Keywords
Chronic Pancreatitis, Alcoholic;
Pancreatectomy; Pancreaticoduodenectomy;
Pancreatic Neoplasms; Quality of Life
Abbreviations
EORTC QLQ-C30: European
Organisation for Research and Treatment of
Cancer-Quality of Life Questionnaire; FACTP:
Functional Assessment of Cancer Therapy-
Pancreas; GIQLI: Gastrointestinal Quality of
Life Index; QoL: quality of life; SF-36:
medical outcome study 36-Item Short-Form
Health Survey; WHO: World Health
Organization
Introduction
The World Health Organization (WHO) has
defined the quality of life (QoL) as: "… an
individual's perception of their position in life
in the context of the culture and value system
in which they live and in relation to their
goals, expectations, standards and concerns. It
is a broad-ranging concept affected in a
complex way by the person's physical health,
psychological state, level of independence,
social relationships, and their relationship to salient features of their environment." [1].
This is a general definition because QoL,
subjectively perceived by the patient, is
becoming a major issue in the evaluation of
any therapeutic intervention, mainly in
patients with chronic or hard to cure diseases
where the aim of the intervention is to keep
patients either symptom-free and able to live
in the community for a long time, or to reduce
the discomfort caused by the disease. Even if
chronic pancreatitis and pancreatic cancer are
chronic and hard-to-cure diseases, the
suggestion of WHO has been applied by
clinical researchers only recently. In fact,
together with the traditional evaluation of
morbidity and mortality, and the assessment
of exocrine and endocrine functions in
patients with pancreatic disease, we should
consider the perception of the health status of
patients with benign [2, 3, 4] or malignant
pancreatic diseases as a priority. If this is true
for chronic disease treated medically, QoL
becomes of particular interest in those
patients who undergo surgical procedures for
their pancreatic disease.
It is well-known that patients who undergo
pancreatic surgery may develop several postprocedural
complications mainly represented
by diabetes and maldigestion which may
affect their way of life [5].
The aim of this paper was to review the data
existing in the English literature on the QoL
in patients who undergo surgical resection of
the head of or the entire pancreatic gland
either for benign or for malignant diseases of
the pancreatic gland.
Methods
A search was made on June 20th, 2006 using
three different data bases (MEDLINE, Web of
Science and ScienceDirect) in order to select
the data existing in the literature on QoL and
pancreatic resection surgery published in full
text only. Controlled terms only were
searched: the Medical Subject Headings
(MeSH) terms for MEDLINE, the Topic
terms (TS) for Web of Science (WoS) and the
Keywords for ScienceDirect. Seventy-four
papers on MEDLINE, 122 on WoS, and 4 on
ScienceDirect were found (Tables 1, 2, 3). In
addition, one more article was identified in
the reference data received in the same timeperiod
from an e-mail alerting provider. Forty
duplicate papers were found among the
various databases; 37 of these were present in
MEDLINE and WoS while, regarding the
four papers found in the ScienceDirect
database, two were present at same time in MEDLINE and one was present at same time
in WoS. The fourth paper of the
ScienceDirect database was in abstract form
and was not included in the present study.
One-hundred and sixty papers were found [6, 7, 8, 9,10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109,110, 111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148, 149, 150, 151, 152, 153, 154, 155, 156, 157, 158, 159, 160, 161, 162, 163, 164, 165]
(Figure 1). Of these, 35 papers were excluded
because they were review articles [6, 7, 8, 9,10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40] and two were
letters to the editor not reporting original data
[41, 42]. The remaining 123 original papers
were considered for the purpose of this study.
Of these 123 original papers, 11 were
excluded because they reported data on nonpancreatic
diseases (gastric cancer, cancer of
the gallbladder, cancer of the common bile
duct, caustic disease) [43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53]. Therefore, 112 studies satisfied the aim of our study; however, 27
papers described studies not utilizing any
QoL questionnaire [54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80] and 37 papers
reported data collected using non-validated
QoL questionnaires [81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109,110, 111, 112, 113, 114, 115, 116, 117]. Thirty-five of the 48 remaining studies
were not considered: 19 considered surgical procedures of pancreaticoduodenectomy or
total pancreatectomy without distinction
among chronic pancreatitis, pancreatic
neoplasms, neoplasms of the papilla of Vater,
or biliary tree neoplasms [118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136]; seven papers
reported non resective surgery or resective
surgery of the tail of the pancreas [137, 138, 139, 140, 141, 142, 143]; seven papers
reported data referring only to medical
treatment of unresected patients [144, 145, 146, 147, 148, 149, 150]; finally, two papers
[151, 152] did not distinguished among the
various types of surgery. Therefore, only 13
papers were evaluated for the purpose of this
study [153, 154, 155, 156, 157, 158, 159, 160, 161, 162, 163, 164, 165]; seven of these
papers were present at the same time in two
databases (MEDLINE and WoS) [153, 154, 155, 156, 157, 158, 159], two studies were
present in the MEDLINE database only [160, 161], three in the WoS database only [162, 163, 164], and the remaining one was the one
we received from an alerting e-mail [165].
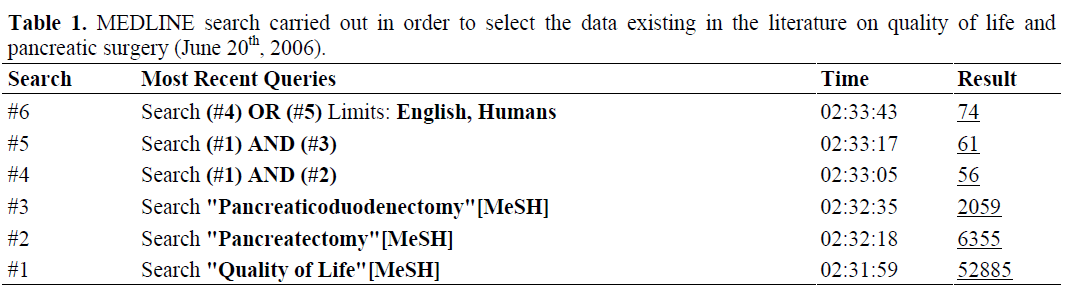
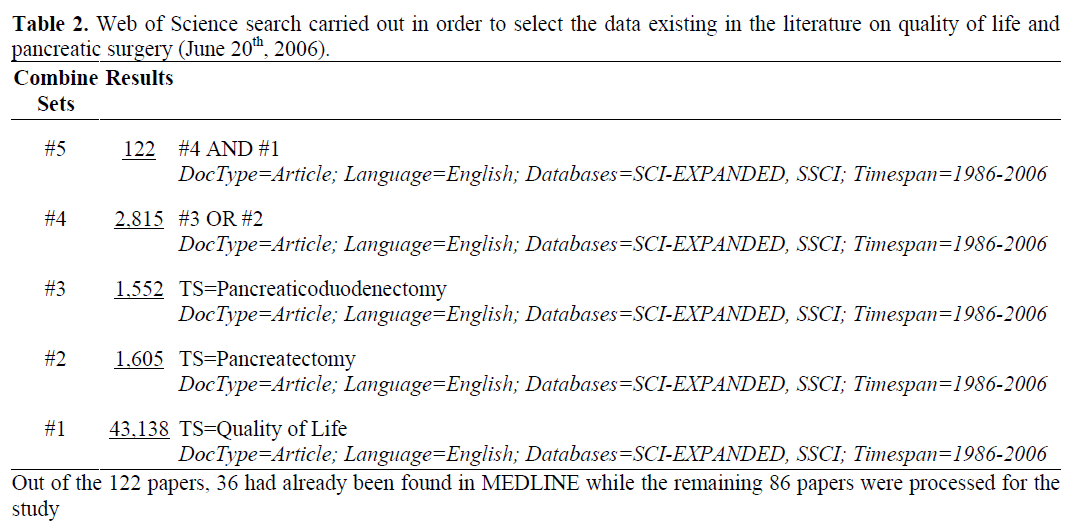
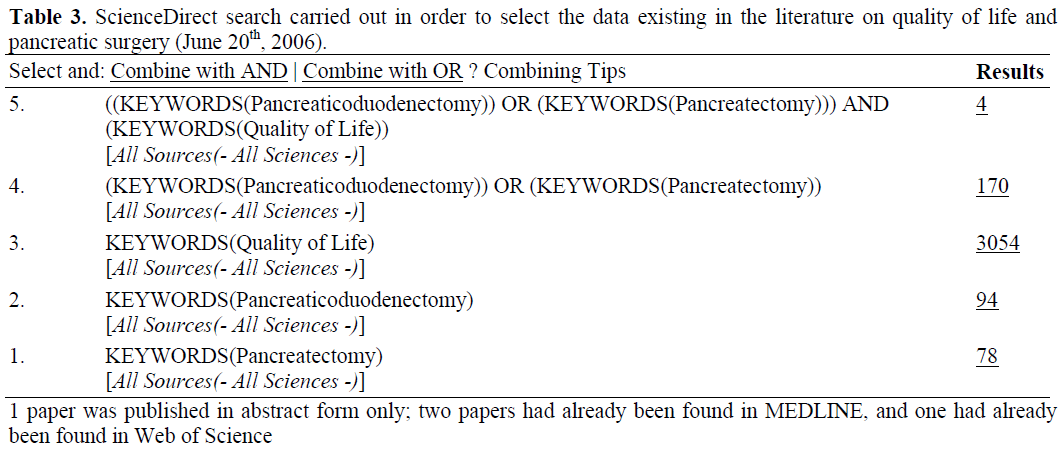
Figure 1. Flowchart showing the selection of papers evaluating the quality of life (QoL) in patients with surgical
resection of the head or whole pancreatic gland either for benign or for malignant pancreatic diseases (June 20th, 2006).
