Keywords
Pancreatic Neoplasms; Stem Cells; Survival
Abbreviations
ESA: epidermal surface antigen; OCT3/4: Organic cation transporter 3/4
What We Knew Before 2103 ASCO Annual Meeting
The identification of cancer stem cells from blood mononuclear cells in human acute myeloid leukemia (AML) in 1997 was a landmark discovery that led to our understanding about this subpopulation of cells. Two scintillating characteristics of these cancer stem cells include: 1) their ability for self-renewal; and 2) their capacity to differentiate into unlimited heterogeneous populations of cancer cells (Figure 1). These results suggest that cancer stem cells may represent a potential therapeutic target for the treatment as well as for prevention of tumor progression. Similarly, there is emerging evidence that certain subset of pancreatic cancer cells termed pancreatic cancer stem cells have ability to stay quiescent for long time, contribute to the tumor’s aggressiveness, invasion, metastasis and resistance to chemotherapeutic regimens and even radiation [1, 2]. Various cell markers had been identified as markers for pancreatic cancer stem cells including CD44, CD24 and epidermal surface antigen (ESA) [1], CD133 [3], CXCR4 [3], c-Met [4], high activity of aldehyde dehydrogenase 1 [5] and low activity 26S proteasome [6]. Unfortunately none of markers described as pancreatic cancer stem cell markers are specific to pancreatic adenocarcinoma and there is significant overlap with other cancer types and even with healthy cells. For this reason there is need to find new stem cell markers with the hope that one day we will have more specific marker or combination of markers.
Figure 1. The model of hierarchical organization of pancreatic
cancer cell population. The pancreatic cancer stem cells and their
progenies in differentiation can develop to single colonies with
different morphologies. Based on the in vivo and in vitro characteristics, holoclones correspond to the cancer stem/
progenitor cells, while paraclones correspond to the fully
differentiated cells and meroclones correspond to the cells in the
intermediate stage. The genes and microRNAs that associate with
cancer stem cells and support chemoresistance, including BMI1,
GLI1/2, CXCR4, mir-21/214/221/222/155, are enriched in
holoclones. However, the Let-7 and mir-30a/b/c are enriched in
paraclones. (Adapted from Tan et al., 2011 [26]. Open-access
article distributed under the terms of the Creative Commons
Attribution License, which permits unrestricted use, distribution,
and reproduction in any medium, provided the original author
and source are credited).
What We Learnt at 2103 ASCO Annual Meeting
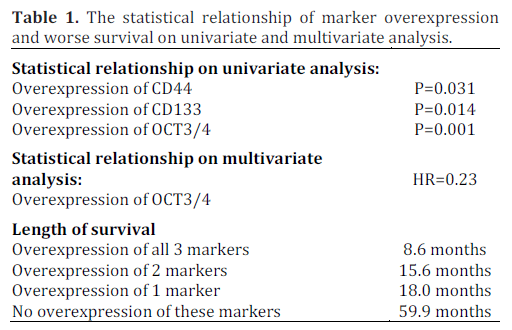
Andrikou et al. (Abstract #e15058) presented the results of a study investigating the relationship between pancreatic cancer stem cell markers and prognostic outcomes among pancreatic ductal adenocarcinoma patients [7]. They included 43 pancreatic cancer histology specimens in their study. All specimens were analyzed for common pancreatic cancer stem cell markers, i.e., CD24, CD44, CD133, CD166, organic cation transporter 3/4 (OCT3/4) and leucine-rich G protein-coupled receptor-5 (LGR5). Univariate analysis revealed patients with an overexpression of CD44, CD133, OCT3/4 had significantly worse prognosis for overall survival (P=0.031, P=0.014, and P=0.001, respectively). As shown in Table 1, similar results were achieved on multivariate analysis and OCT3/4 proved to be an independent factor predicting poor outcome (HR=0.23). Patients who overexpressed all factors had worse overall survival compared to patients expressing only two, one or none (8.6 vs. 15.6 vs. 18.0 vs. 59.9 months; P=0.006).
