Stanislaw Hac1, Adam Nalecz2, Marek Dobosz3, Krzysztof Radziszewski4, Jacek Reszetow1, Kazimierz Jaskiewicz2, Zbigniew Sledzinski1
Departments of 1General Endocrine and Transplant Surgery, 2Pathology, and 3Surgical Nursing,
Medical University of Gdansk; 4Department of Mathematics, University of Gdansk.
Gdansk, Poland
- *Corresponding Author:
- Stanislaw Hac
Department of General Endocrine and
Transplant Surgery
Medical University of Gdańsk
7 Dębinki street
80-952 Gdańsk
Poland
Phone: +48-58.349.2410
Fax: +48-58.349.2410
E-mail: sthac@amg.gda.pl
Received November 29th, 2006 - Accepted January, 3rd, 2007
Keywords
Anatomy; Autopsy; Pancreas; Pancreatic Ducts
INTRODUCTION
Studies of the anatomy of the pancreas have been carried out for over 200 years. The first pancreatic observation performed on autopsy was described by the Greek, Erasistratus of Chios (319-250 B.C.) [1, 2]. The pancreatic duct and its function was discovered by Wirsung in 1642 [3]. About 80 years later, Santorini described the accessory pancreatic duct [4]. The relationship between pancreatic embryogenesis and the anatomy of the duct was established later on. Careful anatomical studies revealed the blood supply of the pancreatic gland. The role of the pancreas and understanding it led to the development of pancreatic surgery. The first pancreatic resection was described by Kausch in 1912 [5]. The main problem in pancreatic resection was pancreatico-entero or -gastro anastomosis [6, 7, 8, 9]. The pancreas varies in size, density and in the location of the pancreatic duct within the cut-line. Various authors have suggested that a uniform system of locating the pancreatic duct in a pancreatic crosssection would be useful for future anatomical studies and comparisons.
The aim of the study was to evaluate the uniform descriptive system of the location of the pancreatic duct within the pancreatic cross-section specimen taken from cadavers.
ETHICS
The procedure was based on The Medical University Ethics Committee agreement (No NKEBN/191/2004).
STATISTICS
The descriptive statistics reported are: means, standard deviations (SD), ranges, and 95% confidence intervals (95% CI). A linear correlation model was applied in order to analyze the data. Statistical evaluations were performed by running the SPSS for Windows 13.0 (SPSS Inc, Chcago, IL, USA) and the STATISTICA 7 version 1 (StatSoft, Inc. Tulsa, OK, USA) packages on personal computers.
METHODS
Twenty-seven consecutive pancreatic cadaveric specimens were analyzed (14 males, 13 females; age: mean±SD 68.1±14.5 years, range 31-84 years). Patients with a history of pancreatic disease were excluded. Autopsies were performed in the standard way within 24-40 hours from death. The omental sac was opened and the duodenum was liberated from the retroperitoneal space. The hepato-duodenal ligament and superior mesenteric vessels were excised. The pancreas was gently removed from the retroperitoneal space together with the duodenum. The entire specimen was mounted on a slide and a probe was introduced into the portal vein to identify the location of the pancreatic isthmus. The cut-line was carried out at a right angle to the pancreatic axis over the probe. The section was made using a disposable blade (Swan and Morton Nr 24, Sheffield, United Kingdom). Then, the whole pancreatic gland was left in a 4% formaldehyde solution for 5 days.
Standard hematoxylin/eosine staining was performed followed by frozen specimen preparation. Each specimen contained an entire plane of the cross-section. The section was evaluated under a light microscope at a 40x magnification; the main pancreatic duct was identified and measured. Then the specimen was photographed (Cannon Power Shot Pro1, Tokyo, Japan) with 2,272x1,704 dpi in super-macro option. The picture was digitally combined with a right angle coordinate system. The pancreatic cross-section was evaluated as a geometric ellipse, and the location of pancreatic duct and vessels were based on coordinates. The largest distance from back to front and the largest distance between the lower and the upper margin of the specimen was established as 100%, respectively. The Wirsung duct identified under the light microscope was found on photography and was described by two fraction co-ordinates. The details of the model described are presented in Figure 1.
Figure 1. Pancreatic cross-section specimen after H&E
staining combined with X and Y coordinates. The
Wirsung duct (arrow) is identified and described by (X;
Y) coordinates. The maximum length and high of
pancreatic specimen is established as 100, respectively.
On the left side, metric scale.
