Keywords
Colorectal Neoplasms; Neoplasm Metastasis; Pancreatic Neoplasms; Surgical Procedures, Operative; Survival
INTRODUCTION
The incidence of carcinomas metastasising to the pancreas is low, and in studies analysing post-mortem and surgical databases, have found the prevalence of different metastatic tumours to be 1.6% of all post-mortem cases and 3.9% of pancreatic resections [1,2]. The most common primary malignancies to metastaise to the pancreas are gastric, lung and bile duct cancers [1]. Other less common primaries include renal cell, breast small bowel, colorectal and melanoma. Due to the uncommon nature of pancreatic metastases, the benefit of surgical intervention in these patients remains uncertain.
Collective data from cases of colorectal carcinoma metastasising to sites other than the pancreas, such as liver, lung and regional lymph nodes are much more widely available [3]. Surgical resection of colorectal liver metastases has proved beneficial, with 5-year survival rates of up to 58%, with at least 17% of patients still alive at 10 years [4-6]. With improved colorectal cancer (CRC) survival, due to earlier detection and effective chemotherapeutics, a greater cohort of patients may enter long-term follow-up, potentially increasing the likelihood of diagnosing secondary pancreatic tumours [7].
It is therefore prudent to establish whether the surgical management of pancreatic metastases from CRC is associated with successful outcomes, as measured by long-term survival or effective palliation. This case series reports the long-term outcomes of patients with pancreatic metastasis arising from the colon and rectum.
METHODS
Patients were managed at Leeds Teaching Hospital Trust (LTHT), a tertiary referral centre for pancreatic disease. Patients with resectable colorectal pancreatic metastases (CRPM) undergoing surgical treatment (operative group) were identified from the units’ pancreatic database. A second group comprised of patients diagnosed with CRPM on cross-sectional imaging but not undergoing potentially curative surgery (non-operative group). This group was used to observe demographic and survival outcomes. These cases were sourced from the colorectal cancer database of the Yorkshire Regional Cancer Network and those patients with pancreatic metastases identified. Such patients undergo annual CT scans of the chest, abdomen, and pelvis for 3 years after resection of primary tumours, with a final CT 5 years after the initial surgery prior to discharge. In addition to CT, Ca19.9 measurements are obtained at diagnosis, and following surgery at 3 and 6 monthly intervals until discharge at 5 years.
We performed a retrospective data analysis reporting the results of imaging studies, pathological findings and outcomes of surgical and medical management until death or the present date (July 2013). Each patient was treated within a multidisciplinary team setting, receiving both surgical and oncological input. Operative management of colorectal and pancreatic disease was carried out within the same institution.
RESULTS
Searching the database revealed a total of 8228 patients who were diagnosed with primary colorectal adenocarcinoma. Nine patients who developed pancreatic metastases were identified. Four patients underwent surgical resection of pancreatic disease and 5 were treated with palliative intent.
Prior to commencement of treatment pathways, each patient was discussed in the multidisciplinary team setting and their radiological imaging reviewed. The main local factors determining resectability of the pancreatic lesion were the absence of arterial involvement and of peritoneal dissemination. Venous involvement was not a contraindication. Additional factors determining suitability for surgery included the presence, and severity of extrapancreatic metastases, co-morbid disease, performance status with regards to fitness for anaesthesia, and patient choice.
Patients with multi-site disease, with no option for resection, were referred for chemotherapy.
Operative Group
The demographics and management of colorectal disease prior to the development of CRPM are summarised in Table 1. The median age was 64 years with 3 of 4 patients being male. In all 4 cases, pancreatic metastases were identified on routine annual CT surveillance in patients who were not experiencing symptoms of pancreatic disease. The median time interval between diagnosis of CRC and CRPM was 6 years (range: 1-7 years). Three of the patients had metastatic disease at presentation of CRC including 2 with liver, and 1 with lung metastasis. These lesions were treated successfully by means of resection prior to the identification of CRPM. At the time of making a decision for resection of CRPM, none of the 4 patients had known extra-pancreatic disease.
