Keywords
gemcitabine; Pancreatic Neoplasms; Regression Analysis; Salvage Therapy
INTRODUCTION
Pancreatic cancer is a fatal disease because it is difficult to diagnose early and has a poor prognosis. Most patients (80%) have locally advanced or metastatic pancreatic cancer at the time of diagnosis [1]. At present, single-agent gemcitabine is recommended as standard chemotherapy for patients with advanced pancreatic cancer and it has been extensively studied in phase II and III trials, especially as first-line chemotherapy. However, patients treated with gemcitabine alone still have a poor prognosis with a clinical benefit response rate of 23.8%, a median overall survival rate of 5.65 months and a 1-year overall survival rate of 18% [2].
In the last decade, several studies attempted to improve the efficacy of gemcitabine in advanced pancreatic cancer, not only by the addition of a second agent to a standard dose and schedule of gemcitabine but also by a fixed dose rate infusion of gemcitabine and also by the use of new agents, most of which had shown a limitation in terms of survival value. Several trials showed that gemcitabine-based doublet cytotoxic chemotherapy improved progression-free survival but not overall survival [3, 4, 5, 6]. With the exception of gemcitabine combined with erlotinib, gemcitabine plus target agents, such as cetuximab [7], bevacizumab [8] and axitinib [9], all had negative results. However, median overall survival only increased by 9 days when using gemcitabine combined with erlotinib in advanced pancreatic cancer [10]. Considering the expensive cost but limited efficacy of erlotinib, gemcitabine plus erlotinib has not been widely used for advanced pancreatic cancer in clinical practice. Phase III trials did not suggest that there could be a survival advantage from a fixed dose rate infusion of either gemcitabine or gemcitabine plus other agents [6, 11]. In addition, strategies with non-gemcitabine regimens had been assessed. A final result of the PRODIGE 4/ACCORD 11 trial [12] showed that 5-fluorouracil plus leucovorin, irinotecan and oxaliplatin (FOLFIRINOX) was associated with an almost doubling of overall survival over that of the standard of care (11.1 vs. 6.8 months) in patients with performance status 0 or 1. Although the regimen was effective, it was studied in a highly selected patient population, possibly enriched for patients without elevated bilirubin. Therefore, it might be a challenge to generalize the use of that regimen across the usual cohort of patients with metastatic pancreatic cancer. Other similar non-gemcitabine regimens had not shown better results [13, 14].
To date, second-line chemotherapy has not been well defined in advanced pancreatic cancer. No specific drugs have been considered as the best choice for second-line chemotherapy. The reason for this was that the majority of patients with progression after first-line chemotherapy had a poor performance status and could not receive the salvage therapy, which made the salvage therapy harder to study. However, several small phase II trials showed that survival advantage in advanced pancreatic cancer might benefit from the second-line chemotherapy [15, 16, 17].
Therefore, new strategies should be explored to promote progression in the treatment of advanced pancreatic cancer. Considering the platform of efficacy achieved with first-line chemotherapy, more attention should be paid to second-line chemotherapy and it should be studied more intensively. In the present study, we focused on exploring the possibility, using pooled analysis of the literature, that higher percentages of patients receiving second-line chemotherapy might result in a significant effect on survival benefit, especially in prolonging median overall survival in advanced pancreatic cancer.
METHODS
Literature Search
We searched in databases, such as MEDLINE, EMBASE, the Chinese Biomedical Literature Analysis and Retrieval System and EBM Reviews (Cochrane Database of Systematic Reviews) for recently published phase II or III trial results regarding the use of gemcitabine in advanced pancreatic cancer. The keywords used in the search were: pancreas, pancreatic cancer, pancreatic carcinoma, pancreatic adenocarcinoma, pancreatic neoplasm, chemotherapy, Gemzar® (Eli Lilly and Co., Indianapolis, IN USA) and gemcitabine. No language restrictions were applied. The search finished on April 31st, 2010.