Discussion
Pancreatic adenocarcinoma has the worse prognosis among the cancers and is 4th leading of cancer related death [8]. Little has changed over last several years for 5-year survival despite introduction of new chemotherapeutic agents. It is primarily due to metastasis at an early stage of the disease as majority of the patients present at an unresectable stage and chemoresistance. Lately attention has been focused on genetic and stem cell levels to find better ways to treat this cancer and improve patient outcomes. Cancer stem cells like normal stem cells are characterized by ability to self-renew and differentiate into other cancer cell types. Additionally, the cancer stem cells can form xenograft tumors in immunodeficient mice and can survive exposure to chemotherapeutic agents in vitro. The presence of cancer stem cells in hematological malignancies like acute myelogenous leukemia and chronic myelogenous leukemia are well established [9, 10]. Molecular analysis of solid organ tumors like breast, prostate, colon, melanoma and glioblastoma has also revealed the presence of stem cells [11, 12, 13, 14, 15]. In case of pancreatic cancer, Li et al. demonstrated the CD44, CD24 and ESA cells to be the most tumorigenic [1]. It was noted that only 100 cells were enough to produce tumor in half of immunodeficient mice. These triple positive cells were able to achieve markers of parent tumors as well as to differentiate into cells which were triple negative, double positive or single positive (ability to differentiate into different lineage). Similarly the presence of CD133 was noted to have stem cell like properties in another study in 2007 [3]. CD133 cells were noted to have increased tumorigenicity compared to CD133 negative cells. It was also noted that CD133 cells were resistant to gemcitabine. CXCR4 is a receptor present on subset of CD133 cells with significantly increased potential to metastasize [3]. It is a receptor for stromal derived factor 1 (SDF1) and plays a role in spread of cancer locally/invasion and metastasis to distant sites. Spread of tumor was prevented by blocking CD133/CXCR4 cells in mice. In 2011 Li et al. reported c-Met as a marker for pancreatic stem cells [4]. c-Met positive cells readily formed in vitro spheres, which was not the case with c-Met negative cells. This sphere formation was inhibited by c-Met inhibitor XL184 or c-Met knockdown with small hairpin RNA. Similarly c-Met high cells were noted to have increased tumorigenicity in NOD SCID mice. It was noted that cells that expressed c-Met and CD44 combination had the highest tumorigenicity and ability to renew. High activity of aldehyde dehydrogenase 1 has also been associated with pancreatic cancer stem cells. Kim et al. reported the pancreatic cancer cells with high ALDH1 activity to be resistant to chemotherapy induced cell death and highly tumorigenic irrespective of CD133 status [5]. CD166 is known to upregulated in prostate cancer. Jiao et al. reported the presence of CD166 in prostate stem/progenitors and castration resistant sub-population of prostate cancer cells [16].
Muraro et al. reported a negative study for colon cancer in which presence of any of commonly reported stem cell markers like CD133 or coexpression with CD166/CD44 or CD44/CD24, did not appear to carry increased tumorigenicity in vivo or increased survival on exposing these cells to chemotherapeutic agents [17]. Similarly Tachezy et al. reported no association with clinical or histological data for pancreatic adenoma carcinoma patients, in contrast to a similar study by same group in which ACAM/CD166 expression was associated with metastasis and worse survival in patients with esophageal cancer [18, 19]. Organic cation transporter 3/4 (OCT3/4) is a transcription factor that regulates self renewal and pluripotency of embryonic stem cells and is a marker of plasticity especially in plastic states sensitive to environmental programming. Reactivity of OCT3/4 is reported to have a role in seminoma carcinomatosis [20, 21, 22]. Lately OCT3/4 had been reported as marker for extragonadal seminoma, embryonic carcinoma, breast and gonadoblastoma [23, 24, 25].
This study expands our knowledge of pancreatic cancer stem cell markers. So far available treatment options in pancreatic cancer, including chemotherapy, surgery and radiotherapy, have yielded poor results. Quite high proportions of patients relapse. This relapse seems to due to the presence of cancer cell population which has features of “stem cells” with ability to stay quiescent for relatively long time, have pluripotency so they can differentiate into various cancer cell lines, survive chemotherapy exposure and form tumors in nude mice. Next frontier for chemotherapy for pancreatic cancer patient could be chemo/immunotherapeutic options based on this understanding and by targeting these cells in addition to currently available chemotherapy option known to result in debulking of cancer, primarily by having cytotoxic effects against differentiated cancer cells. First step to devise such therapies would be to isolate stem cells with precision and define their markers with high specificity. Unfortunately none of the currently available markers of pancreatic cancer stem cells have proven to be specific. Multitude of new markers have confused the picture to extent that few authorities even doubt the presence of these specific “stem” cells in pancreatic cancer. Said that there is need for more research to know more markers with the aim of finding a marker which will be highly specific and sensitive for these cells which contribute to poor outcomes by causing disease to relapse, having a role in metastasis, chemoresistance and eventually to use it as a target for new novel therapies. Our reviewed abstract is such an addition to research on this important topic.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Li, C., et al., Identification of pancreatic cancer stem cells.Cancer Res, 2007. 67(3): p. 1030-7.
- Rasheed, Z.A., et al., Prognostic significance of tumorigeniccells with mesenchymal features in pancreatic adenocarcinoma. JNatl Cancer Inst, 2010. 102(5): p. 340-51.
