Muhammad Wasif Saif
Yale Cancer Center, Yale University School of Medicine. New Haven, CT, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Yale Cancer Center, Yale University School of Medicine, 333
Cedar Street, FMP 116, New Haven, CT, USA
Phone: +1-203.737.1569
Fax: +1-203.785.3788
E-mail: wasif.saif@yale.edu
Received: 19 March, 2010 Accepted: 22 March, 2010
Keywords
erlotinib; gemcitabine; Pancreatic Neoplasms; Salvage Therapy; Treatment Failure
Dear Sir,
We read with interest the review article by Gounaris et al. entitled ‘Options for the Treatment of Gemcitabine- Resistant Advanced Pancreatic Cancer’, published in the March issue of JOP. J Pancreas (Online) [1]. The authors searched the OVID and MEDLINE databases from 1950 to present using the MeSH terms "pancreatic neoplasms", "drug treatment", and "gemcitabine". In addition to 31 published studies identified, these results were supplemented by abstracts published in the last three (2007-2009) American Society of Clinical Oncology (ASCO) proceedings of annual meetings. They found that the evidence for second line treatments of metastatic pancreatic cancer consists mainly of single arm, small phase II studies. Only oxaliplatin-fluoropyrimidine combinations have been compared against supportive care and seem promising. However, we will add that oral capecitabine seems to be a very convenient and an optimal therapy too [2].
We agree with the authors that there is growing evidence supporting benefit of chemotherapy after gemcitabine failure in selected patients with good performance status as we published similar data earlier in JOP. J Pancreas (Online) [2]. Lack of data to support second-line treatment strategy in advanced pancreatic cancer is probably due to the fact that we still do not have an effective first-line treatment that renders true survival benefit [3]. In order to establish a much needed effective second-line treatment options for advanced pancreatic cancer, we need cooperative efforts among institutions and community practices in enrolling gemcitabine refractory patients in clinical trials. Moreover, development of novel therapeutic agents should be an obvious area of our focus in the future. We must improve study design and be more rigorous in scrutinizing phase II data before moving forward with large phase III randomized trials that require enormous resources. One solution would be more frequent implementation of randomized phase II trials to test agents with encouraging activities before undertaking phase III trials.
Patient selection and individualized medicine is another area of increased interest at present. While it is still at a very early stage before we can see clinical application, pharmacogenomics in pancreatic cancer is an important area to watch. There are various preclinical studies investigating polymorphisms and expression levels of genes associated with gemcitabine sensitivity and/or resistance [4].
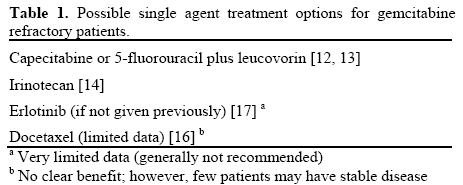
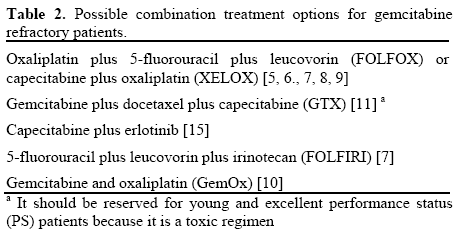
In brief, selected advanced pancreatic cancer patients with good performance status should be considered for second-line chemotherapy after first-line gemcitabine failure. With better patient selection, we can improve clinical outcomes of advanced pancreatic cancer in second-line settings, which will ultimately improve the over all survival. It is also important to consider the quality of life measurements in this setting as obviously patients are more symptomatic when receiving second-line chemotherapy. Prospective clinical trials investigating clinical outcomes in association with published prognostic factors such as performance status, C-reactive protein, and peritoneal dissemination may improve patient selection for second-line treatment as we previously suggested (Figure 1; Tables 1 and 2).
Figure 1: Proposed selection guideline for second-line therapy after
gemcitabine failure [2].
