Keywords
Choledochostomy; Jaundice, Obstructive; Palliative Care; Pancreatic Neoplasms; Stents
INTRODUCTION
In spite of the advances made in diagnostic procedures over the past several decades, only about 20% of pancreatic head cancers are found to be resectable at the time of presentation [1, 2, 3]. About 80% of pancreatic carcinomas are located in the head of the pancreas, and most (75%) are adenocarcinomas [4]. In the palliative setting, differentiation between carcinomas of the pancreatic head and the distal biliary tree is often impossible. However, both of these malignancies are usually adenocarcinomas and have the same symptoms when they reach advanced stages. Up to 90% of these patients exhibit the signs and symptoms of obstructive jaundice at the time of presentation [5, 6]. Jaundice can cause hepatic and renal failure and can also lead to dysfunction of the coagulation cascade. Therefore, treatment of obstructive jaundice is one of the major aims of palliative therapy for carcinomas of the pancreatic head.
Various palliative therapeutic strategies have been described. Today, the most common treatments are endoscopic biliary stenting and surgical biliary bypass surgery with or without concomitant gastrojejunostomy [7, 8, 9, 10]. In addition, radiologically-guided percutaneous transhepatic biliary drainage or transhepatic stent placement is typically reserved for patients with unresectable disease on initial imaging, and who are unable to undergo endoscopic drainage [11].
The major advantage of biliary stents is that the procedure used to place them is minimally invasive and well tolerated by patients. However, the palliative potential of the stent is limited by the possibility of the recurrence of jaundice secondary to stent migration, accretion, and obstruction [8, 12, 13]. Furthermore, tumor progression and duodenal obstruction may render repeat stenting impossible if the first stent has malfunctioned. Endoscopic biliary stenting is associated with lower early morbidity and mortality rates and a shorter initial hospital stay than surgical biliary bypass but, in terms of patient prognosis, there is no difference between stenting and surgical palliation [1, 14].
Recurrent jaundice after biliary bypass surgery is very rare, and because of this, surgical palliation is the only available option which provides the opportunity for long-term biliary drainage [15, 16]. Cholecystojejunostomy and hepaticojejunostomy are the established biliary bypass surgery procedures. Hepaticojejunostomy seems to have better long-term results and should be favored if it is feasible [17, 18]. However, in some cases, large malignancies or bulky portal lymphadenopathy may render it difficult to safely perform a hepaticojejunostomy.
After the biliary bypass portion of the operation has been completed, a gastroenterostomy can then be performed either to treat existing gastric outlet failure or with a prophylactic intent [9].
The aim of this study was to compare morbidity and mortality rates as well as the effectiveness of palliative biliary drainage procedures among patients undergoing surgical biliary bypass or endoscopic stenting for advanced pancreatic head or distal biliary duct carcinoma. Furthermore, we determined the frequency of re-hospitalization for recurrent jaundice in patients who underwent endoscopic stent placement. The overall goal of our study was to determine which procedure was associated with better patient outcomes.
PATIENTS AND METHODS
Over a period of 8 years, we retrospectively analyzed the clinical records of a total of 342 patients (151 women, 191 men) with unresectable, histologically proven adenocarcinoma of the pancreatic head or distal biliary tree who presented for palliative therapy in our department. The median age of the patients included was 63 years (range: 36-89 years). At the time of diagnosis, obstructive jaundice was evident in 261 cases (76%) and these patients therefore required palliative treatment.
Patients with jaundice were divided into three groups based on the treatment they received (Figure 1):
Group 1: endoscopic stent placement without subsequent hepaticojejunostomy;
Group 2: preoperative stenting with subsequent palliative hepaticojejunostomy;
Group 3: hepaticojejunostomy without preoperative stenting.
Figure 1. Patient classification.
We determined the frequency of re-hospitalization for stent failure, stent-associated complications, and/or recurrent jaundice among the patients in Group 1. Patients in Group 2 underwent laparotomy with the aim of performing a curative resection. When the tumor was found to be unresectable or metastatic disease was noted at the time of surgery, a palliative hepaticojejunostomy was performed. Some of the patients in Group 2 (no. 15) underwent a hepaticojejunostomy for recurrent stent failure even though their tumors had been deemed unresectable.
