Sun Young Oh1, Nawal Wasif2, Marie Carmel Garcon3, Gladys Rodriguez3 and Muhammad Wasif Saif1*
1Department of Hematology/Oncology and Experimental Therapeutics, Tufts University School of Medicine. Boston, MA, USA.
2Brookline High School. Brookline, MA, USA.
3Columbia University Medical Center. New York, NY, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Section of GI Cancers and Experimental Therapeutics
Tufts University School of Medicine
800 Washington Street; Boston, MA 02111
USA
Phone +1-617.636.5627
Fax +1-617.636.8535
E-mail wsaif@tuftsmedicalcenter.org
Received June 5th, 2013 – Accepted August 2nd, 2013
Keywords
Deafness; Hearing Loss; oxaliplatin; Pancreatic Neoplasms; Peripheral Nervous System Diseases
INTRODUCTION
Oxaliplatin is a third-generation diamine cyclohexane platinum derivative which mechanism of action involves the formation of DNA adducts and inhibition of the DNA synthesis [1]. The clinical development of oxaliplatin-based chemotherapy regimens started in the 1990s and along the years, several different combination regimens have been used in oncology [2]. Oxaliplatin is widely used for the treatment of various solid organ malignancies including colorectal cancer, pancreatic cancer, upper gastrointestinal cancer, hepatobiliary cancer, and ovarian cancer. In pancreatic cancer, oxaliplatin is used in combination with 5-fluorouracil, leucovorin and irinotecan (FOLFIRINOX) for patients with metastatic disease [3].
While neurotoxicity is a frequently reported sideeffect of oxaliplatin (76%) [1], it displays a characteristic pattern; an acute onset neuropathy which may occur immediately after infusion, characterized by cold-exacerbated paresthesia, muscle spasm and fasciculation. These acute symptoms typically resolve within a week, but, at higher cumulative doses, oxaliplatin induces doselimiting sensory neuropathy and leads to persistent functional impairment and even ataxia [2]. Among patients who received oxaliplatin for duration of 5-7 months, such neurotoxic adverse reaction occurs approximately in 50% [2]. Other major oxaliplatin related side effects include fatigue, diarrhea, nausea, vomiting, stomatitis and abdominal pain [1].
Ototoxicity related to the use of platinum derivatives, especially cisplatin has been well documented. However, development of ototoxicity after use of oxaliplatin is very rare, less than 1% of patients. Here we present a case of a female patient who developed hearing loss after receiving oxaliplatin and gemcitabine (Gem-Ox) for locally advanced, unresectable pancreatic cancer.
Case report
An 85-year-old Caucasian woman presented initially with a 3-month history of decreased appetite, nausea, vomiting, weight loss, and fatigue. Her past medical history was significant for hypertension, diabetes mellitus, presbycusis, cataract, and glaucoma. She had an ultrasound of the abdomen and it revealed a 2.8 cm mass at the head of pancreas. A CT scan of abdomen and pelvis showed 2.9 cm mass at the head of pancreas as well as pancreatic ductal dilatation, and the tumor was found to encompass approximately 50% of the celiac axis and 50% of the superior mesenteric vein. The biopsy confirmed adenocarcinoma. Because of her locally advanced unresectable pancreatic cancer, neoadjuvant chemotherapy was initiated with oxaliplatin (85 mg/m2) and gemcitabine (1,000 mg/m2) given at day 1 which was repeated every 14 days (same day oxaliplatin and gemcitabine) [4, 5]. The patient had a history of moderate to severe bilateral presbycusis necessitating her to wear and use a hearing aid for more than 32 years.
At the end of third cycle (cumulative dose: 85 x 3 = 255 mg/m2), the patient noticed further difficulty in hearing. An audiogram was obtained as shown below in Figure 1.
Figure 1. Post-oxaliplatin audiogram.
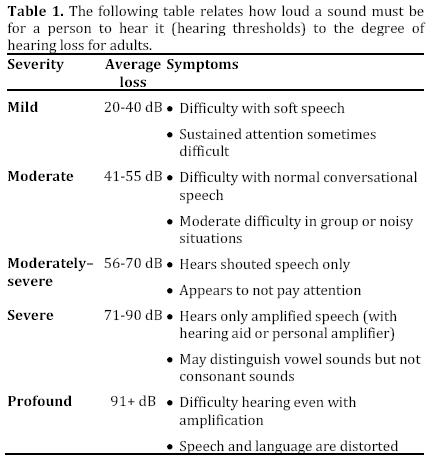
The audiogram showed that the speech recognition threshold was decreased from 55 dB to 85 dB when compared to baseline audiogram (Figure 2).
