Åke Andrén-Sandberg and Tommy Ivanics
Division of Surgery, Department of Clinical Science, Intervention and Technology (CLINTEC),
Karolinska Institutet, Stockholm, Sweden
- *Corresponding Author:
- Åke Andrén-Sandberg
Department of Clinical Science
Karolinska University Hospital
141 86 Stockholm, Sweden
Tel: + 46 (0) 70-222 15 77
Fax: + 46 (0) 8-585 823 40
E-mail: ake.andren-sandberg@karolinska.se
Received January 28th, 2018 - Accepted January 30th, 2018
Keywords
Pancreatoduodenectomy; Pancreatic Neoplasms
The first reports on pancreatic cancer resections
were published after operations performed by Friedrich
Trendelenburg (Bonn) in 1882, Theodor Billroth (Wien)
in 1884, Alessandro Codivilla (Imola/Bologna) and
William S Halsted (Baltimore) in 1898, Walter Kausch
(Berlin) in 1912, Georg Hirschel (Heidelberg) in 1914, and
Alexander Brunschwig (Chicago) in 1937. Presumably, the
majority of these operations were performed for cancers
of the papilla of Vater rather than for exocrine pancreatic
cancer. It wasn’t until the publication by Allan Oldfather
Whipple (New York) with two co-workers in 1935 [1] and
subsequently his own article on “The rationale of radical
surgery for cancer of the pancreas and ampullary region”
in 1941 [2] that highlighted to surgical societies that
pancreatic head cancer was technically resectable.
During his time in surgery Dr. Whipple only performed
37 ”whipples”, which in today’s standards would classify
AO Whipple as a “low-volume Whipple surgeon” The
“Whipples” of today entail “resection of the pancreatic
head” and in fact have little resemblance to the Whipple’s
original operations from 1935 with only slightly more
resemblance to his later descriptions from 1941. Today,
there is no optimal way of performing a “Whipple” and
instead pancreatoduodenectomies may be performed in
many different ways [3]. There have been no indications
that one method is superior to another, and the optimum
method is likely the one which the surgeon is most
acquainted with.
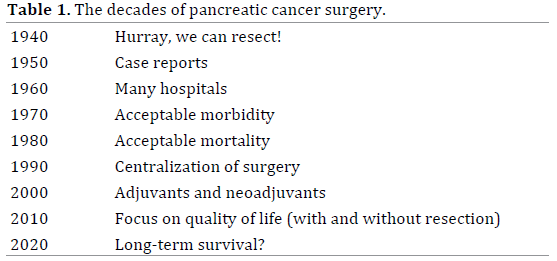
The results of the surgery have progressed through
several different stages since 1935 (Table 1), and the
results are nowadays quite good even outside the centres
of excellence in terms of the perioperative mortality [3, 4].
The long term results are still far from satisfying. Despite
progressively more patients undergoing pancreatectomy
for pancreatic adenocarcinoma – evaluated from 1992 to
2010 – with progressively smaller tumors and earlier stages
of disease the longterm results have not improved. While
it is true that patients lived longer (e.g. improved survival
curves and median survival) but despite this, did not have
an improved 5-year survival, denoting better early and
intermediate survival [4]. However, the number of patients
operated upon in 2010 – and even more so in 2018 – is far
larger than in 1992. Meaning that this is a comparison of
the fittest in 1992 with the fittest together combined with
the not so fit as well as those with more advanced disease
in 2010. Thus, the results are better from a population
point of view despite the dissatisfaction of the statisticians.
The improved result of surgery today is not due to one
or a few new surgical technical innovations. Rather it
is stepwise, gradual, and continuous progress based on
improvements in radiology, anesthesiology, intensive
care, oncology, nursing – and surgery. These disciplines
in turn have progressed because of laboriously research,
rather as a result of careful analysis of thelarge patient
outcomes registries than of few Nobel-prize winning
intellectuals. Our results of today stand on the shoulders
of our surgical forefathers! If this is true,it is likely that
today’s results will be overthrown by tomorrows, and
we will be able to say that our followers’ results are
based on our shoulders.
