Keywords
Heparin, Low-Molecular-Weight; Pancreatic Neoplasms; Thromboplastin; Thrombosis; Venous Thromboembolism
Abbreviations
ASCO: American Society of Clinical Oncology; CONKO: Charité Onkologie; LMWH: low-molecular weight heparin
Introduction
The association between thrombosis and cancer has been known for centuries. Although the exact incidence of venous thromboembolism in individual cancers has not been defined, there is evidence that the absolute risk depends on the tumor type, the extent of tumor burden, and treatment with chemotherapeutic agents. Idiopathic thrombosis can often be the first manifestation of an occult malignancy and based on a recent meta-analysis, the cancer-specific risk after idiopathic venous thromboembolism was highest in ovarian, pancreatic and hepatic cancers in descending order [1]. Pancreatic cancer has the highest risk of thrombotic events amongst any other gastrointestinal cancers and the incidence ranges from 17% to 57% [2]. The diagnosis of thromboembolism in pancreatic cancer patients is associated with an advanced stage of disease and poor overall survival [3, 4].
The pathogenesis of hypercoagulability in cancer is complex. There is an increased expression of prothrombotic factors [5, 6, 7] (tissue factor, thrombin and fibrinogen), decreased inhibitors of anticoagulation [7, 8] and an increase in platelet aggregation resulting from increased fibrinogen, thrombospondin I and mucin [9, 10]. Of prime importance is tissue factor protein, the initiator of coagulation, in noninvasive and invasive pancreatic neoplasia. In addition to clinical venous thromboembolism, it is also associated with vascular endothelium growth factor (VEGF) expression, and increased microvessel density [6]. However, tissue factor as a predictor of clinical outcomes has not been well studied.
Standard therapy for venous thromboembolism in cancer includes the use of low-molecular weight heparins (LMWH) followed by warfarin. Data from emerging prospective clinical trials support the use of LMWHs over warfarin by showing improved efficacy and outcomes [11, 12, 13, 14].
What We Learnt at ASCO 2010
Impact of Thromboembolism on Clinical Outcomes of Pancreatic Cancer
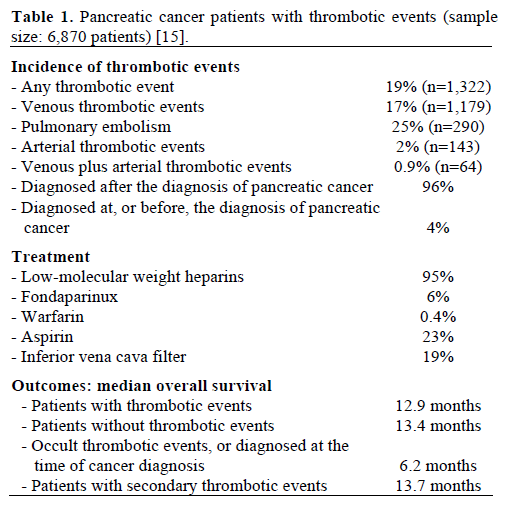
A retrospective, single institute study looked at 6,870 patients with pancreatic cancer treated from January 1st, 2000 to December 31st, 2009 [15]. The group evaluated these patients for venous as well as arterial thrombotic events. The overall incidence of thrombotic events was 19% in this group of patients, with a vast majority of patients experiencing venous thromboembolism (17%), compared to a smaller proportion of patients with arterial thrombotic events (2%) and combined venous thromboembolism plus arterial thrombotic events (0.9%). Of the patients with venous thromboembolism, 25% had a pulmonary embolism. Majority of the patients received LMWH for treatment (95%) and 19% of patients had an inferior vena cava filter placement.
The investigators report a worse overall survival for patients with a thrombotic event as compared to those without (12.9 months vs. 13.4 months). Also, thrombotic events diagnosed at, or before, the diagnosis of pancreatic cancer conferred a significantly poorer overall survival (6.2 months vs. 13.7 months). The data of this study are summarized in Table 1.
What Are the Predictors of Thromboembolism in Pancreatic Cancer and Do They Affect Outcomes?