Figure 2. Pre-oxaliplatin audiogram.
This change confirmed her to progress from moderate to profound hearing loss as depicted in Table 1. The patient denied vertigo, tinnitus, or any other cranial nerve symptoms.
Her pancreatic tumor clearly responded to same day oxaliplatin and gemcitabine by CT scan, which showed 15.6% decrease in size after fourth cycle. Also her CA 19-9 level was reduced by 60%. Therefore her treatment was continued with dose reduction of oxaliplatin from 85 mg/m2 to 65 mg/m2 starting from fourth cycle. We added calcium and magnesium salts pre- and postoxaliplatin infusion [6, 7]. Her hearing aid was upgraded.
The patient completed a total of 10 cycles of same day oxaliplatin and gemcitabine with cumulative dose of 710 mg/m2 (85 x 3 = 255 mg/m2 plus 65 x 7 = 455 mg/m2), followed by one-month duration of chemoradiation therapy with capecitabine. Repeat imaging was obtained after completion of chemoradiation therapy and it showed further decrease in size of the tumor from 2.9 cm initially to 1.4 cm. Given the potential need for an arterial reconstruction in case of a surgery, the patient was not considered to be a surgical candidate and her chemotherapeutic regimen was changed to single agent therapy with gemcitabine. Her further clinical course was complicated by severe neutropenia leading to interruptions in therapy and subsequent dose reduction. However, her hearing remained unchanged. Follow-up CT scans revealed stable disease status and improvement in vascular involvement of the tumor.
Discussion
Platinum-based chemotherapeutic agents are widely used in various malignancies including pancreatic cancer [8]. However, like other chemotherapeutic agents, they have significant adverse effects that commonly limit their therapeutic use. Oxaliplatin is a third generation cisplatin analog and it is considered to be far less nephrotoxic and ototoxic compared to cisplatin or carboplatin [2].
The main targets of the platinum derivative-related ototoxicity are the outer hair cells in the organ of Corti and the vascularized epithelium in the lateral wall of the cochlea, the stria vascularis [9]. The organ of Corti is protected by a blood-labyrinth barrier that restricts the entry of platinum derivatives to the perilymphatic compartment of the inner ear. Disruption of this blood-labyrinth barrier by a loop diuretic or noise exposure enhances the entry of the drug to the inner ear perilymphatic compartment and can potentiate the amount of damage [10]. Among three platinum derivatives in clinical use, cisplatin is considered as the most ototoxic agent. It was proposed that the major difference in the ototoxic profile of various platinum compounds might arise from several different metal transporters that selectively regulate the influx, efflux and sequestration of these drugs [10]. In this regard, recent pharmacokinetic studies have revealed that the cochlear uptake of oxaliplatin is considerably less than the uptake of cisplatin that may explain their different ototoxic profiles [9].
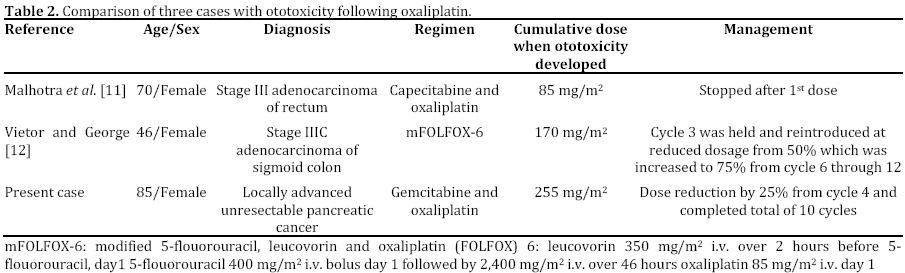
To the best of our knowledge, this is the third case report of oxaliplatin-induced ototoxicity as shown in Table 2 [11, 12]. Previously, Malhotra et al. have reported a case of acute unilateral ototoxicity following a single intravenous infusion of oxaliplatin that was minimally improved after 2 years of follow-up [11]. Vietor and George have described a case of oxaliplatin-induced ototoxicity and transient hepatotoxicity [12].
