Keywords
Pancreatic Neoplasms; Pancreatitis
INTRODUCTION
In 1982, Stolte et al. coined the term ‘‘groove pancreatitis’’ and described it as a special form of segmental pancreatitis characterized by fibrous scarring of the anatomic space between the dorsocranial part of the head of the pancreas, the duodenum and the common bile duct. This type of pancreatitis has been reported under various names in the literature including paraduodenal pancreatitis [1, 2], cystic dystrophy of heterotopic pancreas [3, 4], pancreatic hamartoma of duodenum [5], myoadenomatosis and peri-ampullary duodenal wall cyst. Becker and Mischke in 1991 classified groove pancreatitis into a pure form and a segmental form [6]. Groove pancreatitis in the pure form involves the groove only, with preservation of the pancreatic parenchyma and the main pancreatic ducts. The segmental form of groove pancreatitis involves both the groove and the head of the pancreas with stenosis of the pancreatic duct causing upstream dilatation [1].
Clinically, this particular pancreatic inflammation is found predominantly in male patients (40-50 years) with a history of alcohol abuse. The clinical setting is similar to the usual form of chronic pancreatitis, but recurrent vomiting, attributable to marked duodenal stenosis with impaired motility and weight loss, tends to be more pronounced in groove pancreatitis [2, 4]. Jaundice develops in 20% of the patients [1, 2] and, if present, often fluctuates, in contrast to the continuously progressive jaundice found in patients with pancreatic carcinoma [5].
Recently, reports have described pancreatic cancers arising from the groove, called pancreatic groove carcinoma [7, 8, 9, 10]. Several studies have been attempted to clarify the points of differentiation between carcinoma and pancreatitis in the groove area [7, 11, 12]. This discrimination has been proved to be difficult; frequently the definitive diagnosis is only obtained after surgical intervention.
The purpose of this study is to report a case and review the clinical, radiological and pathological characteristics of groove pancreatic carcinomas and groove pancreatitis. We try to show that groove pancreatitis can coexist with pancreatic carcinoma or may even mask it. We further discuss the relevant radiological features which may help differentiate these two pathologies, which should form part of the differential diagnosis of any groove pathology.
CASE REPORT
A 58-year-old male, with a history of alcohol excess, presented with 4 months of upper abdominal pain associated with weight loss and vomiting. The patient was initially admitted and managed at a primary hospital where US and CT were carried out and a diagnosis of groove pancreatitis was made Duodenoscopy revealed gastric outflow obstruction secondary to duodenal stenosis and attempts at dilatation failed. There was no mucosal ulceration or erosion seen at site of stenosis. Biopsies at D1 and D2 were taken and revealed chronic active duodenitis. He underwent a gastrojejunostomy and truncal vagotomy as he did not tolerate enteral feeding. Histology of the biopsies performed intra-operatively did not demonstrate any malignancy. A follow-up endoscopy revealed a diverticulum in the first part of the duodenum and a tight stricture that prevented entry into the second part of the duodenum.
The patient then developed painless obstructive jaundice four months after the procedure. As the clinical features changed and became more sinister, CT scan was repeated, following which a referral was made to the tertiary regional HPB unit. The pre-bypass CT had shown inflammation in the groove with cystic changes in the duodenal wall. A repeat CT at our centre showed a major difference in that there was significant dilatation of the bile duct with a stenosis at the cystic duct insertion site, but the pancreatic duct was not significantly dilated. This was followed by a failed ERCP due to duodenal stenosis hence percutaneous transhepatic cholangiogram and biliary drainage was carried out. MRCP showed a small non enhancing area of low T1 signal within the pancreatic head surrounding the intra-pancreatic common bile duct extending to the ampulla of uncertain significance. CT and MRI scans revealed deleted a soft tissue mass in the head of the pancreas, abutting his superior mesenteric vein (Figures 1 and 2).
Figure 1. Pre-operative abdominal CT. a. Transverse CT with arrow
indicating the soft tissue mass in head of pancreas and dilatation of
the intra and extrahepatic biliary tree. b. Coronal CT with arrow
illustrating deleted cystic changes of duodenal wall and intra and
extra hepatic dilatation.
Figure 2. Pre-operative MRCP. a. Coronal MRCP images
illustrating soft tissue mass in head of pancreas and dilatation of the
intra and extrahepatic biliary tree. b. Coronal MRCP illustrating intra
and extrahepatic biliary duct dilatation.
