metabolism in contrast to the PPPD [61].
The classic PJ should be reserved only for those cases with selective dilation of Wirsung’s duct, as is observed in cases of obstructive CP due to scarring from a previous necrotizing pancreatitis. The presence of a pseudocyst, other than those localized in the tail, necessitates a drainage procedure. If the pseudocyst is in broad communication with the main duct, a CJ can be sufficient; however, if isolated, a PCJ is necessary [7]. The presence of an obstruction of the main biliary duct rarely presents as the only symptom; it is usually associated with pain or other complications such as the presence of a pseudocyst [44]. Other than the appearance of frank jaundice, the only sign of biliary involvement in the pancreatic process may be elevations in liver function tests [44, 62]. Stenosis of the intrapancreatic bile duct is usually the only site of concern. The choice of surgery will be based on the ultimate pathology or associated symptomatology. The suspicion of neoplasia can necessitate pancreatic head resection. If, however, a pancreatic drainage procedure is indicated, diversion of the biliary tract can be safely performed on the same Roux loop used for the pancreaticojejunostomy [7, 63-65].
Conclusions
involving CP. Based on the need to reduce morbidity and mortality, the creation of rigorous therapeutic protocols, at least in large and experienced centers, cannot be delayed. When possible, this should be preceded by an attempt at conservative management through a program of alcohol abstinence. In the proper scenario, the possibility of an endoscopic approach, which is less invasive than surgery, must be actively pursued. If surgery is indicated, the choice of operation must be based on the reason for which treatment had been sought and upon the various morphologic aspects revealed by diagnostic imaging. An approach indicated for a patient must be based on the stage of disease and not on previous biases. Taking into account the comparative results of surgical techniques, some operations should be abandoned due to greater morbidity. As many have noted, it is obvious that the future lies in the creation of pancreatic teams, in which surgeons will be one of the team players.
References
- National Library of Medicine. Pubmed. (Medline). https://www.ncbi.nlm.nih.gov/entrez/
- Prinz RA, Greenlee HB. Pancreatic duct drainage in 100 patients with chronic pancreatitis. Ann Surg 1981; 194:313-20.
- Hart MJ, Miyashita H, Morita N, White TT. Pancreaticojejunostomy report of a 25 year experience. Am J Surg 1983; 145:567- 70.
- Bradley EL III. Long term results of pancreaticojejunostomy in patients with chronic pancreatitis. Am J Surg 1987; 153:207-13.
- Greenlee HB, Prinz RA, Aranha GV. Long term results of side to side pancreaticojejunostomy. World J Surg 1990; 14:70-6.
- Prinz RA. Pancreatic duct drainage for chronic pancreatitis. In: Beger HG, Buechler MW, Malferthainer P, eds. Standards in Pancreatic Surgery. Berlin, Heidelberg: SprigerVerlag, 1993: 554-64.
- Pederzoli P, Falconi M, Bassi C, Vesentini S, Briani GF, Bonora A, Salvia R. Derivative surgical treatment. In: Pederzoli P, Cavallini G, Bassi C, Falconi M, eds. Facing Pancreatic Dilemma. Berlin, Heidelberg: SprigerVerlag, 1994: 199-213.
- Adams DB, Ford MC, Anderson MC. Outcome after lateral pancreaticojejunostomy for chronic pancreatitis. Ann Surg 1994: 219:481-9. [94241794]
- Moreaux J. Long term follow-up study of 50 patients with pancreaticoduodenectomy for chronic pancreatitis. World J Surg 1984; 8:346-53.
- Gall FP, Gebhardt C, Meister R, Zirnglib H, Schneider MU. Severe chronic cephalic pancreatitis: use of partial pancreaticoduodenectomy with the occlusion of the pancreatic duct in 289 patients. World J Surg 1989; 13:809-17.
- Beger HG, Buechler MW, Bittner R, Uhl W. Duodenum-preserving of the head of the pancreas in chronic pancreatitis of the inflammatory mass in the head. World J Surg 1990; 14:83-7.
- Howard JM, Zhang Z. Pancreaticoduodenectomy (Whipple resection) in the treatment of chronic pancreatitis. World J Surg 1990; 14:77-82.
- Easter DW, Cuschieri A. Total pancreatectomy with preservation of duodenum and pylorus for chronic pancreatitis. Ann Surg 1991; 214:575-80.
- Sawyer R, Frey CF. Is there still a role for in distal pancreatectomy in surgery for chronic pancreatitis? Am J Surg 1994; 168:6- 9. [94295888]
- Falconi M, Valerio A, Caldiron E, Salvia R, Sartori N, Talamini G, et al. Changes in pancreatic resection for chronic pancreatitis over 28 years in a single institution. Br J Surg 2000; 87:428-33. [20223094]
- Seiler CA, Friess H, Buechler MW. Thrombosis of the portal and splenic vein. In: Beger HG, Warshaw AL, Buechler MW, Carr-Locke DL, Neoptolemos JP, Russel C, Sarr MG, eds. The Pancreas. London: Blackwell Science, 1998: 761-5.