Inclusion Criteria
Study Design
The papers had to have been published in peer-reviewed journals. The clinical trial had to have been a phase II or III prospective, properly randomized trial in which the information baseline in subgroups, such as age, sex, stage and performance status, was unbiased.
Study Population
Patients with advanced pancreatic cancer, as well as those with locally advanced and metastatic disease, were included in the study. Patients eligible for the study were required to have histologically or cytologically ascertained pancreatic cancer. Furthermore, patients were required to be adults over 18 years of age with a baseline Karnofsky performance status equal to, or greater than, 50% (or ECOG performance status less than 2). Patients had to have adequate hematological, renal, cardiac and hepatic functions. Patients had to have an estimated life expectancy of at least twelve weeks, no prior chemotherapy regimens, no prior radiation therapy or any other anti-tumor therapy in the 6 months prior to entry in the study.
Intervention
The control group received only gemcitabine in treating local or metastatic disease. The treatment group received gemcitabine-based combination therapy, which included gemcitabine plus either cytotoxic agents or targeted agents. Gemcitabine alone or gemcitabine-based combination chemotherapy was given as a first-line treatment until the disease progressed or the patient could no longer tolerate chemotherapy. Any cytotoxic drugs administered after the first-line chemotherapy for at least one cycle were considered to be second-line chemotherapy.
Types of Outcomes
The primary outcome measures were overall survival, which should have a survival curve or clear endpoint of survival. Overall survival was defined as the time interval from randomization to death from any cause or to the last follow-up in censored patients.
One secondary endpoint was progression-free survival, which was defined as the time from randomization to disease progression or death or that censored at the last follow-up. Some papers in the literature reported time to tumor progression or time to treatment failure instead of progression-free survival. Another secondary endpoint was residual survival, which is usually calculated from the date of disease progression after first-line chemotherapy to the date of death or that censored at the last follow-up. Because no individual patient data was available, for the sake of consistency with progression-free survival, in our study, we estimated residual survival by calculating the difference between the value of overall survival minus the value of progression-free survival.
The median value of each endpoint was used in the present study.
Exclusion Criteria
Patient populations of < 30 in each group were considered to be too small to continue analysis. Single arm phase II studies lacked baseline balance. The methodological quality of the trials was assessed using a validated scale (ranging from 0 to 5) applied to the items which influenced intervention efficacy. The scale reported by Jadad et al. [18] consisted of items pertaining to randomization, masking, dropouts and withdrawals. Low quality studies with a Jadad scale score of less than 2 points were not eligible for our study. The literature did not contain an exact rate or original information regarding second-line chemotherapy in the progression of pancreatic cancer.
Data Extraction
Two primary reviewers (Zhang YD and Yang Q) assessed all the abstracts that were identified from the sources. Both reviewers independently selected trials for inclusion according to prior agreement regarding the study population and the intervention. If one of the reviewers concluded an abstract might be eligible, the complete article was retrieved and reviewed in detail by both reviewers independently. Disagreements were resolved by consensus or by a third reviewer (Xie DR). The final decision was made by at least two reviewers. If the same trial was found but in different publications, the data of the final trial were chosen.
The following information was obtained from each trial: year of publication, number of patients, median age, gender (male vs. female), stage of disease (frequency of local advanced pancreatic cancer), performance status (frequency of ECOG performance status 0-1), chemotherapy regimen, combination chemotherapy (i.e., gemcitabine-combination chemotherapy vs. single agent gemcitabine), frequency of patients who had second-line chemotherapy, regimens of second-line chemotherapy, median overall survival, median progression free survival, and median residual survival. Data missing from the primary study reports was requested by the investigators.
ETHICS
The study was a retrospective data analysis, which was approved by the Institution of Scientific Research of Sun Yat-sen Memorial Hospital, and did not require patient consent. All aspects of the study conformed to the ethical guidelines of the Declaration of Helsinki 1964, as revised in Tokyo 2004.
