Muhammad Wasif Saif1, Susan Hotchkiss2, Marianne Brennan2, Kristin Kaley2
1Columbia University College of Physicians and Surgeons at New York Presbyterian Hospital.
New York, NY, USA. 2Yale University. New Haven, CT, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Columbia University; College of Physicians and Surgeons and the
Herbert Irving Cancer Center; 177 Fort Washington Avenue, Suite
6-435; New York, NY 10032; USA
Phone: +1-212.305.4954
Fax: +1-212.3050.3035
E-mail: mws2138@columbia.edu
Received November 12th, 2010 - Accepted November 15th, 2010
Keywords
Lymphatic Metastasis; Pancreatic Neoplasms; Positron-Emission Tomography; Tomography, Emission- Computed; Tomography, X-Ray Computed
Dear Sir,
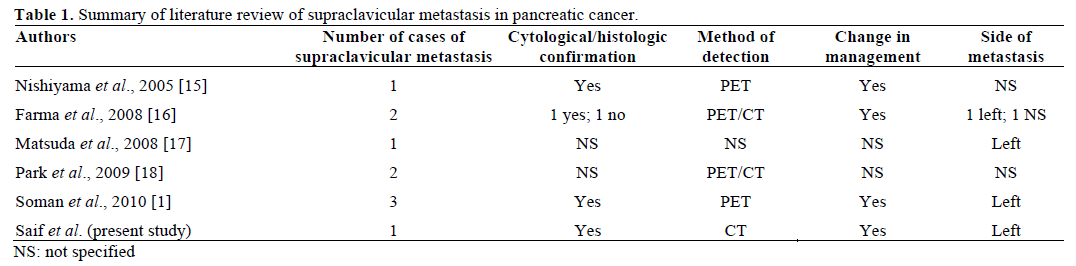
We read with interest the case series of isolated supraclavicular lymph node metastasis in pancreatic adenocarcinoma published in November 2010 edition of JOP. J Pancreas (Online) by Soman et al. [1].
Supraclavicular lymph nodes are a common site of metastases in breast cancer, lung cancer, gastroesophageal cancer and lymphoma [2]. Supraclavicular lymph node metastases in pancreatic cancer are uncommon. As mentioned by the authors, liver and peritoneal cavities are the most common sites, followed by lungs, bones and brain [1, 3]. Rare sites of metastases may involve kidney, adrenal gland, muscle, skin, heart, pleura, stomach, umbilicus, appendix, spermatic cord and prostate have also been reported in pancreatic cancer [4, 5, 6, 7, 8, 9, 10, 11, 12, 13].
We will like to present one more case of a patient with pancreatic cancer who developed metastasis in left supraclavicular lymph node metastasis. The previous cases and our case bring up the question: is this a Virchow’s node?
Our first patient was a 56-year-old Caucasian female with medical history of insulin dependent diabetes and hypothyroidism who was initially diagnosed with locally advanced pancreatic adenocarcinoma involving the celiac axis and superior mesenteric artery after being worked up for abdominal pain and weight loss. She received gemcitabine plus oxaliplatin (GemOx) chemotherapy regimen [14]. After 16 cycles (4 months), she developed a mass in the left supraclavicular area. A PET scan was requested but denied by the insurance. A CT scan was performed that confirmed an enlarged lymph node. Fine needle aspiration was performed and the pathology was consistent with her primary pancreatic adenocarcinoma. She received palliative external beam radiation therapy to the lymph node with improvement in pain. Two weeks after finishing the radiation therapy, her chemotherapy was changed to 5- flourouracil. Unfortunately, later she developed pulmonary metastases.
We have updated the Table 1 with our case, now totaling 10 cases of patients with pancreatic cancer who developed supraclavicular lymph node metastasis. We agree with authors that though supraclavicular lymph nodes represent an uncommon site of metastases, but carry clinical significance both in changing therapy and may be in prognosis; however, due to small number of cases, no clear association can be assessed at present PET/CT can provide valuable information in the detection and follow up of these patients [19]. This issue underscores its significance in patients where such imaging and awareness about uncommon sites can prevent a patient from unnecessary surgery, which also has economic impact.