Results
Of the 13 studies considered, two focused
their interest on assessing the QoL as related
to surgical procedures involving pancreatic
neoplasms [160, 165] and 11 concerned
surgical procedures in chronic pancreatitis
patients [153, 154, 155, 156, 157, 158, 159, 161, 162, 163, 164].
Pancreatic Neoplasm
It is well-known that the QoL is worsen in
patients with pancreatic cancer [166, 167], but
an objective measure of the well-being in
patients operated on for a pancreatic
neoplasm is lacking. The only two studies
performed on patients with pancreatic cancer
are those of Farnell et al. [160] and
Schniewind et al. [165]. Farnell et al. [160]
utilized the Functional Assessment of Cancer
Therapy-Pancreas (FACT-P) questionnaire
which is made up of 37 items; the
questionnaire was self-administered in 35 patients in order to investigate their quality of
life before and four months after pancreatic
resection. Ten patients underwent a Whipple
procedure and 25 a Whipple procedure and
extended lymph node excision. The authors
did not find any difference in the QoL
assessment between the two types of surgery.
The study of Schniewind et al. [165] added
some more information to the previous study
of Farnell et al. [160]. These authors studied
91 patients resected for pancreatic
adenocarcinoma before surgery, at discharge,
and 3, 6, 12 and 24 months after the
operation; the EORTC QLQ-C30
questionnaire was used for the study. At the
time of discharge from the hospital, all
functional scores had dropped below baseline.
At 3 and 6 months after surgery, the scores
were comparable to preoperative values. After
12 and 24 months, patients reported a slightly
better QoL than before surgery. The only
exception was in the scale role functioning,
which improved at 24 months when compared
to the value at discharge but did not reach the
preoperative level. With patients who had R0
resection, similar outcomes were found in the
EORTC QLQ-C30 functional scales between
partial pancreaticoduodenectomy and pylorus
preserving pancreaticoduodenectomy, even if
patients who had pylorus preserving
pancreaticoduodenectomy reported
significantly more pain at 24 months after
surgery. Moreover, patients who had an
extended lymphadenectomy reported better
QoL on the EORTC QLQ-C30 functional
scales, but the symptom scales were worse in
comparison to the patients who underwent a
regional lymphadenectomy.
Chronic Pancreatitis
The questionnaires utilized by the various
authors who assessed the QoL following
surgical procedures in chronic pancreatitis
patients are reported in Table 4. The
questionnaires utilized were five: the SF-36,
the EORTC QLQ-C30, the visual analog
quality of life questionnaire, the
Gastrointestinal Quality of Life Index
(GIQLI), and the McGill Pain Questionnaire.
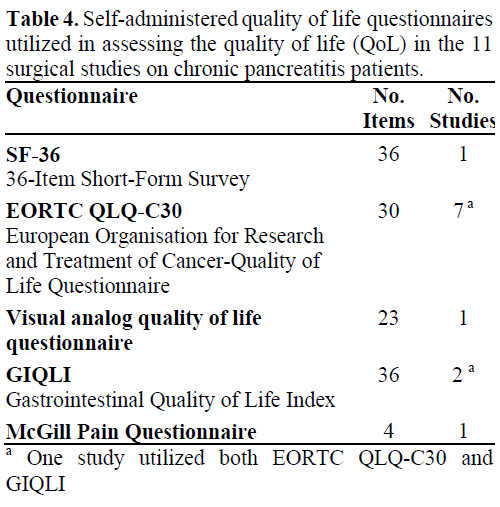
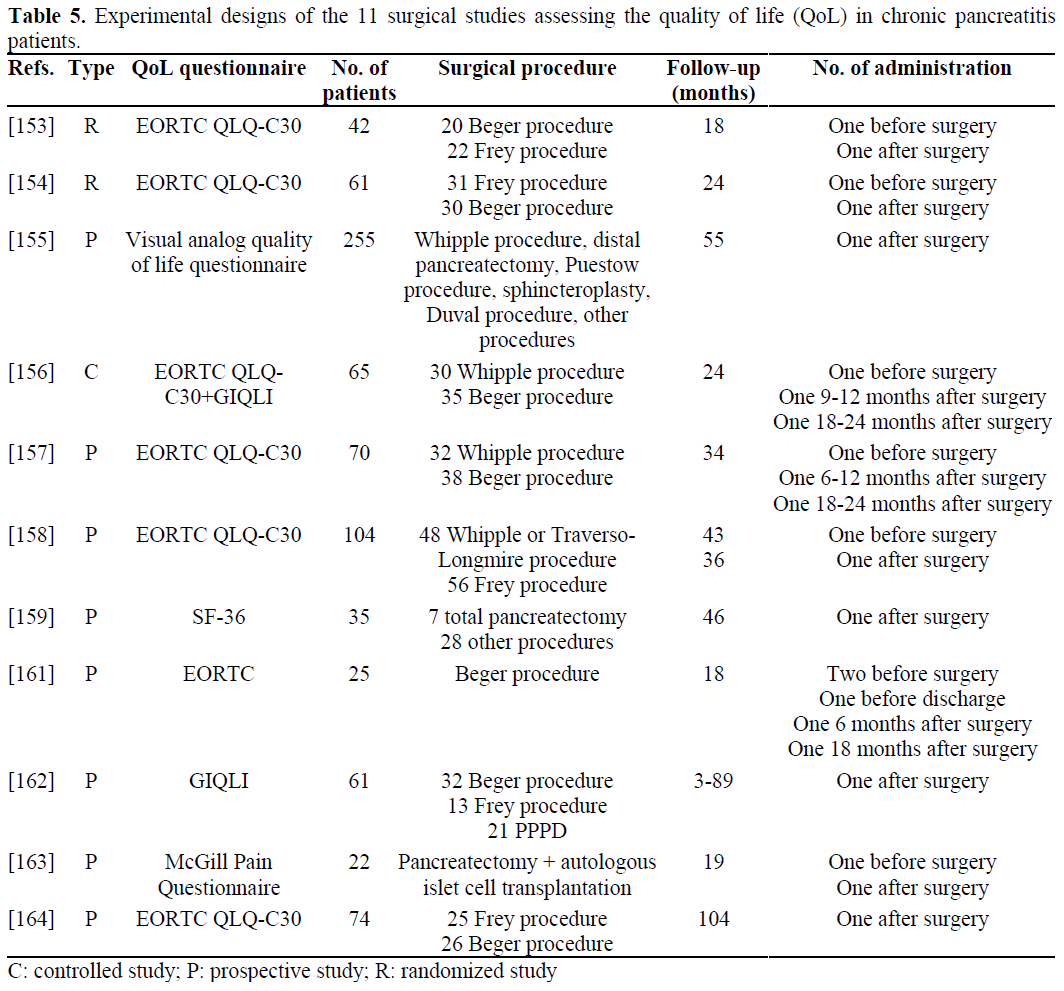
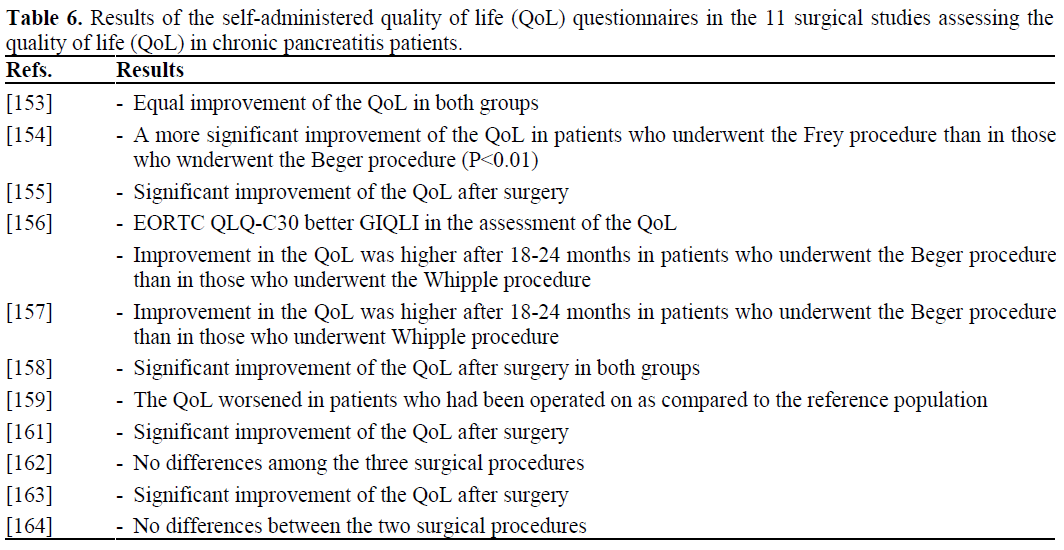
Table 5 shows the experimental designs of
these 11 surgical studies and the respective
results are reported in Table 6. At present,
there are no comparative studies assessing the
possibility that the various questionnaires
utilized explored the same physical and
mental domains. Furthermore, except for one
study demonstrating that the QoL in surgical
patients is worse as compared to a reference
population [159], in the other studies [153, 154, 155, 156, 157, 158, 159, 161, 162, 163, 164],
the authors aimed to demonstrate the
superiority of one type of operation with
respect to another, or to demonstrate that
surgery is capable of improving the QoL as
compared to the status evaluated prior to the surgery. The follow-up period for assessing
QoL in these studies had a median of 37
months (range 18-104 months) and this timeinterval
is probably too short to measure the
impact of surgery on well-being over a longterm
period. It is also difficult to compare
QoL results between the various studies
because of the differences in methodology,
study design and patient characteristics. In
this respect, more information comes from
studies which evaluated mixed medicalsurgical
populations of chronic pancreatitis
patients with a long follow-up period; in these
papers, patients who underwent various