- Bradley EL III. In: Bradley EL III, ed. Complications of Chronic Pancreatitis: Medical and Surgical Management. Philadelphia: WB Saunders, 1982: 265-92.
- Neoptolemos JP, Winslet MC. Pancreatic ascites. In: Beger HG, Buechler MW, Ditschuneit H, Malferthainer P, eds. Chronic Pancreatitis. Berlin, Heidelberg: Springer Verlag, 1990: 269-79.
- Prinz RA. Surgical options in chronic pancreatitis. Int J Pancreatol 1993; 14:97-105. [94110678]
- Di Magno EP, Layer P, Clain JE. Chronic pancreatitis. In: Go VLW, Gardner FP, Lebenthal E, DiMagno EP, Scheele GA, eds. The Pancreas: Biology, Pathobiology and Disease. New York: Raven Press, 1993: 1433- 7.
- Kloeppel G, Maillet B. Pathology of acute and chronic pancreatitis. Pancreas 1993; 8:659-70.
- Russel C. Indications for surgery. In: Beger HG, Warshaw AL, Buechler MW, Carr-Locke DL, Neoptolemos JP, Russel C, Sarr MG, eds. The Pancreas. London: Blackwell Science, 1998: 815-23.
- Barnett JL, Owyang C. Medical management of chronic pancreatitis. In: Howard JM, Idezuki Y, Ihse I, Prinz RA, eds. Surgical Diseases of the Pancreas. Baltimore: Williams & Wilkins, 1998: 335-41.
- Trapnell JE. Chronic relapsing pancreatitis: a review of 64 cases. Br J Surg 1979; 76:471-5.
- Miyake H, Harada H, Kunichika K, Ochi K, Kimura I. Clinical course and prognosis of chronic pancreatitis. Pancreas 1987; 2:378-85.
- Beger HG, Buechler MW, Bittner RR, Oettinger W, Roscher R. Duodenumpreserving resection of the head of the pancreas in severe chronic pancreatitis. Ann Surg 1989; 209:273-8. [89165519]
- Knoefel WT, Bloechle C, Limmer JC, Kuechler T, Izbicki JR. Pathogenesis of pain and quality of life in chronic pancreatitis. In: Izbicki JR, Binmoeller KF, Soehendra N, eds. Chronic Pancreatitis: an Interdisciplinary Approach. Berlin, New York: De Gruyter, 1997: 15-30.
- Bradley EL III. Pancreatic duct pressure in chronic pancreatitis. Am J Surg 1982; 144:313-6.
- Ebbehoj N, Svendsen LB, Madsen P. Pancreatic tissue pressure in chronic obstructive pancreatitis. Scand J Gastroenterol 1984; 19:1066-8.
- Ebbehoj N. Pancreatic tissue fluid pressure and pain in chronic obstructive pancreatitis. Danish Med Bull 1993; 39:128- 33.
- Bockmann DE, Buechler MW, Malfertheiner P, Beger HG. Analysis of nerves in chronic pancreatitis. Gastroenterology 1988; 94:1459-69. [88196769]
- Cavallini G, Frulloni L, Pederzoli P, Talamini G, Bovo V, Bassi C, et al. Longterm follow-up of patients with chronic pancreatitis in Italy. Scand J Gastroenterol 1998; 33:880-9. [98425733]
- Amman RW, Akovbiantz A, Largiader F, Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 254 patients. Gastroenterology 1984; 86:820-8.
- Lankish PG. Prognosis. In: Beger HG, Warshaw AL, Buechler MW, Carr-Locke DL, Neoptolemos JP, Russel C, Sarr MG, eds. The Pancreas. London: Blackwell Science, 1998: 740-7.
- Talamini G, Bassi C, Falconi M, Sartori N, Salvia R, Di Francesco V, et al. Pain relapses in the first 10 years of chronic pancreatitis. Am J Surg 1996; 171:565-9.
- Freney PC. Radiology. In: Beger HG, Warshaw AL, Buechler MW, Carr-Locke DL, Neoptolemos JP, Russel C, Sarr MG, et al., eds. The Pancreas. London: Blackwell Science, 1998: 728-39.
- Becker V, Mischke U. Groove pancreatitis. Int J Pancreatol 1991; 10:173-82.
- Ioth S, Yamakawa K, Shimamoto K, Endo T, Ishigaki T. Groove pancreatitis. J Computed AssitTomogr 1994; 18:911-5.
- Colardelle P, Chochon M, Larvon L, Palazzo L, Flejou JF, Andrieu J. Dystrophiekystiquesur pancreas aberrant antro-bulbaire. GastroenterolClinBiol 1994; 42:277-80.
- Procacci C, Graziani R, Zamboni G, Cavallini G, Pederzoli P, Guarise A, et al. Cystic dystrophy of the duodenal wall: radiological findings. Radiology 1997; 205:741-7. [98055248]
- Nealon WH, Townsend CM, Thompson JC. Operative drainage of the pancreatic duct delays functional impairment in patients with chronic pancreatitis. Ann Surg 1988; 208:321- 9.