Tissue was obtained for histological examination either intraoperatively, by ultrasound or by CT-guided fine needle aspiration. Data on short- and long-term postoperative or post-interventional morbidity rates were collected. We also calculated 30-day mortality rates for each group of patients. Survival data were collected by telephoning the appropriate general practitioner, by examining hospital records, or by examining records from our affiliated cancer center. The decision to perform endoscopic stenting vs. surgery was based on the suggestion of our interdisciplinary discussion with due regard to the patient’s general health status, and the cancer staging. In addition, all options of palliative treatment were extensively discussed with the patient. None of the patients with histologically proven distant metastases underwent surgical therapy.
All patients who underwent endoscopic placement had a plastic biliary stent placed using a side-viewing endoscope under fluoroscopic guidance. Stent position was confirmed by injecting contrast into the stent following placement to ensure that it was positioned above the bile duct stricture. Patients undergoing palliative surgery all underwent hepaticojejunostomy. A gastroenterostomy only was performed in cases of apparent duodenal obstruction. No patient underwent prophylactic gastroenterostomy. The patients received palliative chemotherapy on an individual basis.
ETHICS
Oral informed consent was obtained from each patient and the study protocol conformed to the ethical guidelines of the “World Medical Association Declaration of Helsinki” Ethical Principles for Medical Research Involving Human Subjects adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004. Inasmuch as it was a retrospective analysis of anonymized data, there was neither an a priori ethics review possible nor retrospectively necessary according to our institutional board (Ethikkommission der TU Dresden). All patients contacted later for follow-up gave their oral consent to be included in the study.
STATISTICS
Statistical analysis was performed with SPSS Version 11.5 (SPSS Inc. Chicago IL, USA). Median survival time (together with 95% CI) was calculated via the Kaplan-Meier method and the data were analyzed by means of the log-rank test. The interval between initial stent placement and stent replacement is expressed as mean±SD. Categorical variables are described by means of absolute and relative frequencies and were analyzed by using the Fisher’s exact and the Pearson chi-squared tests. Two-tailed P values of less than 0.05 were considered statistically significant.
RESULTS
Over the 8-year period we studied, a total of 342 patients underwent palliative treatment for pancreatic head carcinoma or carcinoma of the distal biliary tree. These two types of tumors were combined for the analysis because accurate differentiation between the two tumor types is not feasible in the palliative setting. At the time of presentation, 261 patients (76.3%) exhibited signs and symptoms of obstructive jaundice. These patients were divided into the aforementioned three groups based on the treatment they received (Figure 1). In 14 patients with obstructive jaundice, endoscopic stent implantation and/or surgery were impossible due to poor patient condition. In these patients, the obstructive jaundice was treated radiologically by percutaneous transhepatic biliary drainage.
Morbidity showed significant differences among the three groups (P=0.011): patients who only underwent stenting (Group 1: 7/138, 5.1%) had a significantly lower morbidity rate than patients treated with preoperative stenting and subsequent palliative hepaticojejunostomy (Group 2: 12/68, 17.6%; P=0.008)) while the comparison between patients who underwent hepaticojejunostomy without preoperative stenting did not reach the significant level (Group 3: 6/41, 14.6%; P=0.078).
The complications are listed in detail in Table 1. In Group 1, three patients developed cholangitis or pneumonia and had to be treated with antibiotics. Four patients had to have their stent changed during the initial hospital stay due to stent obstruction. A total of 81 patients (58.7%) treated only with endoscopic plastic stent placement were re-hospitalized for stent failure or scheduled exchange; all of these patients had a new biliary stent placed. The estimated mean interval between initial stent placement and stent replacement was 70.8±32.0 days.