Ototoxicity seems to be a rare complication of oxaliplatin therapy. Therefore, it is difficult to generalize the guidance in regard to the prediction of the ototoxic side effect from this drug. Our patient and the patient in the report by Vietor and George [12] were not taking known ototoxic medication including loop diuretics. All three subjects in reported cases are female and it appears that the ototoxicity occurs at lower cumulative dosage compare to neuropathy which occurs in 10- 15% of patients after a cumulative dose of 780 to 850 mg/m2 [13]. Regardless of its rare occurrence, clinicians should be aware of this severe complication and be diligent in monitoring patients' clinical symptoms. We suggest in patients with known risk factors for hearing problems, prior exposure to ototoxic drugs, or planned treatment at high doses, hearing monitoring should be considered. Further research to define the potential for ototoxicity using this chemotherapy is warranted.
Conflict of interest
The authors have no potential conflict of interest
References
- Ibrahim A, Hirschfeld S, Cohen MH, Griebel DJ, Williams GA, Pazdur R. FDA drug approval summaries: oxaliplatin. Oncologist. 2004; 9(1): 8-12.
- Hoff PM, Saad ED, Costa F, Coutinho AK, Caponero R, Prolla G, Gansl RC. Literature review and practical aspects on the management of oxaliplatin-associated toxicity Clin Colorectal Cancer. 2012 Jun; 11(2): 93-100.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la Fouchardière C, Bennouna J, Bachet JB, Khemissa-Akouz F, Péré-Vergé D, Delbaldo C, Assenat E, Chauffert B, Michel P, Montoto-Grillot C, Ducreux M; Groupe Tumeurs Digestives of Unicancer; PRODIGE Intergroup. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011 May 12; 364(19): 1817-25.
- Li J, Merl M, Lee MX, Kaley K, Saif MW. Safety and efficacy of single-day GemOx regimen in patients with pancreatobiliary cancer: a single institution experience. Expert Opin Drug Saf. 2010 Mar; 9(2): 207-13.
- Afchain P, Chibaudel B, Lledo G, Selle F, Bengrine-Lefevre L, Nguyen S, Paitel JF, Mineur L, Artru P, André T, Louvet C. First-line simplified GEMOX (S-GemOx) versus classical GEMOX in metastatic pancreatic cancer (MPA): results of a GERCOR randomized phase II study. Bull Cancer. 2009 May; 96(5): E18-22.
- Saif MW, Reardon J. Management of oxaliplatin-induced peripheral neuropathy. Ther Clin Risk Manag. 2005 Dec; 1(4): 249-58.
- Saif MW. Oral Calcium Ameliorating Oxaliplatin-Induced Peripheral Neuropathy. J Appl Res. 2004 Jan 1; 4(4): 576-582.
- Saif MW, Kim R. Role of platinum agents in the management of advanced pancreatic cancer. Expert Opin Pharmacother. 2007 Nov; 8(16): 2719-27.
- Hellberg V, Wallin I, Eriksson S, Hernlund E, Jerremalm E, Berndtsson M, Eksborg S, Arnér ES, Shoshan M, Ehrsson H, Laurell G. Cisplatin and oxaliplatin toxicity: importance of cochlear kinetics as a determinant for ototoxicity. J Natl Cancer Inst. 2009 Jan 7; 101(1): 37-47.
- Ding D, Allman BL, Salvi R. Review: ototoxic characteristics of platinum antitumor drugs . Anat Rec (Hoboken). 2012 Nov; 295(11): 1851-67.
- Malhotra NK, Aslam R, Lipman SP, Bilski VJ. Acute ototoxicity from a single infusion of oxaliplatin. Ear Nose Throat J. 2010 Jun; 89(6): 258-61.
- Vietor NO, George BJ. Oxaliplatin-induced hepatocellular injury and ototoxicity: a review of the literature and report of unusual side effects of a commonly used chemotherapeutic agent. J Oncol Pharm Pract. 2012 Sep; 18(3): 355-9.
- Cassidy J, Misset JL Oxaliplatin-related side effects: characteristics and management. Semin Oncol. 2002 Oct; 29(5 Suppl 15): 11-20.