- Nealon WH, Thompson JC. Progressive loss of pancreatic function in chronic pancreatitis is delayed by main pancreatic duct decompression. Ann Surg 1993; 217:458-68. [93256638]
- Bassi C, Falconi M, Caldiron E, Salvia R, Sartori N, Valerio A, et al. To what extent is surgery superior to endoscopic therapy in the management of chronic pancreatitis.Ital J GastroenterolHepatol 1998; 30:571-8.
- Falconi M, Sartori N, Caldiron E, Casetti L, Salvia R, Bassi C, Pederzoli P. La pancreatitecronica: lineeguida per un razionaleapproccioterapeuticoendoscopico e chirurgico. Giornale Aggiornamenti PatologiaDigestiva 1999; 2:17-35.
- Delhaye M, Vandermeeren A, Baize M, Cremer M. Extracorporeal shockwave lithotripsy of pancreatic calculi. Gastroenterology 1992; 102:610-20.
- Sauerbruch T, Holl J, Sackmann M, Paumgartner G. Extracorporeal lithotripsy of pancreatic stones in patients with chronic pancreatitis and pain: a prospective follow up study. Gut 1992; 33:969-72.
- Cremer M, Deviere J, Delhaye M, Baize M, Vandermeeren A. Stenting in severe chronic pancreatitis: results of medium-term follow-up in seventy-six patients. Endoscopy 1991; 23:171-6.
- Binmoeller KF, Jue P, Seifert H, Nam WC, Izbicki J, Soehendra N. Endoscopic pancreatic stent drainage in chronic pancreatitis and dominant stricture: long term results. Endoscopy 1995; 27:638-44.
- Smits ME, Badiga SM, Rauws AJ, Titgat GN, Huibregtse K. Long-term results of pancreatic stents in chronic pancreatitis. GastrointestEndosc 1995; 42:452-6.
- Du Val MJ. Caudal pancreaticojejunostomy for chronic relapsing pancreatitis.Ann Surg 1954; 140:775-85.
- Partington PF, Rochelle RE. Modified Puestow procedure for retrograde drainage of the pancreatic duct. Ann Surg 1960; 152:1037-42.
- Frey CF, Smith GJ. Description and rationale for a new operation for chronic pancreatitis. Pancreas 1987; 2:701-7.
- Puestow CB, Gillesby WJ. Retrograde surgical drainage of pancreas for chronic pancreatitis. Arch Surg 1958; 76:898-906.
- Whipple AO, Pearson WB, Mullins CR. Treatment of carcinoma of the ampulla of Vater. Ann Surg 1935; 102:763-9.
- Traverso LW, Longmire WP. Preservation of the pylorus in pancreaticoduodenectomy. SurgGynecolObstet 1978; 146:659-62.
- Beger HG, Krautzberger W, Bittner R, Buchler M, Limmer J. Duodenum-preserving resection of the head of the pancreas in patients with severe chronic pancreatitis. Surgery 1985; 98:467-73. [85168757]
- Kozuscheck W, Reith HB, Waleczech H, Haarmann W, Edelmann M, Sonntag D. A comparison of long term results of the standard Whipple procedure and the pylorus preserving pancreaticoduodenectomy. J Am CollSurg 1994;178:443-53.
- Di Carlo V, Zerbi A, Balzano G, Corso V. Pylorus-preserving pancreaticoduodenectomy versus conventional Whipple operation. World J Surg 1999; 23:920-5. [99380692]
- Martin RF, Rossi RL, Leslie KA. Long term results of pylorus-preserving pancreaticoduodenectomy for chronic pancreatitis. Arch Surg 1996; 131:247-52. [96197921]
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T, Binmoeller KF, Broelsch CE. Duodenum preserving resection of the head of the pancreas in chronic pancreatitis. A prospective, randomized trial. Ann Surg 1995; 221:350-8. [95243757]
- Izbicki JR, Bloechle C, Broering DC, Knoefel WT, Kuechler T, Broelsch CE. Extended drainage versus resection in surgery for chronic pancreatitis. Prospective randomized trial comparing the longitudinal pancreaticojejunostomy combined with local pancreatic head excision with the pyloruspreservingpancreaticoduodenectomy. Ann Surg 1998; 228:771-9. [99075819]
- Stahl TJ, O’ConnorsAM, Ansel HJ, Venes JA. Partial biliary obstruction caused by chronic pancreatitis. Ann Surg 1998; 207:26-32.
- Prinz RA, Aranha GV, Greenlee HB. Combined pancreatic duct and upper gastrointestinal and biliary tract drainage in chronic pancreatitis. Arch Surg 1985; 120:361-6.
- Warshaw AL. Conservation of pancreatic tissue by combined gastric, biliary, and pancreatic duct drainage for pain for chronic pancreatitis. Am J Surg 198; 149:563-9.
- Sugerman HJ, Barnhart GR, Newsome HH. Selective drainage for pancreatic, biliary, and duodenal obstruction secondary to chronic fibrosing pancreatitis. Ann Surg 1986; 203:558-67.