STATISTICS
A multiple linear regression model was developed using the stepwise method, according to the least absolute value of the standardized partial regression coefficient. The two P values of 0.05 and 0.20 were chosen as limits for including or excluding the variables in the analysis, respectively. The set of exploratory variables included median age, gender, stage of disease, performance status, combination chemotherapy and second-line chemotherapy. Each variable was judged according to sample size. Three analyses were applied considering median overall survival, median progression-free survival and median residual survival.
RESULTS
Trial Flow
According to the pre-set inclusion and exclusion criteria, 1,682 potentially eligible published papers were included. Of these, 21 papers conformed to the inclusion criteria [3, 4, 5, 6, 7, 14, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33]. Of these 21, 11 papers conformed to the exclusion criteria [3, 4, 7, 14, 19, 20, 21, 22, 23, 24, 25]; therefore, 10 papers involving 2,679 patients were finally included [5, 6, 26, 27, 28, 29, 30, 31, 32, 33]. The flow chart of the selection of the literature is shown in Figure 1.
Figure 1. Flow chart of the selection of randomized controlled trials
for correlation analysis.
Characteristics of the Selected Trials
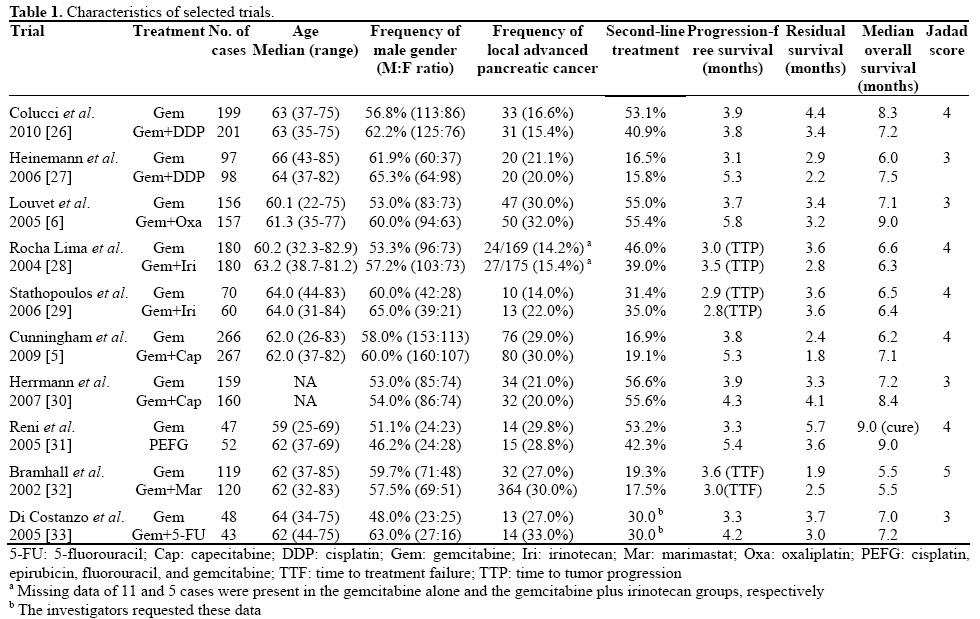
Ten prospective randomized controlled trials which achieved a score of three or more points in the Jadad scale were included in present study [5, 6, 26, 27, 28, 29, 30, 31, 32, 33]; only one trial was a Phase II randomized controlled trial and the others were Phase III randomized controlled trials. All detailed clinical characteristics were summarized in Table 1. Because different cut-offs of performance status were used to stratify patients in the original trials, performance status was considered as an unreliable variable in our multiple linear regression analyses in order to avoid artificial error.