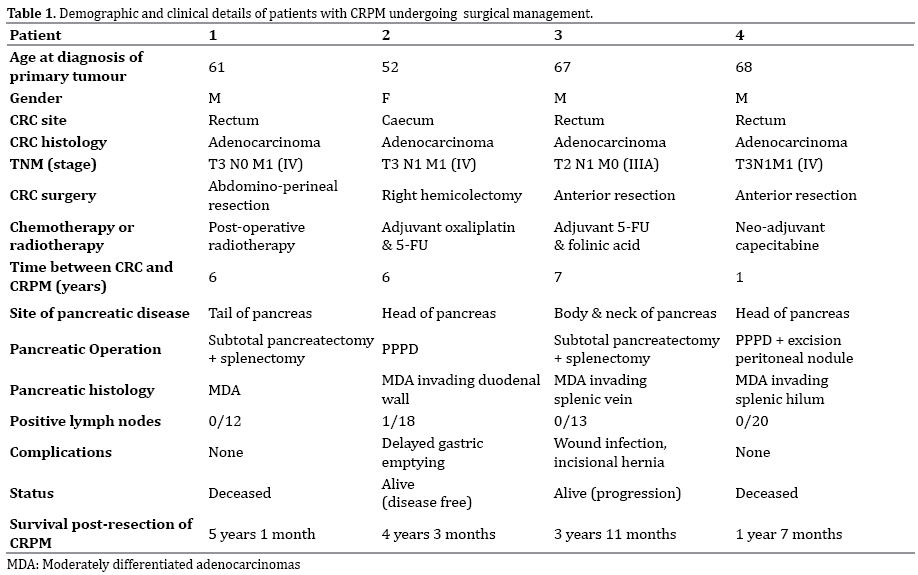
Two patients underwent distal pancreatectomy. Both of these cases necessitated splenectomy; one due to invasion of the splenic vein and one due to tumour spread to the splenic hilum. The latter patient was also found to have a single large (2 x 3 cm) peritoneal metastasis, identified during surgery that had not been appreciated on pre-operative imaging. The other 2 patients required a pylorus-preserving pancreatoduodenectomy (PPPD). Histologically, the CRPMs were all moderately differentiated adenocarcinomas (MDAs), corresponding morphologically to the CRC. At the time of the diagnosis in these patients routine biopsy and specific immunostaining was not performed in our centre to confirm histological diagnosis of primary prior to surgery. More recently, in line with national guidelines we perform endoscopic ultrasound (EUS) in the assessment of pancreatic metastasis to establish tissue diagnosis prior to surgery.
Surgical morbidity consisted of one case of delayed gastric emptying requiring nasojejunal feeding, with normal feeding being resumed by three months. One patient’s recovery was affected by wound infection and later by an incisional hernia.
One patient is alive and disease free at 4 years 3 months, and a second is alive with recurrent disease at 3 years and 11 months. Two patients died of disease recurrence at 1 year 7 month, and 5 years 1 month respectively.
Non-operative Group
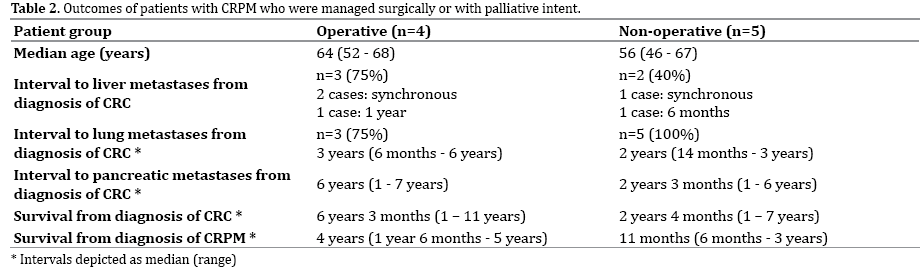
The median age of patients in the unresected group was 56 years. The median interval between diagnosis of CRC and CRPM was 2 years 3 months (range 1-6 years). Each of these patients underwent treatment with chemotherapy for CRC, with variation in the regimens used. Palliative management of CRPM included biliary stent insertion in one patient and percutaneous transhepatic cholangiography in another. All 5 patients were also affected by pulmonary metastases. Additional disease burden included 2 cases of liver metastases, 1 case of spine metastases and 1 patient who developed metastases of the brain and kidney.