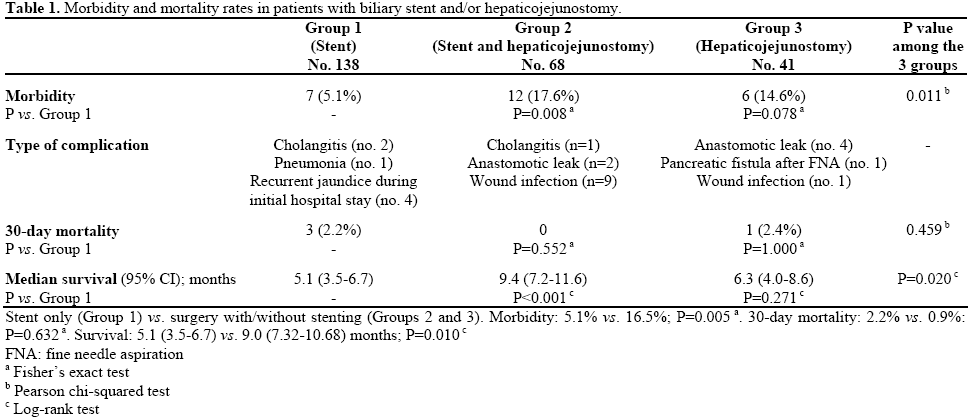
Only two patients (2.9%) in Group 2 showed evidence of an anastomotic leak after hepaticojejunostomy and preoperative biliary stenting; of these two patients, one patient underwent reoperation and the other one was treated with ultrasound-guided drainage. The nine cases of postoperative wound infection which occurred in Group 2 (13.2%) were all considered to be mild complications.
In four patients who did not undergo preoperative biliary stenting (Group 3), leakage occurred at the anastomotic site after the hepaticojejunostomy (9.8%). One of them underwent reoperation due to peritonitis and drainage failure. One patient in this group developed a pancreatic fistula after fine needle aspiration of the pancreatic tumor (2.4%), and one patient experienced postoperative wound infection (2.4%).
None of the patients who underwent surgery (Groups 2 and 3; n=109) had to be re-hospitalized for recurrent jaundice. Additionally, gastroenterostomy (n=13; 11.9%) was only performed primarily in patients with evidence of duodenal obstruction without any increase in morbidity. In 3 out of the other 96 patients (3.1%), only duodenal obstruction after hepaticojejunostomy was observed and led to re-operation (gastroenterostomy).
There were no significant differences in the mortality rates observed among the three patient groups (Group 1: 2.2%; Group 2: 0%; Group 3: 2.4%; P=0.459). Among patients who underwent stent placement without subsequent surgery (Group 1), one death was attributed to cholangitis and subsequent sepsis and two other patients died due to reasons unrelated to the procedure carried out for their underlying disease. One patient in Group 3 died after hepaticojejunostomy due to leakage at the anastomotic site and subsequent sepsis (2.4%).
Overall survival was significantly different among the 3 groups of patients (P=0.020) (Figure 2 and Table 1). In particular, median overall survival was significantly (P=0.010) greater in patients who underwent palliative surgery with or without stent placement (Groups 2 and 3: 9.0 months) than in the patients who only underwent stent placement (Group 1: 5.1 months). When the outcomes of patients in Group 1 (stent) were compared to those of patients in Group 2 (stent and hepaticojejunostomy), we found that the patients in Group 2 had significantly longer median survival (9.4 months; P<0.001).
Figure 2. Overall survival following endoscopic stent placement
and/or palliative surgery.
DISCUSSION
About 70% of the patients with pancreatic cancer have evidence of obstructive jaundice at the time of presentation. Therefore, the main goal of palliative therapy in patients with unresectable carcinoma of the pancreatic head or distal biliary tree is to resolve the biliary obstruction [1, 6]. There is still disagreement as to whether endoscopic or surgical palliation is associated with a better outcome, and there have been a number of retrospective studies which have shown the superiority of one treatment or the other (i.e., endoscopic vs. surgical treatment) [19, 20, 21]. Furthermore, there have only been four randomized trials comparing the outcomes of endoscopic stent placement vs. surgical biliary bypass in a palliative setting (Table 2). However, it must be noted that these studies were carried out a long time ago.
