Keywords
Pancreatic Neoplasms; Salvage Therapy; Treatment Failure
Abbreviations
ASCO: American Society of Clinical Oncology; LV: leucovorin
INTRODUCTION
Since the birth of fluorouracil (5-FU) 50 years ago, we have made only incremental changes in clinical outcomes in pancreatic cancer. Gemcitabine remains to be the only standard of care in advanced pancreatic cancer since mid-1990s [1]. Numerous trials which enrolled thousands of patients failed to improve the outcome significantly beyond gemcitabine. At present time, data set in 2nd line setting is grossly limited. One reason is that most advanced pancreatic cancer patients who progress on their 1st line treatment are often poor candidates for clinical trials due to their worsening performance status. Lack of active agents seen in number of trials in 1st line is another limitation in advancing agents in 2nd line setting. The change of this rather dark landscape in 1st line setting is suggested by two recent large randomized phase III trials in advanced pancreatic cancer showing that addition of capecitabine or erlotinib to gemcitabine render superiority to single-agent gemcitabine [2, 3].
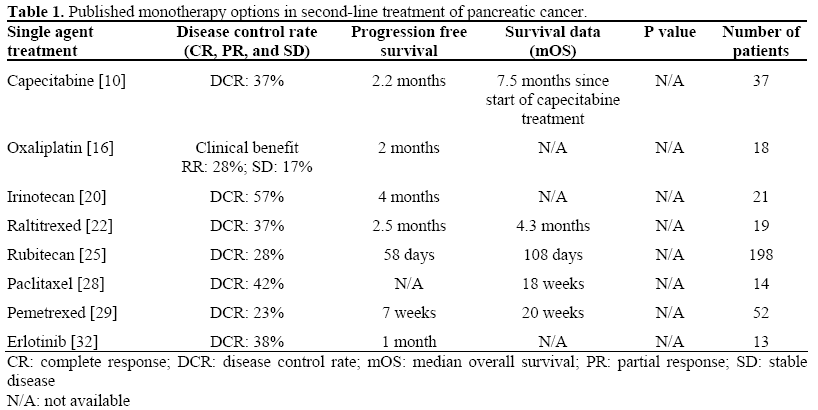
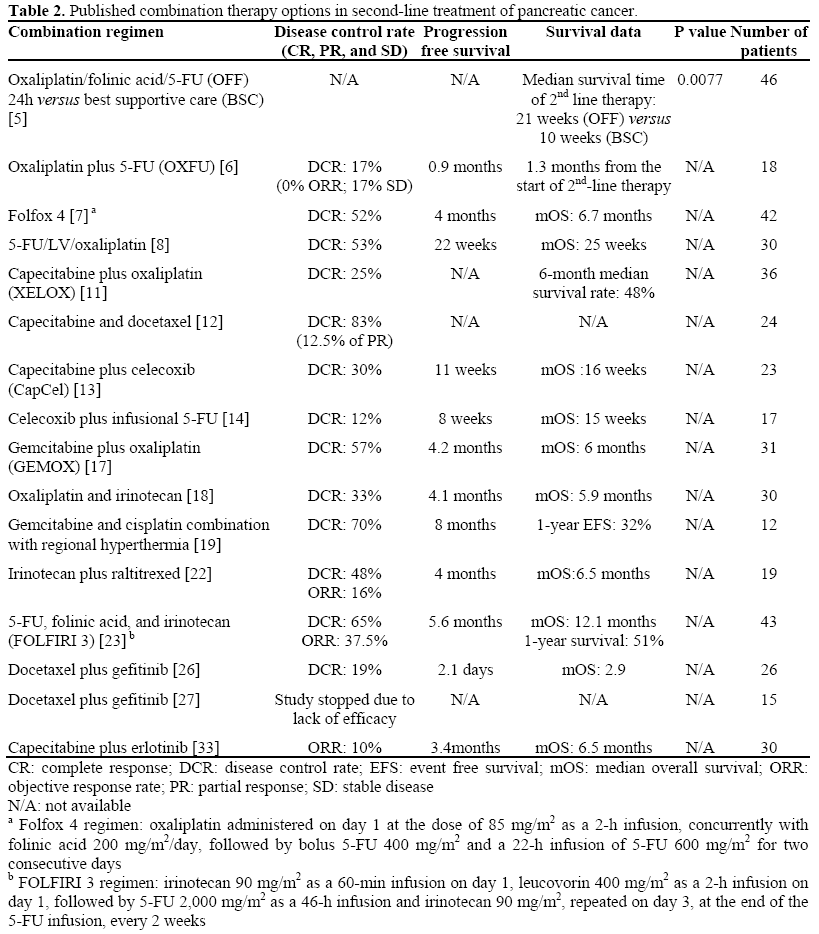
There is growing evidence supporting benefit of chemotherapy after gemcitabine failure in selected patients with good performance status (Tables 1 and 2) [4]. In order to establish a much needed effective 2nd line treatment options for advanced pancreatic cancer, we need cooperative efforts among institutions and community practices in enrolling gemcitabine refractory patients in clinical trials.