surgical procedures for chronic pancreatitis
had a QoL similar to patients treated
medically [4, 151, 152]. It is probably true
that surgical procedures are able to briefly
ameliorate the QoL of surgically treated
patients but, thereafter, chronic pancreatitis per se tends to affect the well-being of these
patients.
Conclusions
Presently, there are very few studies exploring
the QoL in patients who undergo resection of
the head of the pancreas or total
pancreatectomy for benign and especially for
malignant disease of the pancreas.
Furthermore, more knowledge is necessary regarding the comparative behavior of the
QoL between patients operated on for benign
and for malignant pancreatic diseases; finally,
there is a need for studies which compare the
QoL of patients who have been operated on
with the well-being of a reference population.
In the meantime, the routinely assessment of
QoL in operated patients is recommended
both for patients affected by chronic
pancreatitis and for those with pancreatic
carcinoma in order to plan intensive medical
and psychological support.
Conflict of interest The authors have no
potential conflicts of interest
References
- World Health Organization, Division of Mental
Health. WHOQOL Measuring Quality of Life. The
World Health Organization quality of life instruments
(WHO/MSA/MNH/PSF/97.4). Geneva, Switzerland,
1997.
- Wehler M, Reulbach U, Nichterlein R, Lange K,
Fischer B, Farnbacher M, et al. Health-related quality
of life in chronic pancreatitis: a psychometric
assessment. Scand J Gastroenterol 2003; 38:1083-9.
[PMID 14621285]
- Pezzilli R, Morselli Labate AM, Ceciliato R,
Frulloni L, Cavestro GM, Comparato G, et al. Quality
of life in patients with chronic pancreatitis. Dig Liver
Dis 2005; 37:181-9. [PMID 15888283]
- Pezzilli R, Morselli-Labate AM, Frulloni L,
Cavestro GM, Ferri B, Comparato G, et al. The quality
of life in patients with chronic pancreatitis evaluated
using the SF-12 questionnaire: a comparative study
with the SF-36 questionnaire. Dig Liver Dis 2006;
38:109-15. [PMID 16243011]
- Pezzilli R. Diabetic control after total
pancreatectomy. Dig Liver Dis 2006; 38:420-2. [PMID
16569522]
- Kimura W, Han I, Furukawa Y, Sunami E,
Futakawa N, Inoue T, et al. Appleby operation for
carcinoma of the body and tail of the pancreas.
Hepatogastroenterology 1997; 44:387-93. [PMID
9164507]
- Obertop H, Pedrazzoli S. Current views on
surgical treatment of pancreatic cancer. Dig Surg 1999;
16:263-4. [PMID 10847759]
- McLeod RS. Quality of life, nutritional status and
gastrointestinal hormone profile following the Whipple
procedure. Ann Oncol 1999; 10(Suppl 4):281-4.
[PMID 10436841]
- Izbicki JR, Bloechle C, Knoefel WT, Rogiers X,
Kuechler T. Surgical treatment of chronic pancreatitis
and quality of life after operation. Surg Clin North Am
1999; 79:913-44. [PMID 10470335]
- Gouma DJ, Nieveen van Dijkum EJ, van Geenen
RC, van Gulik TM, Obertop H. Are there indications
for palliative resection in pancreatic cancer? World J
Surg 1999; 23:954-9. [PMID 10449827]
- Nolan MT, Johnson C, Coleman J, Patterson S,
Dang D. Unifying organizational approaches to
measuring and managing patient outcomes. J Nurs
Adm 2000; 30:27-33. [PMID 10650433]
- Matsuno S, Egawa S, Arai K. Trends in treatment
for pancreatic cancer. J Hepatobiliary Pancreat Surg
2001; 8:544-8. [PMID 11956906]
- Izbicki JR, Bloechle C. Essentials in surgery for
chronic pancreatitis. Dig Surg 2001; 18:147-8. [PMID
11351162]
- Stanford P. Surgical approaches to pancreatic
cancer. Nurs Clin North Am 2001; 36:567-77. [PMID
11532670]
- Ogata Y, Hishinuma S. The impact of pyloruspreserving
pancreatoduodenectomy on surgical
treatment for cancer of the pancreatic head. J
Hepatobiliary Pancreat Surg 2002; 9:223-32. [PMID
12140611]
- Duffy JP, Reber HA. Surgical treatment of chronic
pancreatitis. J Hepatobiliary Pancreat Surg 2002;
9:659-68. [PMID 12658398]
- Morrison CP, Wemyss-Holden SA, Partensky C,
Maddern GJ. Surgical management of intractable pain
in chronic pancreatitis: past and present. J
Hepatobiliary Pancreat Surg 2002; 9:675-82. [PMID
12658400]
- Schafer M, Mullhaupt B, Clavien PA. Evidencebased
pancreatic head resection for pancreatic cancer
and chronic pancreatitis. Ann Surg 2002; 236:137-48.