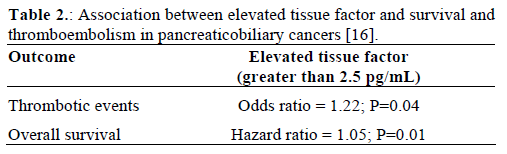
An elevated tissue factor has been reported in patients with multiple cancers, including pancreaticobiliary cancers, and its role in disease progression and outcomes in not well established. This study looks aims to correlate the elevation of tissue factor in pancreaticobiliary cancer patients with thrombotic events (arterial and venous) and survival.
Bharthuar et al. conducted a retrospective study collecting clinical information and plasma samples of available patients diagnosed with pancreaticobiliary cancers between January 2005 to December 2008 [16]. Clinical data was collected independently and tissue factor levels were analyzed with a pre-determined tissue factor microparticle-associated procoagulant activity (MP-PCA) assay. The study included 117 patients, of which 65 were females, 108 Caucasians, and the median age was 65 years. Pancreatic cancers comprised of 68% of the tumors; biliary cancers were 29%. Thrombotic events occurred in 52 (44.4%) patients. Mean and median tissue factor for all patients were 2.15 pg/mL and 1.20 pg/mL, respectively (range: 0.17-31.01 pg/mL). Elevated tissue factor levels was significantly associated with TE events (P=0.04), and an elevated tissue factor level was associated with a worse overall survival (hazard ratio, HR: 1.05; P=0.01). The data of this study are summarized in Table 2.
Is Treatment with LMWH Effective in Pancreatic Cancer Patients Undergoing Chemotherapy?
The final results of the Charité Onkologie (CONKO)- 004 trial were reported at the 2010 American Society of Clinical Oncology (ASCO) Annual Meeting. The primary objective of this randomized trial was to study the reduction in symptomatic venous thromboembolism in advanced pancreatic cancer patients treated with simultaneous LMWH and chemotherapy, with secondary objectives being time to progression and overall survival [17]. The expected reduction in symptomatic venous thromboembolism within the first three months of treatment was from 10% to 3%. From April 2004 to January 2009, 312 patients with histologically or cytologically confirmed advanced pancreatic cancer were randomized to receive or not to receive LMWH (1 mg/kg once a day for 3 months, followed by 40 mg daily). After randomization, 152 patients did not receive LMWH, and 160 patients were in the intervention arm. There was a significant decrease in the incidence of symptomatic venous thromboembolism in the treatment vs. no treatment arm after 3 months (1.25% vs. 9.87%, respectively) as well as after 12 months (5.00% vs. 15.13%, respectively).
There was no significant difference in major bleeding in both arms. The median follow up time was 45.44 months. There was no significant difference in median time to progression (5.03 months in the treatment arm vs. 5.42 months in no treatment arm; P=0.941) or median overall survival (7.92 months in treatment arm vs. 8.15 months in no treatment arm; P=0.054). The data of this study are summarized in Table 3.

Comments
The data from above mentioned studies further reinforce the inverse association of thromboembolism and pancreatic cancer outcomes. The sample size of the single institution study (Abstract #4062 [15]) is commendable. The incidence of venous thromboembolism in this single institutional study was 19% which is consistent with prior literature. It would have been worth stratifying patients with venous thromboembolism according to stage, treatment strategies (best supportive care vs. different chemotherapy regimens), and time elapsed between the development of venous thromboembolism and death. These results also bring up the question whether there is any role of prophylactic anticoagulation in patients diagnosed with pancreatic cancer especially those undergoing active treatment. This question is answered in the CONKO-004 trial [17] which showed that LMWHs can be safely and effectively used in the primary prevention of thrombotic events in advanced pancreatic cancer patients undergoing treatment with chemotherapy. However, this study did not show any improvement in the overall survival and time to progression. A previous non randomized trial did show an improvement in survival by the use of LMWH in conjunction with chemotherapy [12]. This needs to be validated in further prospective trials.
Tissue factor might be a valuable tool for risk assessment of venous thromboembolism development and needs to be investigated in a prospective trial as an independent predictor of disease progression and survival.
Conflict of interest The authors have no potential conflicts of interest
References
- Iodice S, Gandini S, Löhr M, Lowenfels AB, Maisonneuve P.