- Hermann, P.C., et al., Distinct populations of cancer stem cellsdetermine tumor growth and metastatic activity in humanpancreatic cancer. Cell Stem Cell, 2007. 1(3): p. 313-23.
- Li, C., et al., c-Met is a marker of pancreatic cancer stem cellsand therapeutic target. Gastroenterology, 2011. 141(6): p. 2218-2227 e5.
- Kim, M.P., et al., ALDH activity selectively defines anenhanced tumor-initiating cell population relative to CD133expression in human pancreatic adenocarcinoma. PLoS One,2011. 6(6): p. e20636.
- Adikrisna, R., et al., Identification of pancreatic cancer stemcells and selective toxicity of chemotherapeutic agents.Gastroenterology, 2012. 143(1): p. 234-45 e7.
- Andrikou K, Faloppi L, Loretelli C, Mandolesi A, Bearzi I,Cascinu S. Expression of stem cell markers in pancreatic ductaladenocarcinoma and clinical relevance. J Clin Oncol 2013;31(Suppl.): Abstract #e15058.
- Jemal, A., et al., Cancer statistics, 2007. CA Cancer J Clin,2007. 57(1): p. 43-66.
- Bonnet, D. and J.E. Dick, Human acute myeloid leukemia isorganized as a hierarchy that originates from a primitivehematopoietic cell. Nat Med, 1997. 3(7): p. 730-7.
- Graham, S.M., et al., Primitive, quiescent, Philadelphiapositivestem cells from patients with chronic myeloid leukemiaare insensitive to STI571 in vitro. Blood, 2002. 99(1): p. 319-25.
- Al-Hajj, M., et al., Prospective identification of tumorigenicbreast cancer cells. Proc Natl Acad Sci U S A, 2003. 100(7): p.3983-8.
- Miki, J., et al., Identification of putative stem cell markers,CD133 and CXCR4, in hTERT-immortalized primarynonmalignant and malignant tumor-derived human prostateepithelial cell lines and in prostate cancer specimens. Cancer Res,2007. 67(7): p. 3153-61.
- O’Brien, C.A., et al., A human colon cancer cell capable ofinitiating tumour growth in immunodeficient mice. Nature, 2007.445(7123): p. 106-10.
- Frank, N.Y., et al., ABCB5-mediated doxorubicin transportand chemoresistance in human malignant melanoma. Cancer Res,2005. 65(10): p. 4320-33.
- Singh, S.K., et al., Identification of a cancer stem cell in humanbrain tumors. Cancer Res, 2003. 63(18): p. 5821-8.
- Jiao, J., et al., Identification of CD166 as a surface marker forenriching prostate stem/progenitor and cancer initiating cells.PLoS One, 2012. 7(8): p. e42564.
- Muraro, M.G., et al., CD133+, CD166+CD44+, andCD24+CD44+ phenotypes fail to reliably identify cell populationswith cancer stem cell functional features in established humancolorectal cancer cell lines. Stem Cells Transl Med, 2012. 1(8): p.592-603.
- Tachezy, M., et al., ALCAM (CD166) expression and serumlevels in pancreatic cancer. PLoS One, 2012. 7(6): p. e39018.
- Tachezy, M., et al., ALCAM (CD166) expression and serumlevels are markers for poor survival of esophageal cancerpatients. Int J Cancer, 2012. 131(2): p. 396-405.
- Honecker, F., et al., New insights into the pathology andmolecular biology of human germ cell tumors. World J Urol,2004. 22(1): p. 15-24.
- Jones, T.D., et al., OCT4: A sensitive and specific biomarkerfor intratubular germ cell neoplasia of the testis. Clin Cancer Res,2004. 10(24): p. 8544-7.
- de Jong, J., et al., Diagnostic value of OCT3/4 for pre-invasiveand invasive testicular germ cell tumours. J Pathol, 2005. 206(2):p. 242-9.
- Iczkowski, K.A., et al., Trials of new germ cellimmunohistochemical stains in 93 extragonadal and metastaticgerm cell tumors. Hum Pathol, 2008. 39(2): p. 275-81.
- Palma, I., et al., Utility of OCT3/4, TSPY and beta-catenin asbiological markers for gonadoblastoma formation and malignantgerm cell tumor development in dysgenetic gonads. Dis Markers,2013. 34(6): p. 419-24.
- Ling, G.Q., et al., Expression of the pluripotency markersOct3/4, Nanog and Sox2 in human breast cancer cell lines. OncolLett, 2012. 4(6): p. 1264-1268.
- Tan L, Sui X, Deng H, Ding M. Holoclone forming cells frompancreatic cancer cells enrich tumor initiating cells andrepresent a novel model for study of cancer stem cells. PLoS One2011; 6(8):e23383.