[PMID 12170018]
- Russell RC, Theis BA. Pancreatoduodenectomy in
the treatment of chronic pancreatitis. World J Surg
2003; 27:1203-10. [PMID 14534820]
- Niedergethmann M, Farag Soliman M, Post S.
Postoperative complications of pancreatic cancer
surgery. Minerva Chir 2004; 59:175-83. [PMID
15238891]
- Croce E, Olmi S, Bertolini A, Magnone S.
Laparoscopic surgery of pancreatic cancer: state of the
art. Hepatogastroenterology 2005; 52:1889-94. [PMID
16334801]
- Takada T. Surgery for carcinoma of the pancreas
in Japan. Past, present, and future aspects. Digestion
1999; 60(Suppl 1):114-9. [PMID 10026444]
- Roukos DH. Current advances and changes in
treatment strategy may improve survival and quality of
life in patients with potentially curable gastric cancer.
Ann Surg Oncol 1999; 6:46-56. [PMID 10030415]
- Huguier M, Mason NP. Treatment of cancer of the
exocrine pancreas. Am J Surg 1999; 177:257-65.
[PMID 10219866]
- Renou C, Laugier R. Postoperative pain therapy
following operation for chronic pancreatitis.
Pancreatology 2001; 1(Suppl 1):35-40.
- Spanknebel K, Conlon KC. Advances in the
surgical management of pancreatic cancer. Cancer J
2001; 7:312-23. [PMID 11561607]
- Tsiotou AG, Sakorafas GH. Pathophysiology of
pain in chronic pancreatitis: clinical implications from
a surgical perspective. Int Surg 2000; 85:291-6. [PMID
11589594]
- Magee CJ, Shekouh A, Ghaneh P, Neoptolemos
JP. Update on pancreatic cancer. Hosp Med 2002;
63:200-6. [PMID 11995268]
- Yamaguchi K, Noshiro H, Yokohata K, Nakano K,
Watanabe M, Ohtani K, et al. Is there any benefit of
preservation of the spleen in distal pancreatectomy? Int
Surg 2001; 86:162-8. [PMID 11996073]
- Ahrendt SA, Pitt HA. Surgical management of
pancreatic cancer. Oncology (Williston Park) 2002;
16:725-34. [PMID 12088296]
- Fujino Y, Suzuki Y, Ajiki T, Tanioka Y, Ku Y,
Kuroda Y. Predicting factors for survival of patients
with unresectable pancreatic cancer: a management
guideline. Hepatogastroenterology 2003; 50:250-3.
[PMID 12630033]
- Chu QD, Khushalani N, Javle MM, Douglass HO
Jr, Gibbs JF. Should adjuvant therapy remain the
standard of care for patients with resected
adenocarcinoma of the pancreas? Ann Surg Oncol
2003; 10:539-45. [PMID 12794020]
- Frey CF, Mayer KL. Comparison of local
resection of the head of the pancreas combined with
longitudinal pancreaticojejunostomy (frey procedure)
and duodenum-preserving resection of the pancreatic
head (beger procedure). World J Surg 2003; 27:1217-
30. [PMID 14534821]
- Sakorafas GH, Anagnostopoulos G. Surgical
management of chronic pancreatitis: current concepts
and future perspectives. Int Surg 2003; 88:211-8.
[PMID 14717527]
- Smeenk HG, Tran TC, Erdmann J, van Eijck CH,
Jeekel J. Survival after surgical management of
pancreatic adenocarcinoma: does curative and radical
surgery truly exist? Langenbecks Arch Surg 2005;
390:94-103. [PMID 15578211]
- Andren-Sandberg A, Backman PL, Andersson R.
Results of adjuvant therapy in resected pancreatic cancer. Int J Pancreatol 1997; 21:31-8. [PMID
9127171]
- Strasberg SM, Drebin JA, Soper NJ. Evolution and
current status of the Whipple procedure: an update for
gastroenterologists. Gastroenterology 1997; 113:983-
94. [PMID 9287993]
- Sporn JR. Practical recommendations for the
management of adenocarcinoma of the pancreas. Drugs
1999; 57:69-79. [PMID 9951952]
- Guraya SY, Murshid KR. Malignant duodenocolic
fistula. Various therapeutic surgical modalities. Saudi
Med J 2004; 25:1111-4. [PMID 15322610]
- Shrikhande SV, Kleeff J, Friess H, Buchler MW.
Management of pain in small duct chronic pancreatitis.
J Gastrointest Surg 2006; 10:227-33. [PMID
16455455]
- Sarr MG, Farnell MB. Re: Ouchi et al., A
palliative pancreaticoduodenectomy. World J Surg
1999; 23:218-9. [PMID 9880436]
- Krouse RS, Chu DZ, Grant M, Ferrell B, Wagman
LD. Evaluation of quality of life (QOL) in
pancreaticoduodenectomy survivors. Ann Surg 2002;
235:310-1. [PMID 11807377]
- Nakamura S, Nishiyama R, Yokoi Y, Serizawa A,
Nishiwaki Y, Konno H, et al. Hepatopancreatoduodenectomy
for advanced gallbladder carcinoma.
Arch Surg 1994; 129:625-9. [PMID 7515618]
- Ercolani G, Nagino M, Sano T, Kamiya J, Kondo
S, Kanai M, et al. Advanced adenosquamous
carcinoma of the gallbladder with bilio-biliary fistula:
an uncommon case treated by hepatopancreatoduodenectomy.
Hepatogastroenterology 1999;
46:1650-4. [PMID 10430314]
- Nakamura S, Suzuki S, Konno H, Baba S, Baba S.
Outcome of extensive surgery for TNM stage IV
carcinoma of the gallbladder. Hepatogastroenterology
1999; 46:2138-43. [PMID 10521956]
- Pack DA, O'Connor K, O'Hagan K.
Cholangiocarcinoma: a nursing perspective. Clin J
Oncol Nurs 2001; 5:141-6. [PMID 12690613]
- Ichikura T, Tomimatsu S, Okusa Y, Mochizuki H.
Improved physical condition by limiting
lymphadenectomy around the coeliac artery after distal
gastrectomy for gastric cancer. Eur J Surg 1999;
165:123-32. [PMID 10192569]
- Landen S, Wu MH, Jeng LB, Delugeau V, Launois
B. Pancreaticoduodenal necrosis due to caustic burns.
Acta Chir Belg 2000; 100:205-9. [PMID 11143322]
- Morpurgo E, Vitale GC, Galandiuk S, Kimberling
J, Ziegler C, Polk HC Jr. Clinical characteristics of
familial adenomatous polyposis and management of
duodenal adenomas. J Gastrointest Surg 2004; 8:559-
64. [PMID 15239991]
- Gockel I, Pietzka S, Gonner U, Hommel G,
Junginger T. Subtotal or total gastrectomy for gastric
cancer: impact of the surgical procedure on morbidity
and prognosis. Analysis of a 10-year experience.