RESULTS
Analyzing the cross-section plane of the pancreatic isthmus, the mean size of the pancreatic isthmus cross-section was 10.46±2.34 mm in width and 25.55±4.56 mm in length. The mean vertical/horizontal distance ratio was 0.42±0.12 and the mean size of the main pancreatic duct was 1.02±0.49 x 2.46±0.79 mm. The coordinates of the mean distribution of the main pancreatic duct were: X 51.23±12.50; Y 50.60±8.51. The results are presented in Table 1. The graphic distribution of the main pancreatic duct in the cross-section of the isthmus is shown in Figure 2. A significant relationship was observed between the coordinates of the Wirsung duct position (Y = 68.928 - 0.358 X; r = -0.525; P=0.005). The blue ellipse represents the 95% CI of the bivariate normal distribution of the main pancreatic duct localization.
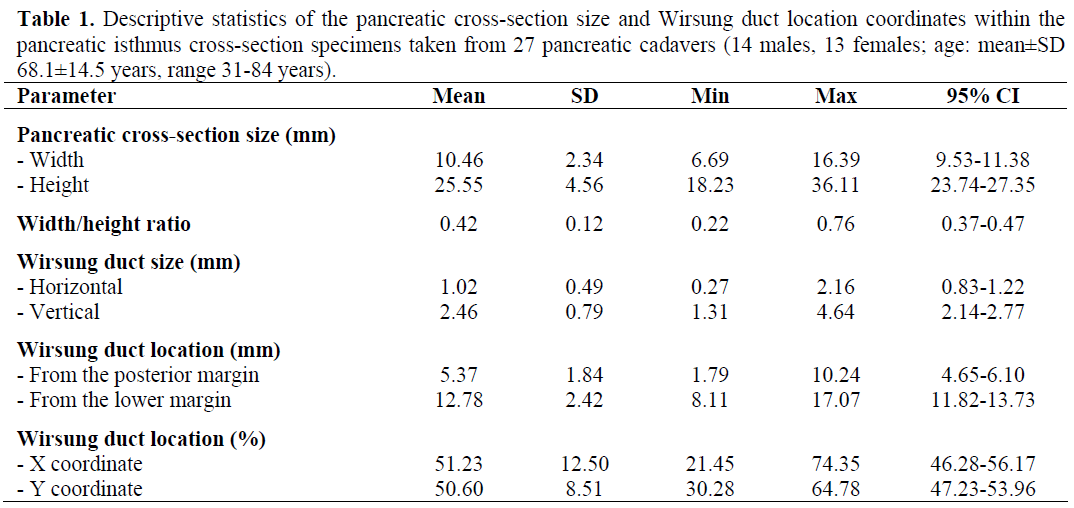
Figure 2. The Wirsung duct position within the
pancreatic isthmus cross-section presented in a
proportional system. The left side is the dorsal part and
the upper one is cephalic. Both scales (X and Y)
represent 100 of pancreatic cross-section width and 100
of height. A significant relationship was observed
between the coordinates of the Wirsung duct position
(Y = 68.928 - 0.358 X; r = -0.525; P=0.005). The blue
ellipse represents the 95% CI of the bivariate normal
distribution of the main pancreatic duct localization
(STATISTICA 7 version 1).
DISCUSSION
The first description of the pancreatic duct was made by Wirsung in 1642. The anatomical and physiological studies provided the necessary information for developing pancreatic surgery. The isthmus is the part of the pancreatic gland localized between the head and the corpus, situated over the portal vein. The pancreatic isthmus is the part of the gland with a relatively thin layer of tissue and the most common cross-section site regardless of the pancreatic resection method [6, 7, 8]. Pancreatic cross-section topography is one of the most important factors in pancreaticoentero reconstruction [10]. Technical reports of pancreatic anastomosis stress the importance of identifying the pancreatic duct before reconstruction [11]. There is no uniform system for describing the details of cross-section anatomy.
The model described was obtained from cadaver specimens in order to obtain uniform material in a relatively short time. All specimens were fixed in a 4% formaldehyde solution for 5 days. Fixation resulted in dehydration and gland texture change. The entire pancreas is made up of the same kind of tissue; thus, the Authors believe that the gland proportions taken into consideration in the study were not changed. The cross-section size and the pancreatic duct diameter might be diminished only after fixation.
Pancreatic stump suture placement requires knowledge of the location of the intrapancreatic duct and vessels. Several authors, in evaluating the pancreatico-entero anastomosis formation, took into consideration the pancreatic isthmus crosssection configurational anatomy [7, 11]. Other studies have stressed the blood supply and the pancreatic duct diameter [6]. Some authors believe that a description of the pancreatic cross-section might help in evaluating factors important in analyzing surgical complications. The anatomy of the pancreatic and the common bile ducts is usually obtained by endoscopic (ERCP) or nuclear resonance cholangiopancreatography (MRCP). These findings do not give information about the cross-section configuration of the pancreatic ducts or vessels [12, 13, 14, 15].