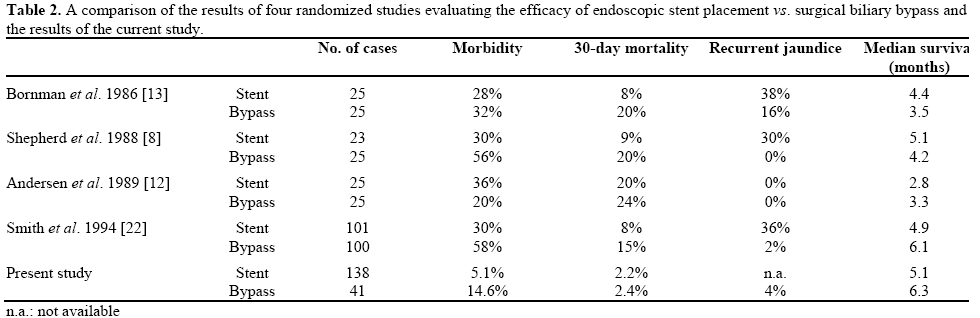
Regarding patient prognosis, there seems to be no difference between these two treatment methods, but short- and long-term results vary considerably (Table 2).
Watanapa and Williamson [1], as well as Van der Bosch et al. [14], have shown that endoscopic stenting has lower morbidity during the initial post-procedural period. However, as the length of follow-up increased in these studies, 20-50% of patients developed complications, such as cholangitis or recurrent jaundice. These complications had an especially large impact on the long-term survivors in these studies. However, while studies of patients who underwent hepaticojejunostomy found that these patients had higher morbidity rates during the initial postoperative period as well as longer post-procedural hospital stays, the occurrence of long-term sequelae (such as recurrent jaundice) was unusual (0-7%) [8, 12, 13, 22]. In another study, Schwarz et al. [23] stated that an endoprothesis should be placed if the patient has evidence of metastatic disease or if surgical palliation is not feasible. A later meta-analysis noted that the available data did not provide definitive evidence as to which treatment was preferable [24].
In conclusion, several authors, including Van Heek et al. [6], have stated that patient prognosis should guide the decision as to whether surgery or stent placement is more clinically appropriate. They recommended that endoscopic stenting should be performed in patients with a poor prognosis (i.e., a life expectancy less than 6 months) and that patients with a life expectancy of greater than 6 months should be treated with biliary bypass surgery because of the better long-term results associated with surgery. Thus, it is evident that evaluation of patient prognosis in the palliative setting is needed and can be used to guide treatment decisions. Our results show that the median survival time of patients treated with hepaticojejunostomy alone is longer than that of patients who were treated with endoscopic stent placement (6.3 vs. 5.1 months, respectively; P=0.271) (Tables 1 and 2). The randomized study performed by Smith et al. [22] showed very similar results (Table 2). In prior studies by Bornmann et al. [13], Shepherd et al. [8], and Andersen et al. [12], the median survival times were much lower overall, and the patients who had undergone endoscopic stent placement seemed to have a survival benefit (Table 2). However, due to the retrospective nature of our analysis, it is not possible to presume causality between surgery and better median survival times. Furthermore, in our study, the extent of the disease was not considered. Despite this limitation, it is plausible that, by allowing patients to avoid hospital admissions for recurrent jaundice and sepsis, surgical biliary bypass (hepaticojejunostomy) may lead to increased survival in the surgically treated group (Group 3). Thus, given the previously demonstrated improved long-term results associated with surgical treatment, hepaticojejunostomy is preferable in cases with a potentially better prognosis.
Patients who underwent preoperative stent placement and were subsequently treated with hepaticojejunostomy (Group 2) demonstrated a significantly longer survival time (median: 9.4 month) than patients only treated with stent (Group 1) (median: 5.1 months; P<0.001) (Table 1).