Cytotoxic Agents
Fluoropyrimidine
Single agent 5-FU has shown benefit over best supportive care in number of clinical trials in advanced pancreatic cancer and has been the standard of care for approximately 40 years until mid 1990’s when gemcitabine emerged as the new standard [1]. Response rates with 5-FU alone with or without leucovorin (LV) in various infusional modes in 1st line settings have been modest. Currently, there is no data supporting the use of 5-FU/LV alone in gemcitabine refractory advanced pancreatic cancer patients.
Clinical trials including phase III randomized trial proving that patients with refractory advanced pancreatic cancer benefit from salvage chemotherapy with 5-FU based regimen [5, 6]. Various combinations of 5- FU/LV/oxaliplatin were tested in advanced pancreatic cancer patients after gemcitabine failure and have shown promising disease control rates. A chemotherapy protocol consisting of oxaliplatin, 5-FU, and folinic acid (Folfox 4; oxaliplatin administered on day 1 at the dose of 85 mg/m2 as a 2-h infusion, concurrently with folinic acid 200 mg/m2/day, followed by bolus 5-FU 400 mg/m2 and a 22-h infusion of 5-FU 600 mg/m2 for two consecutive days) appears to be the most active regimen of this combination resulting in 52% disease control rates and 4 months progression free survival (Tables 1 and 2) [7, 8].
Capecitabine is an oral fluoropyrimidine which was tested in 1st line setting with clinical benefit response rate of 24%, suggesting possible role of capecitabine as a salvage therapy after gemcitabine failure [9]. Capecitabine as monotherapy or in combination with oxaliplatin (XELOX) has shown encouraging disease control rates in gemcitabine refractory patients [10, 11]. Capecitabine and docetaxel combination is also an active 2nd line treatment option with 71% of patients maintaining stable disease for 2 or more cycles (Tables 1 and 2) [12].
Lately, a novel combination of capecitabine plus celecoxib resulted in modest activity in 2nd line setting of advanced pancreatic cancer [13]. Celecoxib was also combined with protracted intravenous 5-FU in gemcitabine refractory advanced pancreatic cancer patients and shown modest activity suggesting synergy between fluoropyrimidine and celecoxib [14]. S-1 is a fourth generation oral fluoropyrimidine with a potential activity in pancreatic cancer in second line setting and needs further investigation (Tables 1 and 2) [15].
Platinum
Single agent oxaliplatin rendered a clinical response in 28% of advanced pancreatic cancer who progressed on gemcitabine [16].
Oxaliplatin in combination with 5-FU and capecitabine is a reasonable 2nd line treatment option in advanced pancreatic cancer as described in above section. Gemcitabine plus oxaliplatin (GEMOX) showed activity in 2nd line setting after gemcitabine failure. GEMOX regimen showed approximately 57% disease control rates with median time to progression of 4 months in a study by Demols et al. [17]. Cantore et al. also reported 20% clinical response rates with duration of 7.2 months using a combination of oxaliplatin and irinotecan in gemcitabine refractory advanced pancreatic cancer patients [18]. Gemcitabine and cisplatin combination with regional hyperthermia was evaluated in advanced pancreatic cancer patients after gemcitabine failure. This regimen, at interim analysis which was presented in the 2006 American Society of Clinical Oncology (ASCO) meeting, showed a potential although only 12 patients were evaluated at the time [19].
Topoisomerase Inhibitors
Irinotecan monotherapy is active as a 2nd line treatment of gemcitabine refractory advanced pancreatic cancer patients. Fifty-seven percent of patients had disease control with median time to progression of 4 months [20]. Preclinical study suggesting that pemetrexed and irinotecan may have synergistic activity in pancreatic cancer, and this regimen should be evaluated in 2nd line settings [21]. Irinotecan plus raltitrexed in gemcitabine refractory advanced pancreatic cancer patients resulted in an objective response rate of 16% and clinical benefit response of 29% [22]. Combination of 5-FU, folinic acid, and irinotecan (FOLFIRI) was tested in 1st line setting with promising activity and due to this regimen’s lack of cross-resistance with gemcitabine based 1st line treatment options, FOLFIRI may emerge as a reasonable 2nd line option in selected patients with good performance status [23]. Rubitecan is an orally active camptothecin derivative, and it has shown a moderate activity as a salvage therapy in heavily pretreated patients with advanced pancreatic cancer [24, 25].