Langenbecks Arch Surg 2005; 390:148-55. [PMID
15711817]
- Kaminishi M, Shimoyama S, Yamaguchi H,
Yamada H, Ogawa T, Kawahara M, et al. Results of
subtotal gastrectomy with complete dissection of the
N2 lymph nodes preserving the spleen and pancreas in
surgery for gastric cancer. Hepatogastroenterology
1994; 41:384-7. [PMID 7959577]
- Hatanaka N, Miyata M, Kamiike W, Okumura K,
Hashimoto T, Yamaguchi T, et al. Radical resection of
primary malignant melanoma of the gallbladder with
multiple metastases: report of a case. Surg Today 1993;
23:1023-6. [PMID 8292857]
- Sung JP, Stewart RD, O'Hara VS, Westhpal KF,
Wilkinson JE, Hill J. A study of forty-nine consecutive
Whipple resections for periampullary adenocarcinoma.
Am J Surg 1997; 174:6-10. [PMID 9240943]
- Evans DB, Abbruzzese JL, Lee JE, Leach SD,
Charnsangavej C Cleary KR, et al. Preoperative
chemoradiation for adenocarcinoma of the pancreas.
MD Anderson experience. Semin Surg Oncol 1995;
11:132-40.
- Taschieri AM, Elli M, Rovati M, Sampietro GM,
Cristaldi M, Danelli P, Pisacreta M. Surgical treatment
of pancreatic tumors invading the spleno-mesentericportal
vessels. An Italian Multicenter Survey. Hepatogastroenterology
1999; 46:492-7. [PMID 10228849]
- Henne-Bruns D, Vogel I, Luttges J, Kloppel G,
Kremer B. Surgery for ductal adenocarcinoma of the
pancreatic head: staging, complications, and survival
after regional versus extended lymphadenectomy.
World J Surg 2000; 24:595-601. [PMID 10787083]
- Sakorafas GH, Farnell MB, Nagorney DM, Sarr
MG, Rowland CM. Pancreatoduodenectomy for
chronic pancreatitis: long-term results in 105 patients.
Arch Surg 2000; 135:517-23. [PMID 10807274]
- Siech M, Mattfeldt T, Schlosser W, Beger HG.
Duodenum-preserving pancreatic head resection in
patients with benign and borderline tumors of the
pancreatic head. Langenbecks Arch Surg 2000;
385:229-33. [PMID 10857496]
- Sakorafas GH, Farnell MB, Farley DR, Rowland
CM, Sarr MG. Long-term results after surgery for
chronic pancreatitis. Int J Pancreatol 2000; 27:131-42.
[PMID 10862512]
- Takano S, Ito Y, Oishi H, Kono S, Yokoyama T,
Kubota N, Iwai S. A retrospective analysis of 88
patients with pancreaticogastrostomy after pancreaticoduodenectomy.
Hepatogastroenterology 2000;
47:1454-7. [PMID 11100375]
- Yamaguchi K, Yokohata K, Nakano K, Ohtani K,
Ogawa Y, Chijiiwa K, Tanaka M. Which is a less
invasive pancreatic head resection: PD, PPPD, or
DPPHR? Dig Dis Sci 2001; 46:282-8. [PMID
11281176]
- Yamaguchi K, Yokohata K, Ohkido M, Watanabe
M, Ogawa Y, Chijiiwa K, Tanaka M. Which is less
invasive. Distal pancreatectomy or segmental
resection? Int Surg 2000; 85:297-302. [PMID
11589595]
- Ohtsuka T, Yamaguchi K, Chijiiwa K, Tanaka M.
Postoperative pancreatic exocrine function influences
body weight maintenance after pylorus-preserving
pancreatoduodenectomy. Am J Surg 2001; 182:524-9.
[PMID 11754863]
- Osti MF, Costa AM, Bianciardi F, De Nicolo M,
Donato V, Silecchia G, Enrici RM. Concomitant
radiotherapy with protracted 5-fluorouracil infusion in
locally advanced carcinoma of the pancreas: a phase II
study. Tumori 2001; 87:398-401. [PMID 11989594]
- Yamaguchi K, Nakano K, Kobayashi K, Ogura Y,
Konomi H, Sugitani A, Tanaka M. Appleby operation
for pancreatic body-tail carcinoma: report of three
cases. Surg Today 2003; 33:873-8. [PMID 14605963]
- Tezel E, Kaneko T, Sugimoto H, Takeda S, Inoue
S, Nagasaka T, Nakao A. Clinical significance of
intraportal endovascular ultrasonography for the
diagnosis of extrapancreatic nerve plexus invasion by
pancreatic carcinoma. Pancreatology 2004; 4:76-81.
[PMID 15017121]
- Gruessner RW, Sutherland DE, Dunn DL,
Najarian JS, Jie T, Hering BJ, Gruessner AC.
Transplant options for patients undergoing total
pancreatectomy for chronic pancreatitis. J Am Coll
Surg 2004; 198:559-67. [PMID 15051008]
- Imamura M, Doi R. Treatment of locally advanced
pancreatic cancer: should we resect when resectable?
Pancreas 2004; 28:293-5. [PMID 15084974]
- Imamura M, Doi R, Imaizumi T, Funakoshi A,
Wakasugi H, Sunamura M, et al. A randomized
multicenter trial comparing resection and
radiochemotherapy for resectable locally invasive
pancreatic cancer. Surgery 2004; 136:1003-11. [PMID
15523393]
- Shimada K, Sano T, Sakamoto Y, Kosuge T. Safe
management of the pancreatic remnant with prolamine
duct occlusion after extended pancreaticoduodenectomy.
Hepatogastroenterology 2005;
52:1874-7. [PMID 16334797]
- Caronna R, Cardi M, Sammartino P, Mangioni S,
Pittau G, Scozzafava S, et al. Functional results of a
personal technique of reconstruction after
pancreaticoduodenectomy. J Exp Clin Cancer Res
2003; 22(4 Suppl):187-9. [PMID 16767929]
- Easter DW, Cuschieri A. Total pancreatectomy
with preservation of the duodenum and pylorus for
chronic pancreatitis. Ann Surg 1991; 214:575-80.
[PMID 1953110]
- Buchler MW, Friess H, Muller MW, Wheatley
AM, Beger HG. Randomized trial of duodenumpreserving
pancreatic head resection versus pyloruspreserving
Whipple in chronic pancreatitis. Am J Surg
1995; 169:65-9. [PMID 7818000]
- Takada T. Pylorus-preserving pancreatoduodenectomy:
technique and indications. Hepatogastroenterology
1993; 40:422-5. [PMID 7903659]
- Ryu M, Takayama W, Watanabe K, Honda I,
Yamamoto H, Arai Y. Ventral pancreatic resection for
adenoma and low-grade malignancies of the head of
the pancreas. Surg Today 1996; 26:476-81. [PMID
8840427]
- Mayumi T, Nimura Y, Kamiya J, Kondo S,
Nagino M, Kanai M, et al. Distal pancreatectomy with
en bloc resection of the celiac artery for carcinoma of
the body and tail of the pancreas. Int J Pancreatol 1997;
22:15-21. [PMID 9387020]
- Nimura Y. Pancreatic surgery: cutting-edge
developments and technology. Pancreas 1998; 16:227-
32. [PMID 9548659]
- Naganuma T, Isaji S, Kawarada Y. Staging and
extended resection for pancreatic cancer. Pancreas
1998; 16:355-62. [PMID 9548679]
- Nakao A. Pancreatic head resection with
segmental duodenectomy and preservation of the
gastroduodenal artery. Hepatogastroenterology 1998;
45:533-5. [PMID 9638444]
- Henne-Bruns D, Vogel I, Luttges J, Kloppel G,
Kremer B. Ductal adenocarcinoma of the pancreas
head: survival after regional versus extended
lymphadenectomy. Hepatogastroenterology 1998;
45:855-66. [PMID 9684147]
- Little JM. Chronic pancreatitis: results of a
protocol of management. Aust N Z J Surg 1983;
53:403-9. [PMID 6579950]
- Kiviluoto T, Schroder T, Lempinen M. Total
pancreatectomy for chronic pancreatitis. Surg Gynecol
Obstet 1985; 160:223-7. [PMID 3883550]
- Lygidakis NJ, Brummelkamp WH, Tytgat GH,
Huibtegtse KH, Lubbers MJ, van der Meer AD, et al.