At his initial presentation the history, clinical and radiological findings were representative of acute pancreatitis and in this case groove pancreatitis due to its location, but over the following 4 months the clinical scenario had changed to one more suspicious of pancreatic adenocarcinoma. He was discussed in a multidisciplinary meeting and as malignancy could not be rules out irrespective of the negative biopsies a decision to proceed to surgical resection was made and he underwent a Whipple’s pancreaticoduodenectomy.
The pancreas carcinoma did not invade the duodenal mucosa macroscopically but the histopathology report demonstrated cystic areas in both medial and lateral walls of his duodenum microscopically consistent with groove pancreatitis and a moderate to poorly differentiated adenocarcinoma (pT3 N1 V1 R1). The relationship of the carcinoma in this case shows this to be a primary pancreatic ductal carcinoma infiltrating the head of the pancreas with concentric involvement of the distal bile duct with inflammatory changes in the groove and pancreatic head, with normal pancreatic parenchyma present only at the distal pancreatic resection margin. There was also an incidental localized IPMN of the side branch duct type in the head. He made an uncomplicated post-operative recovery and completed adjuvant chemotherapy (gemcitabine) as part of the European Study Group for Pancreatic Cancer (ESPAC) 4 trial. Unfortunately, he was diagnosed with a primary lung squamous cell carcinoma and died 9 months later.
DISCUSSION
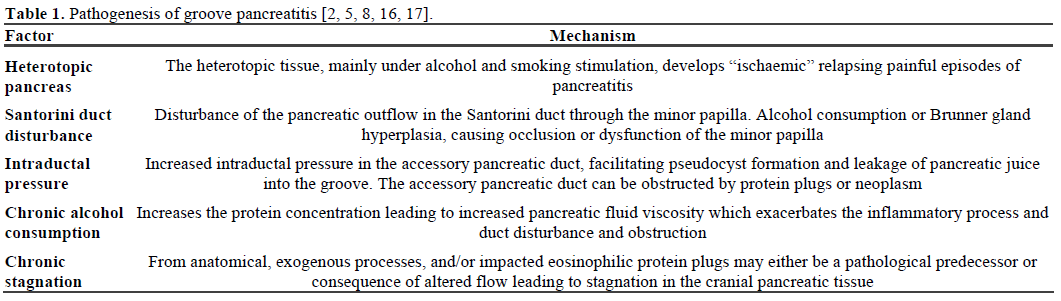
Groove pancreatitis is often diagnosed in 40- to 50- year-old men, with history of alcohol excess in the majority of cases [13, 14]. The initial presentation includes postprandial abdominal pain, impaired motility, vomiting, weight loss and less common presentation is jaundice. The duration of clinical symptoms ranges from few weeks to more than one year [13, 14, 15]. The pathogenesis of groove pancreatitis is unclear, most likely it is due to pancreatic heterotopia in the duodenum or anatomic variation in the region of minor papilla that lead to outflow obstruction and associated with excess alcohol intake [2, 16, 17]. Table 1 shows all suggested mechanisms for pathogenesis of groove pancreatitis.
Investigations usually include endoscopy (with or without EUS) and cross sectional imaging (CT and MRI). Upper gastrointestinal endoscopy can reveal an inflamed and polypoid duodenal mucosa with stenosis of the duodenal lumen [18, 19]. An ERCP is usually difficult to accomplish because of duodenal stenosis, but when successful it can demonstrate distal smooth common bile duct stenosis without abnormality of the main pancreatic duct [15, 17, 18]. The distinction between fibrous scarring in groove pancreatitis and adenocarcinoma of pancreas is difficult on endoscopic ultrasonography, CT and MRI [6, 7, 12, 15, 19]. EUS provides an accurate location and extension of the disease; however, distinction between inflammation and cancerous infiltration is difficult.