Presently there are no disease free subjects with all 5 of these patients dying of recurrent or disseminated disease. The median survival from diagnosis of CRPM and death was 11 months years (range 6 months - 3 years).
Analysis of Operative and Non-operative Groups
In observing the 2 groups (Table 2), the proportion of patients with liver metastases was greater in the resected group (75% versus 40%) as was the proportion of synchronous metastasis (66% versus 50%). However, the distribution of liver disease in those who subsequently underwent resection of CRPM was amenable to resection whereas in those in whom the CRPM managed nonoperatively, the liver disease was not resectable. Likewise lung metastases developed earlier in the non-operative CRPM group and were not suitable for resection.
DISCUSSION
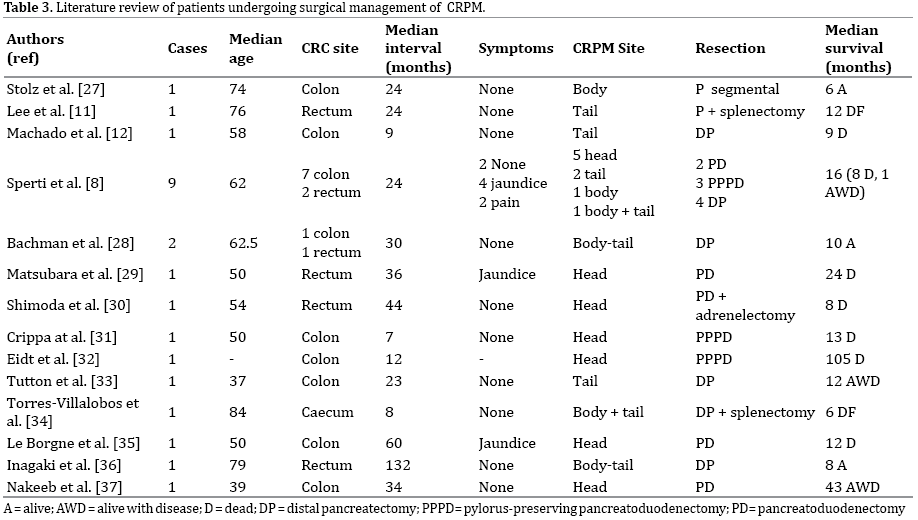
This study compares the outcome of patients undergoing surgical resection of CRPM versus non-operative management. The small series reflects the uncommon nature of CRPMs with the literature comprising mainly of case reports and small case series; the largest featuring 9 patients [8] (Table 3). A retrospective study of 546 pancreatic resections found 3.2% of these to be performed for metastatic disease, of which 1.6% originated from the colon or rectum [8] (Table 3). This figure is comparable to a previous series from Boston that showed pancreatic metastases to account for approximately 2% of all pancreatic resections [9]. A 2009 review of individual case series estimated CRC to be the pathological diagnosis in 7.8% of patients undergoing pancreatic metastatectomy [10]. Two recent reviews have identified between them a total of 31 patients that have undergone resection of pancreatic metastases from either the colon or rectum [11, 12].
Metastatic Spread of CRC
In each case, metastatic spread to other tissues occurred prior to identification of pancreatic involvement. This corresponds with autopsy findings where pancreatic lesions were observed in 3-12% of patients who had diffuse metastatic disease [13]. The appropriate management of patients with CRPM may depend on the degree of additional tumour burden, whereby patients with widespread disease are less likely to be managed surgically. The variable time interval between primary disease and CRPM does not appear to correlate with the stage of CRC. However, patients in the non-operative group had a shorter interval between diagnosis of CRC and development of CRPM compared to the resected group (2 years 3 months versus 6 years, respectively), potentially suggesting more aggressive disease. Although metastatic spread of CRC prior to the diagnosis of CRPM was identified in both groups.
In this series, pancreatic disease amenable to potentially curative treatment was detected on routine CT surveillance as per the hospital protocol after CRC. The time interval between CRC and CRPM emphasises the importance of continued surveillance scanning beyond 5 years of initial CRC diagnosis. Patients in this series had no symptoms suggestive of pancreatic disease at the time of identification. Other series have reported patients with pancreatic metastases from any primary source to be asymptomatic in up to 69% of cases [14, 15].