Conflict of interest
The authors have no potential conflict of interest
References
- Soman AD, Collins JM, DePetris G, Decker GA, Silva A, Moss A, et al. Isolated supraclavicular lymph node metastasis in pancreatic adenocarcinoma: a report of three cases and review of the literature. JOP. J Pancreas (Online) 2010; 11:604-9. [PMID 21068495]
- Fultz PJ, Harrow AR, Elvey SP, Feins RH, Strang JG, Wandtke JC, et al. Sonographically guided biopsy of supraclavicular lymph nodes: a simple alternative to lung biopsy and other more invasive procedures. AJR Am J Roentgenol 2003; 180:1403-9. [PMID 12704059]
- Borad MJ, Saadati H, Lakshmipathy A, Campbell E, Hopper P, Jameson G, et al. Skeletal metastases in pancreatic cancer: a retrospective study and review of the literature. Yale J Biol Med 2009; 82:1-6. [PMID 19325940]
- Otegbayo JA, Oluwasola OA, Akere A, Yakubu A, Daramola OO, Ogun GO. Pancreatic carcinoma presenting as cutaneous nodules in a diabetic Nigerian male. West Afr J Med 2005; 24:180. [PMID 16092324]
- Takamori H, Kanemitsu K, Tsuji T, Kusano S, Chikamoto A, Okuma T, Iyama K. Metastatic gastric tumor secondary to pancreatic adenocarcinoma. J Gastroenterol 2005; 40:209-12. [PMID 15770407]
- Turiaf J, Battesti JP, Basset F, Degos JD. Metastatic pleurisy in pancreatic cancer with the presence of considerable quantities of amylase in the pleural effusion and a major paraneoplastic peripheral neurologic syndrome. Ann Med Interne (Paris) 1969; 120:449-58. [PMID 4309013]
- Crescentini F, Deutsch F, Sobrado CW, Araújo S. Umbilical mass as the sole presenting symptom of pancreatic cancer: a case report. Rev Hosp Clin Fac Med Sao Paulo 2004; 59:198-202. [PMID 15361985]
- Martino L, Martino F, Coluccio A, Mangiarini MG, Chioda C. Renal metastases from pancreatic adenocarcinoma. Arch Ital Urol Androl 2004; 76:37-9. [PMID 15185821]
- Filik L, Ozdal-Kuran S, Cicek B, Zengin N, Ozyilkan O, Sahin B. Appendicular metastases from pancreatic adenocarcinoma. Int J Gastrointest Cancer 2003; 34:55-8. [PMID 15235136]
- Bandyopadhyay D, Kapadia CR, Da Costa PE. Pancreatic carcinoma: report of two cases presenting with unusual metastases. Indian J Gastroenterol 2005; 24:75-6. [PMID 15879657]
- Merseburger AS, Muller CC, Merseburger Schonborn CT, Ostertag H, Kuczyk MA. A rare case of isolated prostate metastasis from primary pancreatic cancer. Urologe A 2005; 44:527-9. [PMID 15739061]
- Wafflart E, Gibaud H, Lerat F, de Kersaint-Gilly A, Leborgne J. Muscular metastasis of cancer of the pancreas. A propos of a case. J Chir (Paris) 1996; 133:167-70. [PMID 8761070]
- Robinson BW, Lewis RR. Myocardial metastasis from carcinoma of pancreas presenting as acute myocardial infarction. J R Soc Med 1982; 75:560-2. [PMID 7086811]
- Li J, Merl M, Lee MX, Kaley K, Saif MW. Safety and efficacy of single-day GemOx regimen in patients with pancreatobiliary cancer: a single institution experience. Expert Opin Drug Saf 2010; 9:207-13. [PMID 20095915]
- Nishiyama Y, Yamamoto Y, Yokoe K, Monden T, Sasakawa Y, Tsutsui K, et al. Contribution of whole body FDG-PET to the detection of distant metastasis in pancreatic cancer. Ann Nucl Med 2005; 19:491-7. [PMID 16248386]
- Farma JM, Santillan AA, Melis M, Walters J, Belinc D, Chen DT, et al. PET/CT fusion scan enhances CT staging in patients with pancreatic neoplasms. Ann Surg Oncol 2008; 15:2465-71. [PMID 18551347]
- Matsuda M, Watanabe G, Hashimoto M. A case of salvage chemotherapy with gemcitabine hydrochloride and nedaplatin for gemcitabine-refractory pancreatic cancer. Gan To Kagaku Ryoho 2008; 35:137-9. [PMID 18195544]
- Park SS, Lee KT, Lee KH, Lee JK, Kim SH, Choi JY, Rhee JC. Diagnostic usefulness of PET/CT for pancreatic malignancy. Korean J Gastroenterol 2009; 54:235-42. [PMID 19844143]
- Saif MW, Tzannou I, Makrilia N, Syrigos K. Role and cost effectiveness of PET/CT in management of patients with cancer. Yale J Biol Med 2010; 83:53-65. [PMID 20589185]