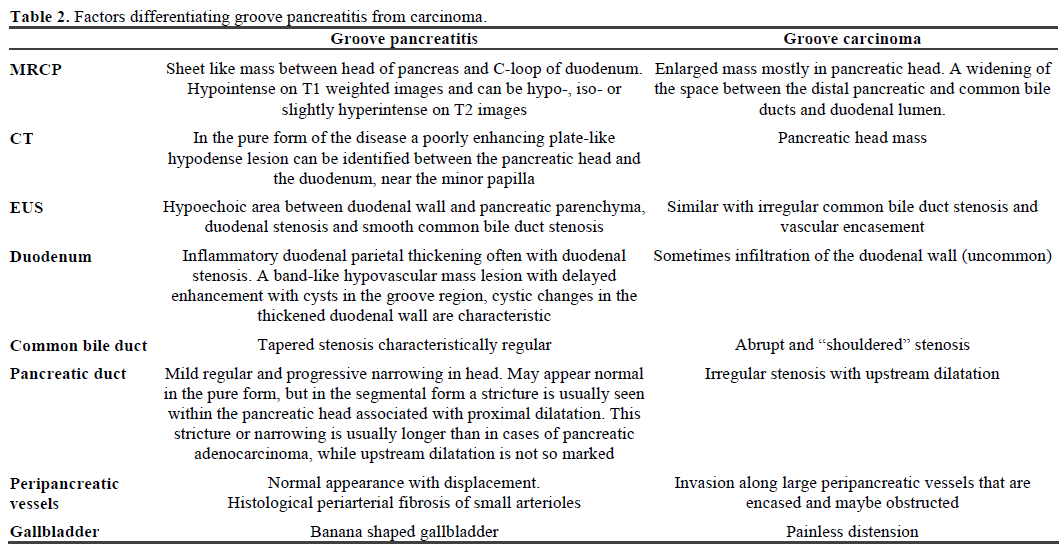
Computed tomography demonstrates groove pancreatitis well [16] but recently, Gabata et al. have demonstrated that pancreatic carcinomas arising in the groove area cannot be reliably differentiated from groove pancreatitis with CT and MRI imaging when there are no cystic lesions within the mass and/or the thickened duodenal wall [7]. The differential diagnosis of the pure form of grove pancreatitis includes duodenal cancer, cholangiocarcinoma, acute pancreatitis or chronic pancreatitis. In cases of segmental form of groove pancreatitis, the differential diagnosis from pancreatic carcinoma is challenging. Table 2 shows differences between the two pathologies which may help diagnosis.
The histopathological hallmark of groove pancreatitis is the presence of scar tissue with fibrosis in pancreaticoduodenal groove or in the groove and the superior portion of the pancreatic head (in the pure and segmental forms of the disease, respectively). Histologically, groove pancreatitis causes either thickening or scarring of the duodenal wall, particularly in the area corresponding to the minor papilla, that extend to the adjacent pancreatic head tissue and/or sieve-like cystic changes in the duodenal wall. The cysts contain clear fluid, but others may have more granular white material and even stones. The fibrotic tissue that develops in the wall of the pancreas, also involves the groove between the wall and the pancreatic tissue may compress and indent the common bile duct [2]. The different aspects of microscopic pathologic features associated with groove pancreatitis are reflected by the various terms describing this entity in the literature [1, 3, 4, 5, 16]. In typical cases there is a chronic inflammatory process that resides in the duodenal submucosa and the adjacent pancreatic tissue, several small foci of necrosis surrounded by a dense proliferation of myoid cells. There are often cystically dilated ducts and hyperplasia of Brunner’s glands is also a major finding that is seen in almost all cases [2]. The duodenum is always involved by a chronic inflammatory process, with scar tissue in the wall leading to fibrosis and various levels of stenosis.
Conservative measures including analgesics, pancreatic rest, and abstinence from alcohol are usually successful at treating initial symptoms, but may not be longlasting. Effectiveness of conservative management should be reassessed regularly according to symptoms, imaging and biochemical results. Endoscopic drainage of a stenotic or occluded via the minor duct has been reported with good initial results. The presence of intractable pain and/or pancreatic insufficiency (weight loss, steatorrhoea or diabetes), can be attributed to the severe inflammatory and fibrotic changes observed in the head of pancreas often associated with duodenal obstruction secondary to scarring or cystic dystrophy. Occasionally, groove pancreatitis is resistant to medical treatment and follows prolonged course, so surgical intervention in the form of a pancreaticoduodenectomy may be required at a late phase of the disease, resulting in symptomatic relief [20] and can lead to adequate weight gain [20]. Surgery is often required to definitively rule out a pancreatic neoplasm. Groove pancreatitis is classified as a rare disease, but this might be partly due to lack of awareness of this condition.
In conclusion, groove pancreatitis is a very interesting uncommon pancreatic disease with challenging imaging diagnosis that can lead to surgical dilemmas. This condition should be considered when making the differential diagnosis between pancreatic masses and duodenal stenosis. Therefore, awareness of the possibility that a focal pancreatic lesion depicted on imaging studies may represent groove pancreatitis should influence the surgeon to perform further investigation before radical surgery is attempted. On the other hand, in any case of a questionable pancreatic head mass, before making the diagnosis of groove pancreatitis, the possibility of adenocarcinoma ought to be carefully excluded.