An interesting histopathological finding was the identification of intraluminal extension of the metastasis in one of the cases. Extension of tumour into the lumen of the main pancreatic duct is frequently seen in association with pancreatic ductal adenocarcinoma due to the intimate anatomical relationship between the tumour and the duct. The potential for intraluminal growth of acinar cell tumours of the pancreas [16-20] is also well appreciated with tumour extension within the main pancreatic identified by Ban and colleagues in 7/13 (54%) of their patients [20], and a separate pathologic entity being recognised. In terms of metastatic pancreatic lesions, with tumour extension into the main pancreatic duct has been recorded in 3 patients with renal metastases [21-23] but not for other metastatic lesions.
Surgical Management
Pancreatic resections have traditionally been associated with high rates of morbidity and mortality, although it is widely accepted that safety is improving. Recent data suggests mortality of 2.6% and morbidity of 27.1% for pancreatoduodenectomies being conducted for any cause [24]. In this series we have observed complications similar to those following pancreatic resection for primary pancreatic adenocarcinoma.
There has been debate in the literature as to the extent of pancreatic resection appropriate for metastatectomy.
No patient in this series developed local pancreatic recurrence implying adequacy of the pancreatic resection. The proposed advantages of limited resections for small pancreatic masses, such as enucleation, include reduced short and long-term morbidity [25]. In the present series local resection was precluded due to invasion of adjacent structures or proximity of the metastases to the pancreatic duct. Furthermore one patient had metastases to the peri-pancreatic lymph nodes. Other studies have recorded lymph node involvement to be 30% and 26% [8,10]. As such, lymphadenectomy (peripancreatic, station 8 and 9 lymph node groups) should be performed during pancreatic resection of CRPM.
Colorectal pancreatic metastases do not appear to occur in isolation; all patients in this series suffered extrapancreatic metastatic disease. It is not surprising therefore, that the majority of patients following pancreatic resection of CRPM developed recurrent metastatic spread.
We have demonstrated in the operative group that outcomes of surgery for CRPM are comparable to results seen following hepatic or pulmonary resection [4-7,26]. An aggregate analysis of patients with CRPM in isolated cases (n=10) showed the median survival to be 4 years 6 months (1-9 years) with 5-year survival of 29% following metastatectomy [10].
Given the rare nature of CRPM, cases should be referred to a specialist service for consideration of pancreatic resection, taking into account tumour resectability on imaging, control of the primary CRC, presence of extrapancreatic metastases, and co-morbid diseases.
This series suggests that pancreatic involvement is a late feature of CRC, with metastatic spread to other organs occurring in the interim. However, the lack of morbidity, and the potential for cure or effective palliation demonstrated in this series, supports the surgical management of CRPM where possible. There may be a cohort of unreported cases who would benefit from referral to specialist centres to determine their suitability for surgical resection. Future studies such as those using omic technologies (i.e. genomic, transcriptomic, and proteomic) are warranted in determining specific tumour biology characteristics and adding to current selection strategies in facilitating better outcomes of surgical resection for CRPM.
Funding
None
Ethical approval
Not needed
Contributors
GMS, AS and SF designed the project. LCM and JKR sourced and analysed the case notes. LCM and SF wrote the initial draft. All authors edited the manuscript. Statistics not applicable.
Conflicts of Interest
The authors have no conflicts or disclosures.