Linear Regression of Median Overall Survival
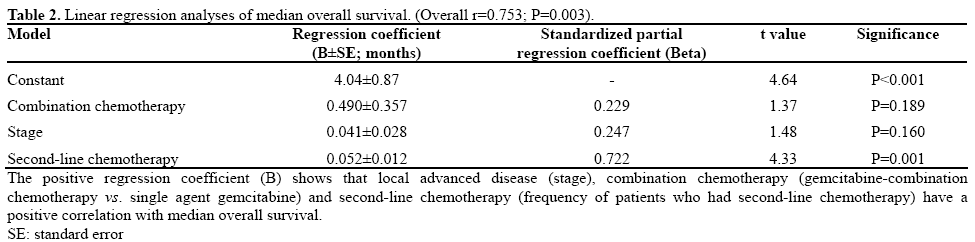
Three of the variables (stage of disease, combination chemotherapy, and second-line chemotherapy) entered into the stepwise multiple linear regression showed an independent positive correlation to median overall survival (overall r=0.753; P=0.003). The detailed results are shown in Table 2. The coefficient computed for second-line chemotherapy demonstrated that median overall survival would be prolonged for 0.052 months (about 1.56 days) if second-line chemotherapy was increased by 1%.
Correlation between Median Progression-Free Survival and Second-Line Chemotherapy
No variables were entered into the stepwise procedure when considering median progression-free survival as a dependent variable. In particular, univariate analysis showed that second-line chemotherapy and median progression-free survival had no significant correlation (r=0.092; P=0.701) (Figure 2).
Figure 2. Relationship between median progression-free survival and
second-line chemotherapy. Linear regression showed a correlation
coefficient of 0.092 which meant that the second-line chemotherapy
and progression-free survival had no significant correlation
(P=0.701).
Correlation between Median Residual Survival and Second-Line Chemotherapy
Unlike the non significant relationship between median progression-free survival and second-line chemotherapy, second-line chemotherapy had unique variables entering the stepwise procedure when median residual survival was considered as a dependent variable, showing a positive significant correlation (r=0.717; P<0.001). The result is shown in Figure 3.
Figure 3. Relationship between residual survival and second-line
chemotherapy. Linear regression showed a correlation coefficient of
0.717 which meant that the second-line chemotherapy and residual
survival had a significant positive correlation (P<0.001).
DISCUSSION
Our results showed that the median overall survival rate of patients with advanced pancreatic cancer was positively correlated to combination chemotherapy, stage of disease and second-line chemotherapy (r=0.753; P=0.003). Combination chemotherapy and disease stage affecting overall survival were similar to other studies [27, 30, 34, 35]. A positive correlation between second-line chemotherapy and median overall survival suggested that median overall survival would be prolonged about 1.56 days if patients accepted second-line chemotherapy increased by 1% (t=4.33; P=0.001). Theoretically, median overall survival would be increased by about 9 days in absolute value if the number of patients who accepted second-line chemotherapy was increased by 5.8%, which was similar to the survival benefit from gemcitabine combined with erlotinib [14]. With this increase in mind, the second-line chemotherapy rate in clinical practice might be easier than increasing the use of erlotinib.
Progression-free survival reflects the efficacy of first-line chemotherapy on cancer. Linear regression analyses showed that second-line chemotherapy has no significant correlation with progression-free survival (r=0.092; P=0.701). The residual survival rate estimates the time-interval between the date of disease progression after first-line chemotherapy to the date of death or that censored at the last follow-up. Theoretically it should be related to second-line chemotherapy and the best supportive care. Our results indicated that residual survival is positively related to second-line chemotherapy (r=0.717; P<0.001); that is, the statistical model correlated to clinical practice and this seems to be reasonable.
A standardized partial regression coefficient can be used to analyze the exact effect of each variable on overall survival. In our study, the standardized partial regression coefficient of second-line chemotherapy was 0.722, which was obviously larger than the variables of combination chemotherapy (0.229) and locally advanced disease (0.247). In other words, second-line chemotherapy had the biggest contribution to survival benefit. In the trials selected, median overall survival was approximately 7 months and median progression-free survival was about 3.9 months. Meanwhile, median residual survival was equal to approximately 3.3 months, which is approximately half the median overall survival. Our model pointed out the reason why second-line chemotherapy had the greatest contribution to overall survival. At the same time, it indirectly influenced overall survival through residual survival.