Conflicts of interest
None
Financial support
None
References
- Adsay NV, Zamboni G. Paraduodenal pancreatitis: a clinicopathologically distinct entity unifying ''cystic dystrophy of heterotopic pancreas'', ''para-duodenal wall cyst'', and ''groove pancreatitis''. SeminDiagnPathol 2004; 21:247-54. [PMID 16273943]
- Kloppel G. Chronic pancreatitis, pseudotumors and other tumorlike lesions. Mod Pathol 2007; 20(Suppl. 1):S113-31. [PMID 17486047]
- Fléjou JF, Potet F, Molas G, Bernades P, Amouyal P, Fékété F. Cystic dystrophy of the gastric and duodenal wall developing in heterotopic pancreas: an unrecognised entity. Gut 1993; 34:343-7. [PMID 8097180]
- Parc R, Soprani A, Louvel A. Heterotopic cystic pancreas of the duodenal wall without associated chronic pancreatitis. J Chir (Paris) 1977; 114:185-92. [PMID 925106]
- McFaul CD, Vitone LJ, Campbell F, Azadeh B, Hughes ML, Garvey CJ, et al. Pancreatic hamartoma. Pancreatology 2004; 4:533- 7. [PMID 15340246]
- Becker V. Bauchspeicheldruse (Inselapperatausgenommen). In: Doerr W, ed. SpeziellepathologischeAnatomie. Berlin, Germany: Springer, 1973.
- Gabata T, Kadoya M, Terayama N, Sanada J, Kobayashi S, Matsui O. Groove pancreatic carcinomas: radiological and pathological findings. EurRadiol 2003; 13:1679-84. [PMID 12835985]
- Tan CH, Chow PK, Thng CH, Chung AY, Wong WK. Pancreatic adenocarcinoma that mimics groove pancreatitis: case report of a diagnostic dilemma. Dig Dis Sci 2006; 51:1294-6. [PMID 16944029]
- BadiaBartolome C, Diaz Formoso FJ, Rodriguez Falcon R, Marchena Gomez J. Groove pancreatitis and its differential diagnosis with pancreatic adenocarcinoma. GastroenterolHepatol 2009; 32:22- 8. [PMID 19174095]
- Aimoto T, Uchida E, Nakamura Y, Katsuni A, Chou K, Kawamoto M, et al. Clinicopathologic study on pancreatic groove carcinoma. Pancreas 2006; 33:255-9. [PMID 17003647]
- Ishigami K, Tajima T, Nishie A, Kakihara D, Fujita N, Asayama Y, et al. Differential diagnosis of groove pancreatic carcinomas vs. groove pancreatitis: Usefulness of the portal venous phase. Eur J Radiol 2010; 74:e95-100. [PMID 19450943]
- Itoh S, Yamakawa K, Shimamoto K, Endo T, Ishigaki T. CT findings in groove pancreatitis: correlation with histopathological findings. J Comput Assist Tomogr 1994;18:911-5. [PMID 7962798]
- Becker V, Mischke U. Groove pancreatitis. Int J Pancreatol 1991; 10:173-82. [PMID 1787332]
- Stolte M, Weiss W, Volkholz H, Rosch W. A special form of segmental pancreatitis: ''groove pancreatitis''. Hepatogastroenterology 1982; 29:198-208. [PMID 7173808]
- Balakrishnan V, Chatni S, Radhakrishnan L, Narayanan VA, Nair P. Groove pancreatitis: a case report and review of literature. JOP. J Pancreas (Online) 2007; 8:592-7. [PMID 17873465]
- Triantopoulou C, Dervenis C, Giannakou N, Papailiou J, Prassopoulos P. Groove pancreatitis: a diagnostic challenge. EurRadiol 2009; 19:1736-43. [PMID 19238393]
- Sanada Y, Yoshida K, Itoh H, Kunita S, Jinushi K, Matsuura H. Groove pancreatitis associated with true pancreatic cyst. J HepatobiliaryPancreatSurg 2007;14:401-9. [PMID 17653641]
- Shudo R, Yazaki Y, Sakurai S, Uenishi H, Yamada H, Sugawara K, et al. Groove pancreatitis: report of a case and review of the clinical and radiologic features of groove pancreatitis reported in Japan. Intern Med Jul 2002; 41:537-42. [PMID 12132521]
- Mohl W, Hero-Gross R, Feifel G, Kramann B, Puschel W, Menges M, et al. Groove pancreatitis: an important differential diagnosis to malignant stenosis of the duodenum. Dig Dis Sci 2001; 46:1034-8. [PMID 11341646]
- Rahman SH, Verbeke CS, Gomez D, McMahon MJ, Menon KV. Pancreatico-duodenectomy for complicated groove pancreatitis. HPB (Oxford) 2007; 9:229-34. [PMID 18333228]