References
- Nakamura E, Shimizu M, Itoh T, Manabe T. Secondary tumors of the pancreas: clinicopathological study of 103 autopsy cases of Japanese patients. Pathol Int. 2001; 51:686-90. [PMID:11696171]
- Adsay NV, Andea A, Basturk O, Kilinc N, Nassar H, Cheng JD. Secondary tumors of the pancreas: an analysis of a surgical and autopsy database and review of the literature. Virchows Arch. 2004; 444:527-35. [PMID:15057558]
- Turk PS, Wanebo HJ. Results of surgical treatment of nonhepatic recurrence of colorectal carcinoma. Cancer. 1993; 71:4267-77. [PMID:8508389]
- Berri RN, Abdalla EK. Curable metastatic colorectal cancer: recommended paradigms. Curr Oncol Rep. 2009; 11:200-8. [PMID: 19336012]
- Abdalla EK. Resection of colorectal liver metastases. J Gastrointest Surg. 2011; 15:416-9. [PMID: 21301986]
- Shimada H, Tanaka K, Endou I, Ichikawa Y. Treatment for colorectal liver metastases: a review. Langenbecks Arch Surg. 2009; 394:973-83. [PMID:19582473]
- Kawazuma Y, Tanaka H, Tsukuma H, Ajiki W, Oshima A. Improvement of survival over time for colon cancer patients by anatomical sub-sites. Jpn J Cancer Res. 1999; 90:705-10. [PMID:10470281]
- Sperti C, Pasquali C, Berselli M, Frison L, Vicario G, Pedrazzoli S. Metastasis to the pancreas from colorectal cancer: is there a place for pancreatic resection? Dis Colon Rectum. 2009; 52:1154-9. [PMID:19581861]
- Z'Graggen K, Fernandez-del Castillo C, Rattner DW, Sigala H, Warshaw AL. Metastases to the pancreas and their surgical extirpation. Arch Surg. 1998; 133:413-7. [PMID:9565122]
- Reddy S, Wolfgang CL. The role of surgery in the management of isolated metastases to the pancreas. Lancet Oncol. 2009; 10:287-93. [PMID:19261257]
- Lee CW, Wu RC, Hsu JT, Yeh CN, Yeh TS, Hwang TL, et al. Isolated pancreatic metastasis from rectal cancer: a case report and review of literature. World J Surg Oncol. 2010; 8:26. [PMID:20374636]
- Machado NO, Chopra PJ, Al Hamdani A. Pancreatic metastasis from colon carcinoma nine years after a hemicolectomy managed by distal pancreatectomy. A review of the literature regarding the role and outcome of pancreatic resection for colorectal metastasis. JOP. 2010; 11:377-81. [PMID:20601814]
- Showalter SL, Hager E, Yeo CJ. Metastatic disease to the pancreas and spleen. Semin Oncol. 2008; 35:160-71. [PMID:18396201]
- Hiotis SP, Klimstra DS, Conlon KC, Brennan MF. Results after pancreatic resection for metastatic lesions. Ann Surg Oncol. 2002; 9:675- 9. [PMID:12167582]
- Le Borgne J, Partensky C, Glemain P, Dupas B, de Kerviller B. Pancreaticoduodenectomy for metastatic ampullary and pancreatic tumors. Hepatogastroenterology. 2000; 47:540-4. [PMID:10791233]
- Fabre A, Sauvanet A, Flejou JF, Belghiti J, Palazzo L, Ruszniewski P, et al. Intraductalacinar cell carcinoma of the pancreas. Virchows Arch. 2001; 438:312-5. [PMID:11315630]
- Hashimoto M, Matsuda M, Watanabe G, Mori M, Motoi N, Nagai K, et al. Acinar cell carcinoma of the pancreas with intraductal growth: report of a case. Pancreas. 2003; 26:306-8. [PMID:1265759]
- Yamaguchi R, Okabe Y, Jimi A, Shiota K, Kodama T, Naito Y, et al. Pancreatic acinar cell carcinoma extending into the common bile and main pancreatic ducts. Pathol Int. 2006; 56:633-7. [PMID:16984622]
- Basturk O, Zamboni G, Klimstra DS, Capelli P, Andea A, Kamel NS, et al. Intraductal and papillary variants of acinar cell carcinomas: a new addition to the challenging differential diagnosis of intraductal neoplasms. Am J Surg Pathol. 2007; 31:363-70. [PMID:17325477]
- Ban D, Shimada K, Sekine S, Sakamoto Y, Kosuge T, Kanai Y, et al. Pancreatic ducts as an important route of tumor extension for acinar cell carcinoma of the pancreas. Am J Surg Pathol. 2010; 34:1025-36. [PMID:20534994]