Although, based on our analysis, second-line chemotherapy positively correlated to survival benefit in advanced pancreatic cancer, it still did not answer whether advanced pancreatic cancer would benefit from second-line chemotherapy. One could argue that patients who live longer have a greater opportunity of being treated with second-line chemotherapy. However, several small phase II clinical trials have indicated a potential advantage in overall survival if second-line chemotherapy was used [36, 37]. The median overall survival rate was about 3-5 months, which seemed even better than our results (residual survival equal to 3.3 months). In addition, a phase III clinical trial showed that oxaliplatin plus folinic acid and 5-fluorouracil was superior as the best supportive care in the second-line chemotherapy of advanced pancreatic cancer with progression after gemcitabine [38]. Therefore, it seemed that patients treated with second-line chemotherapy would survive longer.
However, our study had the following limitations: i) data were collected based on published literature or information supplied by authors but not on individual patient data. Although we tried to request individual patient data for our study, it was difficult to get all the information we needed. Therefore, according to a linear correlation analysis carried out between the abstract data in the literature and individual patient data [39], which maintained that either method was feasible in high quality meta-analyses, in our situation (where no individual patient data were available) it was acceptable to carry out meta-analyses through abstract data in the literature; ii) only 10 clinical trials supplied information about second-line chemotherapy, and the second-line regimens were all different with capecitabine, 5-FU, S-1, oxaliplatin, cisplatin and exatecan being used in the majority of cases. The regimens, doses of drugs, and usage of drugs were not the same. Therefore, we could not arrive at a conclusion as to the effective regimen for second-line chemotherapy, based on our study. However, Mancuso et al. [40] found that DNA repair gene excision repair cross complementing 1 could influence overall survival, time to progression and response to chemotherapy. It indicated additional translational research by biological selection of populations in the second-line chemotherapy field and iii) it was reported that performance status was an important prognostic factor in advanced pancreatic cancer [30]. However, we could not analyze the correlation between performance status and overall survival because the patients were stratified based on different categories of performance status in the various trials, which might have affected the equation and final results. On the other hand, some might argue that patients in the early stage of disease could live longer and arrive at second-line treatment, which might affect overall survival. In our data, no significant correlation was found between second-line treatment and stage of the disease (r=-0.149; P=0.531). Although the definition of the best first-line chemotherapy regimen is presently a very difficult task, emphasis on second-line chemotherapy might be an effective way of improving overall patient survival. In order to gain more experience, we suggest that oncologists introduce more details about patients receiving second-line chemotherapy in clinical research reports after first-line chemotherapy fails in pancreatic cancer. We also advise more biological research in addition to clinical research.
In conclusion, second-line chemotherapy might affect the survival benefit of patients with advanced pancreatic cancer. Depending on the level of efficacy achieved with first-line chemotherapy, physicians should pay more attention to second-line chemotherapy and should conduct additional clinical trials to explore the value of second-line chemotherapy. On the other hand, pemetrexed, as a second-line drug, can be given immediately with a survival benefit for non-small cell lung cancer with stable disease after first-line chemotherapy [41]. Recently, a retrospective study indicated that capecitabine could be used safely as a maintenance agent in gastrointestinal cancer [42]. Therefore, second-line chemotherapy, given immediately in patients without progression after first-line chemotherapy, might improve overall survival in advanced pancreatic cancer; this fact is worthy of additional study in future.
Acknowledgements
We thank Professors Francesco Di Costanzo, Massimo Di Maio, and Richard Herrmann for their kind help in providing detailed second-line chemotherapy data
Authors’ contributions
Zhang YD and Yang Q contributed equally to this work
Funding
This work was supported by a grant from the Science and Technology Program Foundation of Guangdong Province, China (No. 2009B030801195)
Conflicts of interest
The authors have no potential conflicts of interest
References
- Yeo CJ. Cancer of the Pancreas. In: Devita VT Jr, Hellman S, Rosenberg SA. Cancer: Principles & Practice of Oncology, 7th ed USA Philadelphia: Lippincott Williams & Wilkins, 2005:945.