Taxane
Docetaxel has been used in 1st and 2nd line setting in combination with irinotecan and biological agents. Ignatiadis et al. evaluated docetaxel/gefitinib combination as 2nd line treatment in patients with advanced pancreatic cancer after gemcitabine failure. Conclusion of this study was that the regimen, although safe, has no activity as salvage treatment for advanced pancreatic cancer after failure of gemcitabine-based chemotherapy [26]. Another study presented in the 2007 ASCO meeting confirmed inactivity of this combination [27].
Single agent weekly paclitaxel in 2nd and 3rd line setting after gemcitabine failure in a small study by Oettle et al. showed a modest activity. Paclitaxel monotherapy may be considered to be an additional treatment option in gemcitabine refractory pancreatic cancer [28].
Antimetabolites
Pemetrexed is a novel multitargeted antifolate that targets enzymes involved in folate metabolism. In a phase II trial with 52 patients who had progression of disease on gemcitabine, single agent pemetrexed resulted in a 3-month survival rate of 75%, disease control rate of 23% with time to progression of 7 weeks and decrease of CA 19-9 levels by more than 50% in 23% of treated patients [29].
Biological Agents
Vascular Endothelial Growth Factor (VEGF) Inhibition
Agents inhibiting VEGF pathways have been largely disappointing in 1st line setting thus far. Bevacizumab in combination with gemcitabine in randomized phase III clinical trial and sorafenib in a small pilot study have failed to show the superiority over gemcitabine monotherapy [30, 31]. Other combination regimen and novel agents should be investigated in 2nd line setting taking advantage of relatively low toxicity profile of these agents. Our experience in treating other cancer types with bevacizumab suggests that perhaps gemcitabine is not the ideal agent to combine bevacizumab with. Folfox, 5-FU, capecitabine, paclitaxel, and irinotecan have shown synergistic anti-tumor activities in randomized clinical trials, and these approaches should be further investigated in advanced pancreatic cancer.
Epidermal Growth Factor Receptor (EGFR)
Erlotinib monotherapy in 2nd line setting was tested in a small study with 13 patients evaluated. In this study 5 patients had disease control with time to progression of 1 month suggesting that erlotinib is an option for gemcitabine refractory patients with minimal toxicity [32].
Capecitabine plus erlotinib in gemcitabine refractory pancreatic cancer rendered an objective response rate of 10% with median progression free survival of 3.4 months in a recent trial of 30 patients. This study noted no association between clinical outcome and EGFR mutational status although the sample was small [33]. It would be interesting to see if patients with K-ras wild type gene would benefit more from erlotinib in 2nd line setting and should be investigated in future clinical trials. Docetaxel/gefitinib is not active in 2nd line as described in previous section [26, 27]. Docetaxel plus irinotecan plus cetuximab showed a promising activity as a nongemcitabine containing regimen and can potentially be use in 2nd line setting as well [34].
Hormonal Therapies
Tamoxifen monotherapy and octreotide monotherapy showed minimal activity in multiple clinical trials. Tamoxifen did not render survival advantage over placebo in clinical trials and octreotide in combination with 5-FU failed to show any benefit [35, 36, 37, 38]. Based upon these negative trials in 1st line setting, it is unlikely that these agents would have any benefit in 2nd line setting.
Future Direction
Lack of attention to 2nd line treatment strategy in advanced pancreatic cancer is due to the fact that we still do not have 1st line option that renders true survival benefit; therefore, development of novel therapeutic agents should be an obvious area of our focus in the future. However, it is equally important that we improve study design and be more rigorous in scrutinizing phase II data before moving forward with large phase III randomized trials that require enormous resources. One solution would be more frequent implementation of randomized phase II trials to test agents with encouraging activities before undertaking phase III trials.
Patient selection and individualized medicine has been the area of increased interest since human genome project was completed. While it is still at a very early stage and it would take years before we can see clinical application, pharmacogenomics in pancreatic cancer is an important area to watch. There are various preclinical studies investigating polymorphisms and expression levels of genes associated with gemcitabine sensitivity and/or resistance [39]. Given the fact that the cost of sequencing has drastically come down, genotyping patients enrolled in large phase III trials in pancreatic cancer for genotyping should also be a routine practice in order to investigate genotype-phenotype association with significant statistical power in the future [40].
Presence of circulating tumor cells correlates with prognosis and can predict how patient will respond to chemotherapy in breast cancer patients [41]. Research of circulating tumor cells in pancreatic cancer is very limited [42]. Reliable biomarkers such as circulating tumor cells that predict treatment response or outcome earlier than traditional imaging methods will enable oncologists to change treatment regimen before the worsening performance status prohibit us from salvage treatment.