- Abbas MA, Collins JM, Mulligan DC. Renal cell carcinoma metastatic to pancreas. Am J Surg. 2001; 182:183-4. [PMID:11574093]
- Yachida S, Fukushima N, Kanai Y, Nimura S, Shimada K, Yamamoto J, et al. Pancreatic metastasis from renal cell carcinoma extending into the main pancreatic duct: a case report. Jpn J Clin Oncol. 2002; 32:315-7. [PMID:12411571]
- Hijioka S, Hifumi M, Mekky MA, Takekuma Y, Kawaguchi T, Yokomizo H, et al. Total pancreatectomy for metastatic renal cell carcinoma with marked extension into the main pancreatic duct. Intern Med. 2010; 49:557-62. [PMID:20228590]
- Kelly KJ, Greenblatt DY, Wan Y, Rettammel RJ, Winslow E, Cho CS, et al. Risk stratification for distal pancreatectomy utilizing ACS-NSQIP: preoperative factors predict morbidity and mortality. J Gastrointest Surg. 2011; 15:250-9. [PMID:21161427]
- Bassi C, Butturini G, Falconi M, Sargenti M, Mantovani W, Pederzoli P. High recurrence rate after atypical resection for pancreatic metastases from renal cell carcinoma. Br J Surg. 2003; 90:555-9. [PMID:12734861]
- Gomez D, Sangha VK, Morris-Stiff G, Malik HZ, Guthrie AJ, Toogood GJ, et al. Outcomes of intensive surveillance after resection of hepatic colorectal metastases. Br J Surg. 2010; 97:1552-60. [PMID:20632325]
- Stoltz A, Plok V, Ducerf C, Baulieux J, Mabrut JY. A pancreatic metastasis from a colorectal cancer. Clin Res Hepatol Gastroenterol. 2011; 35:586-9. [PMID:21397584]
- Bachmann J, Michalski CW, Bergmann F, Buchler MW, Kleef J, Friess H. Metastasis of rectal adenocarcinoma to the pancreas: two case reports and a review of the literature. JOP. 2007; 8:214-22. [PMID:17356246]
- Matsubara N, Baba H, Okamoto A, Kurato M, Tsuruto K, Funata N, Ashizawa K. Rectal cancer metastasis to the head of the pancreas treated with pancreaticoduodenectomy. J Hepatobiliary Pancreat Surg. 2007; 14:590-4. [PMID:18040627]
- Shimoda M, Kubota K, Kita J, Katoh M, Iwaski Y: Is a patient with metastatic pancreatic tumor from rectal cancer a candidate for resection? Hepatogastroenterology. 2007; 54:1262-5. [PMID:17629084]
- Crippa S, Angelini M, Mussi C, Bonardi C, Romano F, Sartori P, Uggeri F, Bovo G. Surgical treatment of metastatic tumors to the pancreas: a single-centre experience and review of the literature. World J Surg. 2006; 30:1536-42. [PMID:168447716]
- Eidt S, Jergas M, Schmidt R, Siedek M. Metastasis to the pancreas-an indication for pancreatic resection? Langenbecks Arch Surg. 2007; 392:539-42. [PMID:17242893]
- Tutton MG, George M, Hill ME, Abulafi AM. Solitary pancreatic metastasis from a primary colonic tumor detected by PET scan: report of a case. Dis Colon Rectum. 2001; 44:288-90. [PMID:11227949]
- Torres-Villalobos G, Podgaetz E, Anthon FJ, Remes-Trocheb JM, Robles-Doaz J, NuDez CC. Single pancreatic metastasis from a previously resected carcinoma of the caecum: a case report. Curr Surg. 2004; 61:328- 30. [PMID:15165777]
- Le Borgne J, Partensky C, Glemain P, Dupas B, de Kervillier B. Pancreaticoduodenectomy for metastatic ampullary and pancreatic tumors. Hepatogastroenterology. 2000; 47:540-4. [PMID:10791233]
- Inagaki H, Nakao A, Ando N, Kotake K, Imaizumi T, Okuda N, Kaneko T, Kurokawa T, Nonami T, Tagaki H. A case report of solitary metastatin pancreatic cancer from rectal carcinoma: a case report. Hepato-gastroenterology. 1998; 45:2413-7. [PMID:1951934]
- Nakeeb A, Lillemoe KD, Cameron JL. The role of pancreaticoduoendectomy for locally recurrent or metastatic carcinoma to the periampullary region. J AM Coll Surg. 1995; 180:180-2. [PMID:7850053]