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID 9196156]
- Berlin JD, Catalano P, Thomas JP, Kugler JW, Haller DG, Benson AB 3rd. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern Cooperative Oncology Group Trial E2297. J Clin Oncol 2002; 20:3270-5. [PMID 12149301]
- Colucci G, Giuliani F, Gebbia V, Biglietto M, Rabitti P, Uomo G, et al. Gemcitabine alone or with cisplatin for the treatment of patients with locally advanced and/or metastatic pancreatic carcinoma: a prospective, randomized phase III study of the Gruppo Oncologia dell'Italia Meridionale. Cancer 2002; 94:902-10. [PMID 11920457]
- Cunningham D, Chau I, Stocken DD, Valle JW, Smith D, Steward W, et al. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. J Clin Oncol 2009; 27: 5513-8. [PMID 19858379]
- Louvet C, Labianca R, Hammel P, Lledo G, Zampino MG, André T, et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: results of a GERCOR and GISCAD phase III trial. J Clin Oncol 2005; 23:3509-16. [PMID 15908661]
- Philip PA, Benedetti J, Corless CL, Wong R, O'Reilly EM, Flynn PJ, et al. Phase III study comparing gemcitabine plus cetuximab versus gemcitabine in patients with advanced pancreatic adenocarcinoma: Southwest Oncology Group-Directed Intergroup Trial S0205. J Clin Oncol 2010; 28:3605-10. [PMID 20606093]
- Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, et al. Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: phase III trial of the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol 2010; 28:3617-22. [PMID 20606091]
- Spano JP, Chodkiewicz C, Maurel J, Wong R, Wasan H, Barone C, et al. Efficacy of gemcitabine plus axitinib compared with gemcitabine alone in patients with advanced pancreatic cancer: an open-label randomised phase II study. Lancet 2008; 371:2101-8. [PMID 18514303]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6. [PMID 17452677]
- Poplin E, Feng Y, Berlin J, Rothenberg ML, Hochster H, Mitchell E, et al. Phase III, randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose rate infusion) compared with gemcitabine (30-minute infusion) in patients with pancreatic carcinoma E6201: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol 2009; 27:3778-85. [PMID 19581537]
- Conroy T, Desseigne F, Ychou M, Ducreux M, Bouche O, Guimbaud R, et al. Randomized phase III trial comparing FOLFIRINOX (F: 5FU/leucovorin (LV), irinotecan (I), and oxaliplatin (O)) versus gemcitabine (G) as first-line treatment for metastatic pancreatic adenocarcinoma (MPA): Preplanned interim analysis results of the PRODIGE 4/ACCORD 11 trial. J Clin Oncol 2010; 28(15 Suppl.):Abstract 4010.
- Maisey N, Chau I, Cunningham D, Norman A, Seymour M, Hickish T, et al. Multicenter randomized phase III trial comparing protracted venous infusion (PVI) fluorouracil (5-FU) with PVI 5-FU plus mitomycin in inoperable pancreatic cancer. J Clin Oncol 2002; 20:3130-6. [PMID 12118027]
- Ducreux M, Rougier P, Pignon JP, Douillard JY, Seitz JF, Bugat R, et al. A randomised trial comparing 5-FU with 5-FU plus cisplatin in advanced pancreatic carcinoma. Ann Oncol 2002; 13:1185-91. [PMID 12181240]
- Cartwright TH, Cohn A, Varkey JA, Chen YM, Szatrowski TP, Cox JV, Schulz JJ. Phase II study of oral capecitabine in patients with advanced or metastatic pancreatic cancer. J Clin Oncol 2002; 20:160-4. [PMID 11773165]
- Pelzer U, Stieler J, Roll L, Hilbig A, Dörken B, Riess H, Oettle H. Second-line therapy in refractory pancreatic cancer. results of a phase II study. Onkologie 2009; 32:99-102. [PMID 19295247]