ECOG: Eastern Cooperative Oncology Group; PS: performance
status
Conflict of Interest
The authors declare no conflicts of interest
References
- Gounaris I, Zaki K, Corrie P. Options for the treatment of gemcitabine-resistant advanced pancreatic cancer. JOP. J Pancreas (Online) 2010; 11:113-23. [PMID 20208317]
- Kang SP, Saif MW. Optimal second line treatment options for gemcitabine refractory advanced pancreatic cancer patients. Can we establish standard of care with available data? JOP. J Pancreas (Online) 2008; 9:83-90. [PMID 18326918]
- Li J, Merl MY, Saif MW. Any second-line therapy for advanced pancreatic cancer? Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP. J Pancreas (Online) 2010; 11:151-3. [PMID 20208325]
- Strimpakos AS, Syrigos KN, Saif MW. Pharmacogenetics in pancreatic cancer. Highlights from the 45th ASCO annual meeting. Orlando, FL, USA. May 29-June 2, 2009. JOP. J Pancreas (Online) 2009; 10:357-60. [PMID 19581734]
- Novarino A, Satolli MA, Chiappino I, Giacobino A, Bellone G, Rahimi F, et al. Oxaliplatin, 5-fluorouracil, and leucovorin as second-line treatment for advanced pancreatic cancer. Am J Clin Oncol 2009; 32:44-8. [PMID 19194124]
- Tsavaris N, Kosmas C, Skopelitis H, Gouveris P, Kopterides P, Loukeris D, et al. Second-line treatment with oxaliplatin, leucovorin and 5-fluorouracil in gemcitabine-pretreated advanced pancreatic cancer: A phase II study. Invest New Drugs 2005; 23:369-75. [PMID 16012797]
- Hwang J, Yoo C, Kim T, Lee J, Park D, Seo D, et al. A randomised phase II trial of FOLFOX or FOLFIRI.3 as second-line therapy in patients with advanced pancreatic cancer previously treated with gemcitabine-based chemotherapy. J Clin Oncol 2009; 27(15 Suppl.):4618.
- Xiong HQ, Varadhachary GR, Blais JC, Hess KR, Abbruzzese JL, Wolff RA. Phase 2 trial of oxaliplatin plus capecitabine (XELOX) as second-line therapy for patients with advanced pancreatic cancer. Cancer 2008; 113:2046-52. [PMID 18756532]
- Sancho A, Lopez-Vivanco G, Diaz de Corcuera I, Ferreiro J, Moreno A, Mielgo X, et al. Oxaliplatin and capecitabine after gemcitabine failure in patients with advanced pancreatic, biliary or gallbladder adenocarcinoma (APBC). J Clin Oncol 2008; 26:s15625.
- Demols A, Peeters M, Polus M, Marechal R, Gay F, Monsaert E, et al. Gemcitabine and oxaliplatin (GEMOX) in gemcitabine refractory advanced pancreatic adenocarcinoma: a phase II study. Br J Cancer 2006; 94:481-5. [PMID 16434988]
- Dakik HK, Moskovic DJ, Carlson PJ, Qiao W, Ho L, Tamm E, et al. Evaluation of gemcitabine, docetaxel, capecitabine (GTX) in previously treated pancreatic cancer. ASCO Gastrointestinal Cancers Symposium 2010. Abstract No. 221.
- Boeck S, Wilkowski R, Bruns CJ, Issels RD, Schulz C, Moosmann N, et al. Oral capecitabine in gemcitabine-pretreated patients with advanced pancreatic cancer. Oncology 2007; 73:221-7. [PMID 18424886]
- Saif MW, Li J, Lamb L, Rosenberg A, Elligers K, Ruta S, et al. A phase II study of capecitabine (CAP) plus PHY906 in patients (pts) with advanced pancreatic cancer (APC). J Clin Oncol 2009; 27(15 Suppl.):e15508.
- Yi SY, Park YS, Kim HS, Jun HJ, Kim KH, Chang MH, et al. Irinotecan monotherapy as second-line treatment in advanced pancreatic cancer. Cancer Chemother Pharmacol 2009; 63:1141-5. [PMID 18839175]
- Kulke MH, Blaszkowsky LS, Ryan DP, Clark JW, Meyerhardt JA, Zhu AX, et al. Capecitabine plus erlotinib in gemcitabinerefractory advanced pancreatic cancer. J Clin Oncol 2007; 25:4787- 92. [PMID 17947726]
- Cereda S, Reni M. Weekly docetaxel as salvage therapy in patients with gemcitabine-refractory metastatic pancreatic cancer. J Chemother 2008; 20:509-12. [PMID 18676234]
- Tang P, Gill S, Au HJ, Chen EX, Hedley D, Leroux M, et al. Phase II trial of erlotinib in advanced pancreatic cancer (PC). J Clin Oncol 2009; 27(15 Suppl.):4609.