However, it was not possible to determine whether treatment choice had a causal effect on survival with this type of study design. It is possible that patients in Group 2 (stent and hepaticojejunostomy) initially had a lower tumor burden than those who underwent only stenting (Group 1) or primary palliative surgery (Group 3), which would likely lead to a better prognosis among patients in Group 2. Furthermore, most of the preoperatively stented patients (Group 2) were initially expected to be resectable.
The 30-day mortality rates (2.2%, 0%, and 2.4% in Groups 1, 2, and 3, respectively) observed in this study were lower than the observed mortality rates in the aforementioned randomized trials [8, 12, 13, 22] (Table 2).
In terms of overall morbidity, our patients experienced relatively low complication rates. Patients treated with a hepaticojejunostomy had a morbidity rate of only 14.6%, and the complications they experienced were typical postoperative complications, such as peritonitis, anastomotic failure and wound infection. None of the surgically treated patients (hepaticojejunostomy) were readmitted for recurrent jaundice. The types of complications observed in patients in Group 2 (overall morbidity rate 17.6%) were largely associated with the surgical intervention they underwent (i.e., wound infection (13.2%) or anastomotic failure (2.9%)). These findings support the established results that surgery is associated with higher initial morbidity rates, but that it has advantages with regard to long-term outcomes [22].
Also in agreement with the literature, we found that patients who underwent endoscopic biliary stenting only (Group 1) had significantly lower morbidity rates (5.1%, P=0.005) than patients who underwent surgery (overall 16.5%: 17.6% in Group 2 and 14.6% in Group 3) [14, 22]. Complications associated with endoscopically placed biliary stents should be considered to be early complications (Table 1). In a study by Pellicer et al. [25], 44% of biliary stents had to be changed after a mean time of 39 days. In our analysis, the mean interval between initial stent placement and stent replacement was 70.8±32.0 days (mean±DS). In this study, only biliary plastic stents were used, and therefore, the efficacy of metallic stents remains unclear. Metallic stents are postulated to have a longer duration of patency than plastic stents, but they may still become occluded by tumor growth into the stent lumen [26, 27]. There has only been one retrospective study comparing the efficacy of metallic stents with surgery, and it concluded that metallic stents were cost-effective when compared to surgical biliary bypass but had a higher rate of late complications (e.g., duodenal obstruction, acute cholangitis, recurrent jaundice) [28]. However, it must be pointed out that nowadays metallic stents have become the standard of care in palliative treatment of obstructive jaundice. However, according to the literature and our own results, plastic stents may remain an option for patients with larger tumors (greater than 30 mm) [11] and a poor prognosis [26, 28].
Due to general inoperability and local tumor spread which rendered endoscopic stent placement impossible in 14 patients (5.3% of the 261 patients with obstructive jaundice), neither stenting nor surgical palliation was possible. These patients were successfully treated with percutaneous transhepatic biliary drainage. Because of the reduction in quality of life, this procedure has only been used as a last option. However, recent developments in percutaneous transhepatic stenting could be a promising alternative for these patients, as percutaneous drainage is successful in 96 to 100% of cases when endoscopic retrograde cholangiopancreatography fails [29]. Radiology-guided procedures may involve placement of internal stents similar to those placed endoscopically or may involve external drainage when placement of a stent is not possible.
According to our experience, the best policy might be to perform a gastrojejunostomy only in cases of duodenal obstruction, as most patients do not live long enough to develop gastric outlet obstruction, thereby making prophylactic gastroenterostomy unnecessary. In our analysis only 3.1% (no. 3) of the patients developed duodenal obstruction after palliative hepaticojejunostomy, which corresponds to the results of Di Foronzo et al. [30]. Other authors disagree and favor prophylactic gastroenterostomy in this patient population, which might be preferable, as complications and morbidity are not greater when compared to hepaticojejunostomy alone [9, 31, 32]. In conclusion, based on the results of our study as well as on other reports, it seems that surgical biliary bypass surgery (hepaticojejunostomy) can be performed efficaciously and with acceptable morbidity and mortality rates. None of the surgically treated patients in our series had to be readmitted to the hospital for recurrent jaundice. Regarding the frequency of rehospitalization due to stent failure or scheduled stent exchange (which occurred at a mean interval of 70.8 days after the initial stent placement), an hepaticojejunostomy seems to have better long term results than endoscopic stenting; it should therefore be favored for patients with a life expectancy of greater than 6 months. When concluding our data and the results of other authors, surgical palliation shows at least a tendency of improving the quality of life for patients as compared to palliative biliary stenting [6, 24, 33]. We feel that this is especially true if a tumor is only proven to be unresectable at the time of surgical exploration. In these cases, a hepaticojejunostomy should be considered even if biliary stenting had been successful before surgery.