Several authors have described pancreatic duct localization in the pancreatic head or the isthmus cross-section using the metric scale [16]. The main pancreatic duct location is well-known although there is no uniform system describing the duct position. Wilasrusmee et al. described the distance of the Wirsung duct from the four margins of the pancreatic cross-section [17]. Some authors have concluded that the Wirsung duct was most often located in the posterior/superior quadrant of the head cross-section. Individual variability makes it difficult to compare the different shapes and sizes of the gland or the varying results of several different authors
CONCLUSION
A proportional system could be successfully used for anatomical studies of the pancreatic cross-section. The proportional system facilitates the establishment of the most frequent locations of pancreatic ducts and other structures within the specimen. Moreover, this system may be introduced in anatomical studies of cross-sections of the entire pancreatic gland. The proportional parametric system is also easy to analyze statistically and compare the results of the various research groups.
Acknowledgment
We thank to Miss Justyna Nawrot for her language assistance and Mr Leszek Moron for his help
References
- Behr GH. Dissertatioinauguralisanatomicomedica, de PancreateejusqueLiquore, quam, archiatrosummopraeside, conesensu ac indultugaratiosissimaefacultatismedicae in celeberrimaargentinensiumuniverstate, prolicentiasummos in arte medicahonores.Argentorari, SimonisKursneri. Strasburg, 1730:6-7.
- McClusky DA 3rd, Skandalakis LJ, Colborn GL, Skandalakis JE. Harbinger or hermit? Pancreatic anatomy and surgery through the ages.Part 3. World J Surg 2002; 26:1512-24. [PMID 12370786]
- Howard JM, Hess W, Traverso W. Johan Georg Wirsung (1589-1643) and the pancreatic duct: the professor of Padua, Italy. J Am CollSurg 1998; 187:201-11. [PMID 9704970]
- Santorini GD. Observationesanatomicae. Venetiis, apus JB Recurti, 1724.
- Kausch W. Das carcinom der papilla duodeni und seine radikaleentfernung. BeitragezurKlinischenChirurgie 1912; 78:439-86.
- Strasberg SM, Drebin JA, Mokadam NA, Green DW, Jones KL, Ehlers JP, Linehan D. Prospective trial of a blood supply-based technique of pancreaticojejunostomy: effect on anastomotic failure in the Whipple procedure. J Am CollSurg 2002; 194:746-58. [PMID 12081065]
- Hosotani R, Doi R, Imamura M. Duct-to-mucosa pancreaticojejunostomy reduces the risk of pancreatic leakage after pancreatoduodenectomy. World J Surg2002; 26:99-104. [PMID 11898041]
- Hagai H. Configurational anatomy of the pancreas: its surgical relevance from ontogenetic and comparative anatomical viewpoints. J HepatobiliaryPancreatSurg 2003; 10:48-56. [PMID 12918457]
- Kimura W. Surgical anatomy of pancreas for limited resection. J HepatobiliaryPancreatSurg 2000; 7:473-9. [PMID 11180873]
- KonishiM, Ryu M, Kinoshita T, Inoue K. Pathophysiology after pylorus-preserving pancreatoduodenectomy: a comparative study of pancreatogastrostomyand pancreatojejunostomy. Hepatogastroenterology1999; 46:1181-6. [PMID 10370688]
- Kim SW,Youk EG, Park YH. Comparison of pancreatogastrostomy and pancreatojejunostomy after pancreatoduodenectomy performed by one surgeon.World J Surg 1997; 21:640-3. [PMID 9230663]
- Aube C, HentatiN,Tanguy JY, Fournier HD, Papon X, Lebigot J, Mercier P. Radio-anatomic study of the pancreatic duct by MR cholangiopancreatography. SurgRadiolAnat 2003;25:64-9. [PMID 12647024]
- Laing AD, Gibson RN. Magnetic resonance cholangiopancreatography.AustralasRadiol 1999; 43:284-93. [PMID 10901920]
- Matar LD, Frazer C. Two-tone pancreas on T1- weighted images: correlation with abnormalities on magnetic resonance pancreatography. AustralasRadiol2001; 45:58-61. [PMID 11259975]
- Kamisawa T,Yuyang T, Egawa N, Ishiwata J, Okamoto A. Patency of the accessory pancreatic duct in relation to its course and shape: a dye-injection endoscopic retrograde pancreatography study. Am J Gastroenterol 1998; 93:2135-40. [PMID 9820386]
- Uchida T, Takada T, Ammori BJ, Suda K, Takahashi T. Three-dimensional reconstruction of the ventral and dorsal pancreas: a new insight into anatomy and embryonic development.J HepatobiliaryPancreatSurg 1999; 6:176-80. [PMID 10398906]
- Wilasrusmee C, Pongchairerks P. Pancreaticobiliary ductal anatomy in Thai People. J HepatobiliaryPancreatSurg 1999; 1:79-85. [PMID10436241]