Venous thromboembolic events and organ-specific occult cancers: a
review and meta-analysis. J Thromb Haemost 2008; 6:781-8. [PMID
18284604]
- Khorana AA, Fine RL. Pancreatic cancer and thromboembolic
disease. Lancet Oncol 2004; 5:655-63. [PMID 15522652]
- Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of
venous thromboembolism and its effect on survival among patients
with common cancers. Arch Intern Med 2006; 166:458-64. [PMID
16505267]
- Mandalà M, Reni M, Cascinu S, Barni S, Floriani I, Cereda S, et
al. Venous thromboembolism predicts poor prognosis in irresectable
pancreatic cancer patients. Ann Oncol 2007; 18:1660-5. [PMID
17660490]
- Haas SL, Jesnowski R, Steiner M, Hummel F, Ringel J, Burstein
C, et al. Expression of tissue factor in pancreatic adenocarcinoma is
associated with activation of coagulation. World J Gastroenterol
2006; 12:4843-9. [PMID 16937466]
- Khorana AA, Ahrendt SA, Ryan CK, Francis CW, Hruban RH,
Hu YC, et al. Tissue factor expression, angiogenesis, and thrombosis
in pancreatic cancer. Clin Cancer Res 2007; 13:2870-5. [PMID
17504985]
- Lindahl AK, Odegaard OR, Sandset PM, Harbitz TB.
Coagulation inhibition and activation in pancreatic cancer. Changes
during progress of disease. Cancer 1992; 70:2067-72. [PMID
1394036]
- Wojtukiewicz MZ, Sierko E, Zimnoch L, Kozlowski L, Kisiel
W. Immunohistochemical localization of tissue factor pathway
inhibitor-2 in human tumor tissue. Thromb Haemost 2003; 90:140-6.
[PMID 12876637]
- Isenberg JS, Romeo MJ, Yu C, Yu CK, Nghiem K, Monsale J, et
al. Thrombospondin-1 stimulates platelet aggregation by blocking the
antithrombotic activity of nitric oxide/cGMP signaling. Blood 2008;
111:613-23. [PMID 17890448]
- Wahrenbrock M, Borsig L, Le D, Varki N, Varki A. Selectinmucin
interactions as a probable molecular explanation for the
association of Trousseau syndrome with mucinous adenocarcinomas.
J Clin Invest 2003; 112:853-62. [PMID 12975470]
- Lee AY, Levine MN, Baker RI, Bowden C, Kakkar AK, Prins
M, et al. Low-molecular-weight heparin versus a coumarin for the
prevention of recurrent venous thromboembolism in patients with
cancer. N Engl J Med 2003; 349:146-53. [PMID 12853587]
- Icli F, Akbulut H, Utkan G, Yalcin B, Dincol D, Isikdogan A, et
al. Low molecular weight heparin (LMWH) increases the efficacy of
cisplatinum plus gemcitabine combination in advanced pancreatic
cancer. J Surg Oncol 2007; 95:507-12. [PMID 17192920]
- Lee AY, Rickles FR, Julian JA, Gent M, Baker RI, Bowden C,
et al. Randomized comparison of low molecular weight heparin and
coumarin derivatives on the survival of patients with cancer and
venous thromboembolism. J Clin Oncol 2005; 23:2123-9. [PMID
15699480]
- Sohail MA, Saif MW. Role of anticoagulation in the
management of pancreatic cancer. JOP. J Pancreas (Online) 2009;
10:82-7. [PMID 19287098]
- Epstein AS, Crosbie C, Gardos S, Soff A, Shah MA, Kelsen DP,
O'Reilly EP. A single-institution (MSKCC) analysis of incidence and
clinical outcomes in patients with thromboembolic events and
exocrine pancreas cancer. J Clin Oncol 2010; 28(15 Suppl):4062.
- Bharthuar A, Khorana AA, Hutson A, Wang J, Mackman N, Iyer
RV. Association of elevated tissue factor (TF) with survival and
thromboembolism (TE) in pancreaticobiliary cancers (PBC). J Clin
Oncol 2010; 28(15 Suppl):4126.
- Riess H, Pelzer U, Opitz B, Stauch M, Reitzig P, Hahnfeld S, et
al. A prospective, randomized trial of simultaneous pancreatic cancer
treatment with enoxaparin and chemotherapy: Final results of the
CONKO-004 trial. J Clin Oncol 2010; 28(15 Suppl):4033.