Conflict of interest The authors have no potential conflict of interest
References
- Watanapa P, Williamson RC. Surgical palliation for pancreatic cancer: developments during the past two decades. Br J Surg 1992; 79:8-20. [PMID 1371087]
- Warshaw AL, Fernández-del Castillo C. Pancreatic carcinoma. N Engl J Med 1992; 326:455-65. [PMID 1732772]
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg 1999; 189:1-7. [PMID 10401733]
- Lüttges J, Klöppel G. Pancreatic ductal adenocarcinoma and its precursors Pathologe 2005; 26:12-17 [PMID 15630571]
- Singh SM, Longmire WP Jr, Reber HA. Surgical palliation for pancreatic cancer. The UCLA experience. Ann Surg 1990; 212:132- 9. [PMID 1695834]
- van Heek NT, van Geenen RC, Busch OR, Gouma DJ. Palliative treatment in "peri"-pancreatic carcinoma: stenting or surgical therapy? Acta Gastroenterol Belg 2002; 65:171-5 [PMID 12420610]
- Huibregtse K, Tytgat GN. Palliative treatment of obstructive jaundice by transpapillary introduction of large bore bile duct endoprosthesis. Gut 1982; 23:371-5 [PMID 7076014]
- Shepherd HA, Royle G, Ross AP, Diba A, Arthur M, Colin- Jones D. Endoscopic biliary endoprosthesis in the palliation of malignant obstruction of the distal common bile duct: a randomized trial. Br J Surg 1988; 75:1166-8. [PMID 2466520]
- Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman J, et al. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomized trial. Ann Surg 1999; 230:322-8. [PMID 10493479]
- Lillemoe KD, Pitt HA. Palliation. Surgical and otherwise. Cancer 1996; 78(Suppl 3):605-14. [PMID 8681299]
- Prat F, Chapat O, Ducot B, Ponchon T, Fritsch J, Choury AD, Pelletier G, Buffet C. Predictive factors for survival of patients with inoperable malignant distal biliary strictures: a practical management guideline. Gut 1998; 42:76-80 [PMID 9505889]
- Andersen JR, Sørensen SM, Kruse A, Rokkjaer M, Matzen P. Randomised trial of endoscopic endoprosthesis versus operative bypass in malignant obstructive jaundice. Gut 1989; 30:1132-5. [PMID 2475392]
- Bornman PC, Harries-Jones EP, Tobias R, Van Stiegmann G, Terblanche J. Prospective controlled trial of transhepatic biliary endoprosthesis versus bypass surgery for incurable carcinoma of head of pancreas. Lancet 1986; 327:69-71. [PMID 2417075]
- van der Bosch RP, van Eijck CH, Mulder PG, Jeekel J. Serum CA 19-9 determination in the management of pancreatic cancer. Hepatogastroenterology 1996; 43:710-3 [PMID 8799418]
- Lillemoe KD, Barnes SA. Surgical palliation of unresectable pancreatic carcinoma. Surg Clin North Am 1995; 75:953-68. [PMID 7544919]
- Parks RW, Johnston GW, Rowlands BJ. Surgical biliary bypass for benign and malignant extrahepatic biliary tract disease. Br J Surg 1997; 84:488-92. [PMID 9112898]
- Sarr MG, Cameron JL. Surgical palliation of unresectable carcinoma of the pancreas. World J Surg 1984; 8:906 [PMID 6083677]
- Urbach DR, Bell CM, Swanstrom LL, Hansen PD. Cohort study of surgical bypass to the gallbladder or bile duct for palliation of jaundice due to pancreatic cancer. Ann Surg 2003; 237:86-93. [PMID 12496534]