- Xiong HQ, Varadhachary GR, Blais JC, Hess KR, Abbruzzese JL, Wolff RA. Phase 2 trial of oxaliplatin plus capecitabine (XELOX) as second-line therapy for patients with advanced pancreatic cancer. Cancer 2008; 113:2046-52. [PMID 18756532]
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clin Trials 1996; 17:1-12. [PMID 8721797]
- Oettle H, Richards D, Ramanathan RK, van Laethem JL, Peeters M, Fuchs M, et al. A phase III trial of pemetrexed plus gemcitabine versus gemcitabine in patients with unresectable or metastatic pancreatic cancer. Ann Oncol 2005; 16:1639-45. [PMID 16087696]
- Abou-Alfa GK, Letourneau R, Harker G, Modiano M, Hurwitz H, Tchekmedyian NS, et al. Randomized phase III study of exatecan and gemcitabine compared with gemcitabine alone in untreated advanced pancreatic cancer. J Clin Oncol 2006; 24:4441-7. [PMID 16983112]
- Wang XY, Ni Q, Jin M, Li ZS, Wu YX, Zhao YP, Feng F. Gemcitabine or gemcitabine plus cisplatin for in 42 patients with locally advanced or metastatic pancreatic cancer. Chin J Oncol 2002; 24:404-7. [PMID 12408777]
- Yan ZC, Hong J, Xie GR. Observation of therapeutic efficacy of a biweekly regimen of Gemzar plus oxaliplatin for 30 cases with advanced pancreatic cancer. Chin J Clin Oncol 2007; 6:322-5.
- Scheithauer W, Schüll B, Ulrich-Pur H, Schmid K, Raderer M, Haider K, et al. Biweekly high-dose gemcitabine alone or in combination with capecitabine in patients with metastatic pancreatic adenocarcinoma: a randomized phase II trial. Ann Oncol 2003; 14:97-104. [PMID 12488300]
- Van Cutsem E, van de Velde H, Karasek P, Oettle H, Vervenne WL, Szawlowski A, et al. Phase III trial of gemcitabine plus tipifarnib compared with gemcitabine plus placebo in advanced pancreatic cancer. J Clin Oncol 2004; 22:1430-8. [PMID 15084616]
- Gansauge F, Ramadani M, Pressmar J, Gansauge S, Muehling B, Stecker K, et al. NSC-631570 (Ukrain) in the palliative treatment of pancreatic cancer. Results of a phase II trial. Langenbecks Arch Surg 2002; 386:570-4. [PMID 11914932]
- Colucci G, Labianca R, Di Costanzo F, Gebbia V, Cartenì G, Massidda B, et al. Randomized phase III trial of gemcitabine plus cisplatin compared with single-agent gemcitabine as first-line treatment of patients with advanced pancreatic cancer: the GIP-1 study. J Clin Oncol 2010; 28:1645-51. [PMID 20194854]
- Heinemann V, Quietzsch D, Gieseler F, Gonnermann M, Schönekäs H, Rost A, et al. Randomized phase III trial of gemcitabine plus cisplatin compared with gemcitabine alone in advanced pancreatic cancer. J Clin Oncol 2006; 24:3946-52. [PMID 16921047]
- Rocha Lima CM, Green MR, Rotche R, Miller WH Jr, Jeffrey GM, Cisar LA,et al. Irinotecan plus gemcitabine results in no survival advantage compared with gemcitabine monotherapy in patients with locally advanced or metastatic pancreatic cancer despite increased tumor response rate. J Clin Oncol 2004; 22:3776-83. [PMID 15365074]
- Stathopoulos GP, Syrigos K, Aravantinos G, Polyzos A, Papakotoulas P, Fountzilas G, et al. A multicenter phase III trial comparing irinotecan-gemcitabine (IG) with gemcitabine (G) monotherapy as first-line treatment in patients with locally advanced or metastatic pancreatic cancer. Br J Cancer 2006; 95:587-92. [PMID 16909140]