Periampullary and pancreatic head carcinoma: facts
and factors influencing mortality, survival, and quality
of postoperative life. Am J Gastroenterol 1986; 81:968-
74. [PMID 3766499]
- Kerremans RP, Penninckx FM, De Groote J,
Fevery J. Subtotal resection of the head of the pancreas
combined with ductal obliteration of the distal pancreas
in chronic pancreatitis. Ann Surg 1987; 205:240-5.
[PMID 3827358]
- Rossi RL, Rothschild J, Braasch JW, Munson JL,
ReMine SG. Pancreatoduodenectomy in the
management of chronic pancreatitis. Arch Surg 1987;
122:416-20. [PMID 3566523]
- Tamura K, Kin S, Nagami H, Yano S, Naitoh A,
Nakagawa M, Nakase A. Heterotopic autotransplantation
of the distal pancreas segment after
total pancreatectomy for cancer of the head of the
pancreas. Pancreas 1992; 7:664-71. [PMID 1448454]
- Ishikawa O, Ohigashi H, Nakaizumi A, Uehara H,
Kitamura T, Takenaka A, et al. Surgical resection of
potentially curable pancreatic cancer with improved
preservation of endocrine function. Further evaluation
of intraoperative cytodiagnosis. Hepatogastroenterology
1993; 40:443-7. [PMID 8270233]
- Yasue M, Sakamoto J, Morimoto T, Yasui K,
Kuno N, Kurimoto K, et al. Evaluation of the effect of
pancreatic resection in advanced pancreatic cancer with
special reference using hospital-free survival as a
measure of quality of life. Jpn J Clin Oncol 1995;
25:37-45. [PMID 7745821]
- Ishikawa O. Surgical technique, curability and
postoperative quality of life in an extended
pancreatectomy for adenocarcinoma of the pancreas.
Hepatogastroenterology 1996; 43:320-5. [PMID
8714223]
- Lillemoe KD, Cameron JL, Yeo CJ, Sohn TA,
Nakeeb A, Sauter PK, et al. Pancreaticoduodenectomy
and palliation in pancreatic carcinoma.
Gastroenterology 1997; 112:1046-8. [PMID 9041274]
- Takada T, Yasuda H, Amano H, Yoshida M, Ando
H. Results of a pylorus-preserving pancreatoduodenectomy
for pancreatic cancer: a comparison
with results of the Whipple procedure.
Hepatogastroenterology 1997; 44:1536-40. [PMID
9427018]
- Civello IM, Frontera D, Viola G, Cina G, Sganga
G, Crucitti F. Extensive resection in pancreatic cancer:
review of the literature and personal experience.
Hepatogastroenterology 1998; 45:1877-83. [PMID
9840168]
- Lygidakis NJ, Berberabe AE, Spentzouris N,
Dedemadi G, Kalligas T, Loukas G, Sotiropoulou V. A
prospective randomized study using adjuvant
locoregional chemoimmunotherapy in combination
with surgery for pancreatic carcinoma.
Hepatogastroenterology 1998; 45:2376-81. [PMID
9951927]
- Kawarada Y, Yokoi H, Isaji S, Naganuma T,
Tabata M, Machishi H, et al. Modified standard
pancreaticoduodenectomy for the treatment of
pancreatic head cancer. Digestion 1999; 60(Suppl
1):120-5. [PMID 10026445]
- Buhler L, Schmidlin F, de Perrot M, Borst F,
Mentha G, Morel P. Long-term results after surgical management of chronic pancreatitis.
Hepatogastroenterology 1999; 46:1986-9. [PMID
10430382]
- Tandon V. Duodenum preserving head resection
for chronic pancreatitis. Trop Gastroenterol 1999;
20:187-8. [PMID 10769611]
- Ong HS, Ng EH, Heng G, Soo KC.
Pancreaticoduodenectomy with pancreaticogastrostomy:
assessment of patients' nutritional status, quality
of life and pancreatic exocrine function. Aust N Z J
Surg 2000; 70:199-203. [PMID 10765904]
- Nakagohri T, Kenmochi T, Kainuma O, Tokoro Y,
Kobayashi S, Asano T. Inferior head resection of the
pancreas for intraductal papillary mucinous tumors.
Am J Surg 2000; 179:482-4. [PMID 11004335]
- Jordan PH Jr, Pikoulis M. Operative treatment for
chronic pancreatitis pain. J Am Coll Surg 2001;
192:498-509. [PMID 11294407]
- Neoptolemos JP, Stocken DD, Dunn JA, Almond
J, Beger HG, Pederzoli P, et al. Influence of resection
margins on survival for patients with pancreatic cancer
treated by adjuvant chemoradiation and/or
chemotherapy in the ESPAC-1 randomized controlled
trial. Ann Surg 2001; 234:758-68. [PMID 11729382]
- Hardacre JM, Iacobuzio-Donahue CA, Sohn TA,
Abraham SC, Yeo CJ, Lillemoe KD, et al. Results of
pancreaticoduodenectomy for lymphoplasmacytic
sclerosing pancreatitis. Ann Surg 2003; 237:853-8.
[PMID 12796582]
- Chen HM, Jan YY, Chao TC, Hwang TL, Chen
MF. Pancreatoduodenectomy for chronic pancreatitis
with an inflammatory mass of pancreatic head:
preoperative and postoperative functional assessment.
Hepatogastroenterology 2003; 50:2213-7. [PMID
14696501]
- Lygidakis NJ, Singh G, Bardaxoglou E, Dedemadi
G, Sgourakis G, Nestoridis J, et al. Mono-bloc total
spleno-pancreaticoduodenectomy for pancreatic head
carcinoma with portal-mesenteric venous invasion. A
prospective randomized study. Hepatogastroenterology
2004; 51:427-33. [PMID 15086174]
- House MG, Choti MA. Palliative therapy for
pancreatic/biliary cancer. Surg Oncol Clin N Am 2004;
13:491-503. [PMID 15236731]
- Beger HG, Schlosser W, Friess HM, Buchler MW.
Duodenum-preserving head resection in chronic
pancreatitis changes the natural course of the disease: a
single-center 26-year experience. Ann Surg 1999;
230:512-9. [PMID 10522721]
- Isaji S, Kawarada Y. Pancreatic head resection
with second-portion duodenectomy for benign lesions,
low-grade malignancies, and early stage carcinomas
involving the pancreatic head region. Am J Surg 2001;
181:172-6. [PMID 11425061]
- Howard TJ, Jones JW, Sherman S, Fogel E,
Lehman GA. Impact of pancreatic head resection on
direct medical costs in patients with chronic
pancreatitis. Ann Surg 2001; 234:661-7. [PMID
11685030]
- Jang JY, Kim SW, Park SJ, Park YH. Comparison
of the functional outcome after pylorus-preserving
pancreatoduodenectomy: pancreatogastrostomy and
pancreatojejunostomy. World J Surg 2002; 26:366-71.
[PMID 11865376]
- Aspelund G, Topazian MD, Lee JH, Andersen
DK. Improved outcomes for benign disease with
limited pancreatic head resection. J Gastrointest Surg
2005; 9:400-9. [PMID 15749604]
- Lang H, Faller H. Coping and adaptation in
pancreatectomized patients: a somatopsychic
perspective. Psychother Psychosom 1992; 57:17-28.
[PMID 1584894]
- Talbot ML, Foulis AK, Imrie CW. Total dorsal
pancreatectomy for intraductal papillary mucinous
neoplasm in a patient with pancreas divisum.