- Wagner M, Egger B, Kulli C, Redaelli CA, Krähenbühl L, Seiler CA, Büchler MW. Stent or surgical bypass as palliative therapy in obstructive jaundice. Swiss Surg 2000; 6:283-8. [PMID 11077497]
- Nuzzo G, Clemente G, Cadeddu F, Giovannini I. Palliation of unresectable periampullary neoplasms. "surgical" versus "nonsurgical" approach. Hepatogastroenterology 2004; 51:1282-5. [PMID 15362733]
- Santagati A, Ceci V, Donatelli G, Pasqualini MJ, Silvestri F, Pitasi F, et al. Palliative treatment for malignant jaundice: endoscopic vs surgical approach. Eur Rev Med Pharmacol Sci 2003; 7:175-80. [PMID 15206487]
- Smith AC, Dowsett JF, Russell RC, Hatfield AR, Cotton PB. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet 1994; 344:1655-60. [PMID 7996958]
- Schwarz A, Beger HG. Biliary and gastric bypass or stenting in nonresectable periampullary cancer: analysis on the basis of controlled trials. Int J Pancreatol 2000; 27:51-8. [PMID 10811023]
- Taylor MC, McLeod RS, Langer B. Biliary stenting versus bypass surgery for the palliation of malignant distal bile duct obstruction: a meta-analysis. Liver Transpl 2000; 6:302-8. [PMID 10827230]
- Pellicer Bautista F, Martín Guerrero JM, Fernández Pérez FJ, Hassan Asad M, Pallarés Manrique H, Romero Castro R, et al. Edoscopic stenting in the management of malignant biliary obstruction. Rev Esp Enferm Dig 1998; 90:73-84. [PMID 9567641]
- Davids PH, Groen AK, Rauws EA, Tytgat GN, Huibregtse K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992; 340:1488-92. [PMID 1281903]
- Costamagna G, Mutignani M. Pancreatic stenting for malignant ductal obstruction. Dig Liver Dis 2004; 36:635-8. [PMID 15460850]
- Maosheng D, Ohtsuka T, Ohuchida J, Inoue K, Yokohata K, Yamaguchi K, et al. Surgical bypass versus metallic stent for unresectable pancreatic cancer. J Hepatobiliary Pancreat Surg 2001; 8:367-73. [PMID 11521183]
- Kaskarelis IS, Papadaki MG, Papageorgiou GN, Limniati MD, Malliaraki NE, Piperopoulos PN. Long-term follow-up in patients with malignant biliary obstruction after percutaneous placement of uncovered wallstent endoprostheses. Acta Radiol 1999; 40:528-33. [PMID 10485243]
- Di Fronzo LA, Cymerman J, Egrari S, O'Connell TX. Unresectable pancreatic carcinoma: correlating length of survival with choice of palliative bypass. Am Surg 1999; 65:955-8. [PMID 10515542]
- van Wagensveld BA, Coene PP, van Gulik TM, Rauws EA, Obertop H, Gouma DJ. Outcome of palliative biliary and gastric bypass surgery for pancreatic head carcinoma in 126 patients. Br J Surg 1997; 84:1402-6. [PMID 9361599]
- Lesurtel M, Dehni N, Tiret E, Parc R, Paye F. Palliative surgery for unresectable pancreatic and periampullary cancer: a reappraisal. J Gastrointest Surg 2006; 10:286-91. [PMID 16455463]
- Stumpf M, Kasperk R, Bertram P, Truong S, Schumpelick V. Role of surgical biliary bypass for palliation of pancreatic cancer: a retrospective study of 107 cases Zentralbl Chir 2001; 126 913-6. [PMID 11753803]