- Herrmann R, Bodoky G, Ruhstaller T, Glimelius B, Bajetta E, Schüller J, et al. Gemcitabine plus capecitabine compared with gemcitabine alone in advanced pancreatic cancer: a randomized, multicenter, phase III trial of the Swiss Group for Clinical Cancer Research and the Central European Cooperative Oncology Group. J Clin Oncol 2007; 25:2212-7. [PMID 17538165]
- Reni M, Cordio S, Milandri C, Passoni P, Bonetto E, Oliani C, et al. Gemcitabine versus cisplatin, epirubicin, fluorouracil, and gemcitabine in advanced pancreatic cancer: a randomised controlled multicentre phase III trial. Lancet Oncol 2005; 6:369-76. [PMID 15925814]
- Bramhall SR, Schulz J, Nemunaitis J, Brown PD, Baillet M, Buckels JA. A double-blind placebo-controlled, randomised study comparing gemcitabine and marimastat with gemcitabine and placebo as first line therapy in patients with advanced pancreatic cancer. Br J Cancer 2002; 87:161-7. [PMID 12107836]
- Di Costanzo F, Carlini P, Doni L, Massidda B, Mattioli R, Iop A, et al. Gemcitabine with or without continuous infusion 5-FU in advanced pancreatic cancer: a randomised phase II trial of the Italian oncology group for clinical research (GOIRC). Br J Cancer 2005; 93:185-9. [PMID 15986036]
- Xie DR, Yang Q, Chen DL, Jiang ZM, Bi ZF, Ma W, Zhang YD. Gemcitabine-based cytotoxic doublets chemotherapy for advanced pancreatic cancer: updated subgroup meta-analyses of overall survival. Jpn J Clin Oncol 2010; 40:432-41. [PMID 20147334]
- Vickers MM, Powell ED, Asmis TR, Jonker DJ, O'Callaghan CJ, Tu D, et al. Comorbidity and overall survival (OS) in patients with advanced pancreatic cancer (APC): Results from NCIC CTG PA.3-A phase III trial of erlotinib plus gemcitabine (E+G) versus gemcitabine (G) alone. J Clin Oncol 2010; 28(15 Suppl.):Abstract 4079.
- Nakai Y, Isayama H, Sasaki T, Sasahira N, Kogure H, Hirano K, et al. Impact of S-1 in patients with gemcitabine-refractory pancreatic cancer in Japan. Jpn J Clin Oncol 2010; 40:774-80. [PMID 20462979]
- Novarino A, Satolli MA, Chiappino I, Giacobino A, Bellone G, Rahimi F, et al. Oxaliplatin, 5-fluorouracil, and leucovorin as second-line treatment for advanced pancreatic cancer. Am J Clin Oncol 2009; 32:44-8. [PMID 19194124]
- Oettle H, Pelzer U, Stieler J, Hilbig A, Roll L, Schwaner I, et al. Oxaliplatin/folinic acid/5-fluorouracil 24h (OFF) plus best supportive care versus best supportive care alone (BSC) in second-line therapy of gemcitabine-refractory advanced pancreatic cancer (CONKO 003). J Clin Oncol 2005; 23(16 Suppl.):Abstract 4031.
- Brias E, Gralla RJ, Raftopoulos H, Giannarelli D. Comparing two methods of meta-analysis in clinical research - individual patient data-based (IPD) and literature-based abstracted data (AD) methods: Analyzing five oncology issues involving more than 10,000 patients in randomized clinical trials (RCTs). J Clin Oncol 2007; 25(18 Suppl.):Abstract 6512.
- Mancuso A, Sacchetta S, Saletti PC, Tronconi C, Milesi L, Garassino M, et al. Clinical and molecular determinants of survival in pancreatic cancer patients treated with second-line chemotherapy: results of an Italian/Swiss multicenter survey. Anticancer Res 2010; 30:4289-95. [PMID 21036754]
- Gridelli C, Di Maio M. The role of pemetrexed as maintenance treatment in advanced NSCLC: a Phase III randomized trial. Expert Opin Pharmacother 2010; 11:321-4. [PMID 20053140]
- Sun JF, Wu RR, Norris C, Noone AM, Amankwa-Sakyi M, Slack R, Marshall JL. Safety of chronic low-dose capecitabine as maintenance therapy in gastrointestinal cancers. Gastrointest Cancer Res 2009; 3:134-40. [PMID 19742139]