Pancreatology 2005; 5:285-8. [PMID 15855827]
- Yamaguchi K, Konomi H, Kobayashi K, Ogura Y,
Sonoda Y, Kawamoto M, et al. Total pancreatectomy
for intraductal papillary-mucinous tumor of the
pancreas: reappraisal of total pancreatectomy.
Hepatogastroenterology 2005; 52:1585-90. [PMID
16201122]
- Fischer CP, Hong JC. Method of pyloric
reconstruction and impact upon delayed gastric
emptying and hospital stay after pylorus-preserving
pancreaticoduodenectomy. J Gastrointest Surg 2006;
10:215-9. [PMID 16455453]
- Evans JD, Wilson PG, Carver C, Bramhall SR,
Buckels JA, Mayer AD, et al. Outcome of surgery for
chronic pancreatitis. Br J Surg 1997; 84:624-9. [PMID
9171747]
- Rumstadt B, Forssmann K, Singer MV, Trede M.
The Whipple partial duodenopancreatectomy for the
treatment of chronic pancreatitis. Hepatogastroenterology
1997; 44:1554-9. [PMID 9427021]
- Kuhlmann K, de Castro S, van Heek T, Busch O,
van Gulik T, Obertop H, Gouma D. Microscopically
incomplete resection offers acceptable palliation in
pancreatic cancer. Surgery 2006; 139:188-96. [PMID
16455327]
- Falconi M, Bassi C, Casetti L, Mantovani W,
Mascetta G, Sartori N, et al. Long-term results of
Frey's procedure for chronic pancreatitis: a longitudinal
prospective study on 40 patients. J Gastrointest Surg
2006; 10:504-10. [PMID 16627215]
- McLeod RS, Taylor BR, O'Connor BI, Greenberg
GR, Jeejeebhoy KN, Royall D, Langer B. Quality of
life, nutritional status, and gastrointestinal hormone profile following the Whipple procedure. Am J Surg
1995; 169:179-85. [PMID 7817989]
- Patel AG, Toyama MT, Kusske AM, Alexander P,
Ashley SW, Reber HA. Pylorus-preserving Whipple
resection for pancreatic cancer. Is it any better? Arch
Surg 1995; 130:838-42. [PMID 7632143]
- Kovacs I, Toth P, Arkosy P, Hamori J, Sapy P.
Surgical treatment of pancreatic head and
periampullary tumors. Acta Chir Hung 1997; 36:172-3.
[PMID 9408334]
- Todd KE, Lewis MP, Gloor B, Kusske AM,
Ashley SW, Reber HA. Management decisions for
unusual periampullary tumors. Am Surg 1997; 63:927-
32. [PMID 9322675]
- Melvin WS, Buekers KS, Muscarella P, Johnson
JA, Schirmer WJ, Ellison EC. Outcome analysis of
long-term survivors following pancreaticoduodenectomy.
J Gastrointest Surg 1998; 2:72-8.
[PMID 9841971]
- Huang JJ, Yeo CJ, Sohn TA, Lillemoe KD, Sauter
PK, Coleman J, et al. Quality of life and outcomes after
pancreaticoduodenectomy. Ann Surg 2000; 231:890-8.
[PMID 10816633]
- Ohtsuka T, Yamaguchi K, Chijiiwa K, Kinukawa
N, Tanaka M. Quality of life after pylorus-preserving
pancreatoduodenectomy. Am J Surg 2001; 182:230-6.
[PMID 11587683]
- Armstrong T, Walters E, Varshney S, Johnson CD.
Deficiencies of micronutrients, altered bowel function,
and quality of life during late follow-up after
pancreaticoduodenectomy for malignancy.
Pancreatology 2002; 2:528-34. [PMID 12435865]
- Ohtsuka T, Yamaguchi K, Chijiiwa K, Tanaka M.
Effect of gastrointestinal reconstruction on quality of
life and nutritional status after pylorus-preserving
pancreatoduodenectomy. Dig Dis Sci 2002; 47:1241-7.
[PMID 12064798]
- Nguyen TC, Sohn TA, Cameron JL, Lillemoe KD,
Campbell KA, Coleman J, et al. Standard vs. radical
pancreaticoduodenectomy for periampullary adenocarcinoma:
a prospective, randomized trial evaluating
quality of life in pancreaticoduodenectomy survivors. J
Gastrointest Surg 2003; 7:1-9. [PMID 12559179]
- Ohtsuka T, Yamaguchi K, Ohuchida J, Inoue K,
Nagai E, Chijiiwa K, Tanaka M. Comparison of quality
of life after pylorus-preserving pancreatoduodenectomy
and Whipple resection.
Hepatogastroenterology 2003; 50:846-50. [PMID
12828102]
- Nieveen van Dijkum EJ, Kuhlmann KF, Terwee
CB, Obertop H, de Haes JC, Gouma DJ. Quality of life
after curative or palliative surgical treatment of
pancreatic and periampullary carcinoma. Br J Surg
2005; 92:471-7. [PMID 15672431]
- Shaw CM, O'Hanlon DM, McEntee GP. Longterm
quality of life following pancreaticoduodenectomy.
Hepatogastroenterology 2005; 52:927-
32. [PMID 15966234]
- Seiler CA, Wagner M, Bachmann T, Redaelli CA,
Schmied B, Uhl W, et al. Randomized clinical trial of
pylorus-preserving duodenopancreatectomy versus
classical Whipple resection-long term results. Br J Surg
2005; 92:547-56. [PMID 15800958]
- Billings BJ, Christein JD, Harmsen WS,
Harrington JR, Chari ST, Que FG, et al. Quality-of-life
after total pancreatectomy: is it really that bad on longterm
follow-up? J Gastrointest Surg 2005; 9:1059-66.
[PMID 16269376]
- Nakano H, Bachellier P, Weber JC,
Oussoultzoglou E, Dieng M, Shimura H, et al. Arterial
and vena caval resections combined with
pancreaticoduodenectomy in highly selected patients
with periampullary malignancies. Hepatogastroenterology
2002; 49:258-62. [PMID 11941970]
- Garcia Sanchez MV, Lopez Vallejos P, Perez de
Luque D, Naranjo Rodriguez A, Hervas Molina A,
Gonzalez Galilea A, et al. Biliopancreatic tumors:
patient survival and quality of life after palliative
treatment. Rev Esp Enferm Dig 2004; 96:305-14.
[PMID 15180442]
- Schmidt U, Simunec D, Piso P, Klempnauer J,
Schlitt HJ. Quality of life and functional long-term
outcome after partial pancreatoduodenectomy:
pancreatogastrostomy versus pancreatojejunostomy.