However, the young surgeons may not be satisfied
with the present surgical outcomes – a dissatisfaction that
sometimes may be shared with the generation that saw
one fourth of all patients “whippled” never leaving the
hospital alive when they started in surgery [5], and at their
retirement met a postoperative mortality of 0-3 percent.
At the turn of the last millennium the thought was that
centralization of surgery should have an important impact on survival after resection for pancreatic cancer
[6] – and while that was probably true – the benefits
from that had probably already been achieved in most
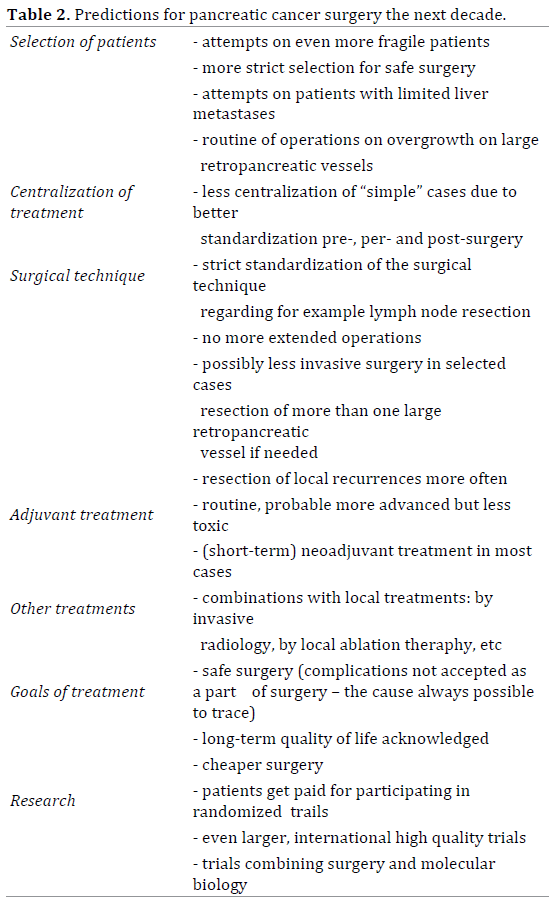
Western countries. There are likely other factors
that now are more important for future progress in
pancreatic cancer surgery (Table 2), and it must be
appreciated that it is not one outstanding thought that
will make the difference for the next set of patients with
pancreatic cancer, but instead it is a cluster of small
differences that together will ultimately increase longterm
postoperative and oncologic survival.
Conflict of Interest
For non of the three authors exists a conflict of interests.
References
- Whipple AO, Parsons WB, Mullins CR. Treatment of carcinoma of the
ampulla of Vater. Ann Surg 1935; 102:763-79. [PMID: 17856666]
- Whipple AO. The rationale of radical surgery for cancer of the pancreas
and ampullary region. Ann Surg 1941; 114:612-5. [PMID: 17857897]
- Kamarajah SK. Pancreaticoduodenectomy for periampullary tumours:
a review article based on Surveillance, End Results and Epidemiology
(SEER) database. Clin Transl Oncol 2018. [PMID: 29335829]
- Luberice K, Downs D, Sadowitz B, Ross S, Rosemurgy A. Has survival
improved following resection for pancreatic adenocarcinoma? Am J Surg
2017; 214:341-6. [PMID: 28601189]
- Andrén-Sandberg Å, Ihse I. Factors influencing survival after total
pancreatectomy in patients with pancreatic cancer. Ann Surg 1983;
198:605-10. [PMID: 6639161]
- Andrén-Sandberg Å, Neoptolemos JP. Resection for pancreatic cancer
in the new millennium. Pancreatology 2002; 2:431-9. [PMID: 12378110]