Ann Surg Oncol 2005; 12:467-72. [PMID 15886907]
- Scheingraber S, Scheingraber T, Brauckhoff M,
Dralle H. Comparison between a general and a diseasespecific
health-related quality-of-life questionnaire in
patients after pancreatic surgery. J Hepatobiliary
Pancreat Surg 2005; 12:290-7. [PMID 16133695]
- Ouchi K, Sugawara T, Ono H, Fujiya T,
Kamiyama Y, Kakugawa Y, et al. Palliative operation
for cancer of the head of the pancreas: significance of
pancreaticoduodenectomy and intraoperative radiation
therapy for survival and quality of life. World J Surg
1998; 22:413-6. [PMID 9523525]
- Schoenberg MH, Schlosser W, Ruck W, Beger
HG. Distal pancreatectomy in chronic pancreatitis. Dig
Surg 1999; 16:130-6. [PMID 10207239]
- Sakorafas GH, Sarr MG, Rowland CM, Farnell
MB. Postobstructive chronic pancreatitis: results with
distal resection. Arch Surg 2001; 136:643-8. [PMID
11387000]
- DuBay D, Sandler A, Kimura K, Bishop W, Eimen
M, Soper R. The modified Puestow procedure for
complicated hereditary pancreatitis in children. J
Pediatr Surg 2000; 35:343-8. [PMID 10693693]
- Kalady MF, Broome AH, Meyers WC, Pappas
TN. Immediate and long-term outcomes after lateral pancreaticojejunostomy for chronic pancreatitis. Am
Surg 2001; 67:478-83. [PMID 11379654]
- Izbicki JR, Bloechle C, Broering DC, Kuechler T,
Broelsch CE. Longitudinal V-shaped excision of the
ventral pancreas for small duct disease in severe
chronic pancreatitis: prospective evaluation of a new
surgical procedure. Ann Surg 1998; 227:213-9. [PMID
9488519]
- Kokoska ER, Stapleton DR, Virgo KS, Johnson
FE, Wade TP. Quality of life measurements do not
support palliative pancreatic cancer treatments. Int J
Oncol 1998; 13:1323-9. [PMID 9824652]
- Heinemann V, Wilke H, Mergenthaler HG,
Clemens M, Konig H, Illiger HJ, et al. Gemcitabine
and cisplatin in the treatment of advanced or metastatic
pancreatic cancer. Ann Oncol 2000; 11:1399-403.
[PMID 11142479]
- Shinchi H, Takao S, Noma H, Matsuo Y, Mataki
Y, Mori S, Aikou T. Length and quality of survival
after external-beam radiotherapy with concurrent
continuous 5-fluorouracil infusion for locally
unresectable pancreatic cancer. Int J Radiat Oncol Biol
Phys 2002; 53:146-50. [PMID 12007953]
- Ducreux M, Rougier P, Pignon JP, Douillard JY,
Seitz JF, Bugat R, et al. A randomised trial comparing
5-FU with 5-FU plus cisplatin in advanced pancreatic
carcinoma. Ann Oncol 2002; 13:1185-91. [PMID
12181240]
- Madura JA, Canal DF, Lehman GA. Wall stentenhanced
lateral pancreaticojejunostomy for small-duct
pancreatitis. Arch Surg 2003; 138:644-9. [PMID
12799336]
- Katz MH, Bouvet M, Takimoto S, Spivack D,
Moossa AR, Hoffman RM. Survival efficacy of
adjuvant cytosine-analogue CS-682 in a fluorescent
orthotopic model of human pancreatic cancer. Cancer
Res 2004; 64:1828-33. [PMID 14996746]
- Chen VK, Arguedas MR, Baron TH. Expandable
metal biliary stents before pancreaticoduodenectomy
for pancreatic cancer: a Monte-Carlo decision analysis.
Clin Gastroenterol Hepatol 2005; 3:1229-37. [PMID
16361049]
- Sho M, Nakajima Y, Kanehiro H, Hisanaga M,
Nishio K, Nagao M, et al. A new evaluation of
pancreatic function after pancreatoduodenectomy using
secretin magnetic resonance cholangiopancreatography.
Am J Surg 1998; 176:279-82. [PMID
9776159]
- Wehler M, Nichterlein R, Fischer B, Farnbacher
M, Reulbach U, Hahn EG, Schneider T. Factors
associated with health-related quality of life in chronic
pancreatitis. Am J Gastroenterol 2004; 99:138-46.
[PMID 14687155]
- Fitzsimmons D, Kahl S, Butturini G, van Wyk M,
Bornman P, Bassi C, et al. Symptoms and quality of life in chronic pancreatitis assessed by structured
interview and the EORTC QLQ-C30 and QLQPAN26.
Am J Gastroenterol 2005; 100:918-26. [PMID
15784041]
- Farnell MB, Pearson RK, Sarr MG, DiMagno EP,
Burgart LJ, Dahl TR, et al. A prospective randomized
trial comparing standard pancreatoduodenectomy with
pancreatoduodenectomy with extended lymphadenectomy
in resectable pancreatic head
adenocarcinoma. Surgery 2005; 138:618-28. [PMID
16269290]
- Schniewind B, Bestmann B, Henne-Bruns D,
Faendrich F, Kremer B, Kuechler T. Quality of life
after pancreaticoduodenectomy for ductal
adenocarcinoma of the pancreatic head. Br J Surg
2006; 93:1099-107. [PMID 16779883]
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T,
Binmoeller KF, Broelsch CE. Duodenum-preserving
resection of the head of the pancreas in chronic
pancreatitis. A prospective, randomized trial. Ann Surg
1995; 221:350-8. [PMID 7726670]
- Bloechle C, Izbicki JR, Knoefel WT, Kuechler T,
Broelsch CE. Quality of life in chronic
pancreatitis.Results after duodenum-preserving
resection of the head of the pancreas. Pancreas 1995;
11:77-85. [PMID 7667246]
- Izbicki JR, Bloechle C, Broering DC, Knoefel
WT, Kuechler T, Broelsch CE. Extended drainage
versus resection in surgery for chronic pancreatitis: a
prospective randomized trial comparing the
longitudinal pancreaticojejunostomy combined with
local pancreatic head excision with the pyloruspreserving
pancreatoduodenectomy. Ann Surg 1998;
228:771-9. [PMID 9860476]
- Sohn TA, Campbell KA, Pitt HA, Sauter PK,
Coleman JA, Lillemo KD, et al. Quality of life and
long-term survival after surgery for chronic
pancreatitis. J Gastrointest Surg 2000; 4:355-64.
[PMID 11058853]
- Witzigmann H, Max D, Uhlmann D, Geissler F,
Ludwig S, Schwarz R, et al. Quality of life in chronic
pancreatitis: a prospective trial comparing classical
Whipple procedure and duodenum-preserving
pancreatic head resection. J Gastrointest Surg 2002;
6:173-9. [PMID 11992802]
- Witzigmann H, Max D, Uhlmann D, Geissler F,
Schwarz R, Ludwig S, et al. Outcome after duodenumpreserving
pancreatic head resection is improved
compared with classic Whipple procedure in the
treatment of chronic pancreatitis. Surgery 2003;
134:53-62. [PMID 12874583]
- Belina F, Fronek J, Ryska M. Duodenopancreatectomy
versus duodenum-preserving
pancreatic head excision for chronic pancreatitis.
Pancreatology 2005; 5:547-52. [PMID 16110253]
- Behrman SW, Mulloy M. Total pancreatectomy
for the treatment of chronic pancreatitis: indications,
outcomes, and recommendations. Am Surg 2006;
72:297-302. [PMID 16676850]
- Kelemen D, Horvath OP. Clinical experience with
different techniques of pancreatic head resection for
chronic pancreatitis. Dig Surg 2002; 19:28-34. [PMID
11961352]
- Rodriguez Rilo HL, Ahmad SA, D'Alessio D,
Iwanaga Y, Kim J, Choe KA, et al. Total
pancreatectomy and autologous islet cell
transplantation as a means to treat severe chronic
pancreatitis. J Gastrointest Surg 2003; 7:978-89.
[PMID 14675707]
- Strate T, Taherpour Z, Bloechle C, Mann O, Bruhn
JP, Schneider C, et al. Long-term follow-up of a randomized trial comparing the beger and frey
procedures for patients suffering from chronic
pancreatitis. Ann Surg 2005; 241:591-8. [PMID
15798460]
- Glimelius B, Hoffman K, Sjoden PO, Jacobsson
G, Sellstrom H, Enander LK, et al. Chemotherapy
improves survival and quality of life in advanced
pancreatic and biliary cancer. Ann Oncol 1996; 7:593-
600. [PMID 8879373]
- Ridwelski K, Fahlke J, Kuhn R, Hribaschek A,
Kettner E, Greiner C, et al. Multicenter phase-I/II study
using a combination of gemcitabine and docetaxel in
metastasized and unresectable, locally advanced
pancreatic carcinoma. Eur J Surg Oncol 2006; 32:297-
302. [PMID 16414235]