Selected advanced pancreatic cancer patients with good performance status should be considered for 2nd line chemotherapy after 1st line gemcitabine failure [4, 5]. With better patient selection, we can improve clinical outcomes of advanced pancreatic cancer in 2nd line settings. Prospective clinical trials investigating clinical outcomes in association with published prognostic factors such as performance status, C-reactive protein, and peritoneal dissemination may improve patient selection for 2nd line treatment (Figure 1) [43].
Figure 1. Proposed selection guideline for second-line
therapy after gemcitabine failure [43].
Conclusion
Current data set on treatment options in 2nd line setting after gemcitabine failure is scattered and scant. We need to establish the standard of care for this rising group of patients. We can achieve this goal by better understanding of the disease, development of novel agents, and concerted effort to enroll patients in rationally designed clinical trials. Emerging science and technology may further guide us to develop individualized treatment algorithm for advanced pancreatic cancer patients which will spare advanced pancreatic cancer patients from inactive 1st line treatment.
Conflict of interest
The authors have no potential conflicts of interest
References
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997, 15:2403-13. [PMID 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007, 25:1960-6. [PMID 17452677]
- Cunningham D, Chau I, Stocken C, Davies C, Dunn J, Valle J, et al. Phase III randomized comparison of gemcitabine (GEM) versus gemcitabine plus capecitabine (GEM-CAP) in patients with advanced pancreatic cancer. Eur J Cancer Suppl 2005; 3:12. Abstract PS11.
- Herrmann Y, Jaeger D, Stremmel W, Herrmann C. Second-line chemotherapy in advanced pancreatic cancer: A retrospective, single-center analysis. J Clin Oncol 2007 ASCO Annual Meeting Proceedings (Post- Meeting Edition). Vol 25, No 18S (June 20 Suppl):15187.
- Oettle H, Pelzer U, Stieler J, Hilbig A, Roll L, Schwaner I, et al. Oxaliplatin/folinic acid/5- fluorouracil [24h] (OFF) plus best supportive careversus best supportive care alone (BSC) in secondline therapy ofgemcitabine-refractory advanced pancreatic cancer (CONKO 003). J Clin Oncol 2005 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 23, No 16S, Part I of II (June 1 Suppl):4031.
- Mitry E, Ducreux M, Ould-Kaci M, Boige V, Seitz JF, Bugat R, et al. Oxaliplatin combined with 5-FU in second line treatment of advanced pancreatic adenocarcinoma. Results of a phase II trial. Gastroenterol Clin Biol 2006; 30:357-63. [PMID 16633299]
- Gebbia V, Maiello E, Giuliani F, Borsellino N, Caruso M, Di Maggio G, Ferraù F, et al. Second-line chemotherapy in advanced pancreatic carcinoma: a multicenter survey of the Gruppo Oncologico Italia Meridionale on the activity and safety of the FOLFOX4 regimen in clinical practice. Ann Oncol 2007, 18 Suppl 6:vi124-7.
- Tsavaris N, Kosmas C, Skopelitis H, Gouveris P, Kopterides P, Loukeris D, et al. Second-line treatment with oxaliplatin, leucovorin and 5-fluorouracil in gemcitabine-pretreated advanced pancreatic cancer: A phase II study. Invest New Drugs 2005; 23:369-75. [PMID 16012797]
- Cartwright TH, Cohn A, Varkey JA, Chen YM, Szatrowski TP, Cox JV, Schulz JJ. Phase II study of oral capecitabine in patients with advanced or metastatic pancreatic cancer. J Clin Oncol 2002, 20:160-4. [PMID 11773165]
- Boeck SH, Wilkowski R, Bruns CJ, Issels RD, Schulz C, Moosmann N, et al. Oral capecitabine in gemcitabine-pretreated patients with advanced pancreatic cancer: A single-center study. J Clin Oncol 2007 ASCO Annual Meeting Proceedings (Post- Meeting Edition). Vol 25, No. 18S (June 20 Suppl):15085.
- Xiong HQ, Wolff RA, Hess KR, Varadhachary GR, Blais JC, Abbruzzese JL. A phase II trial of oxaliplatin plus capecitabine (xelox) as second line therapy for patients with advanced pancreatic cancer. J Clin Oncol 2006 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 24, No. 18S (June 20 Suppl):4119.
- Blaya M, Lopes GL, Roman E Jr, Ahn E, Macintyre J, Quesada J, et al. Phase II trial of capecitabine and docetaxel as second line therapy for locally advanced and metastatic pancreatic cancer. J Clin Oncol 2007 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 25, No. 18S (June 20 Suppl):15029.
- Gelibter A, Milella M, Malaguti P, De Marco S, Ruggeri E, Carlini P, et al. Pilot study of capecitabine combined with celecoxib (CapCel) as second-line treatment for advanced pancreatic (P) and biliary tree (BT) cancer. J Clin Oncol 2006 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 24, No. 18S (June 20 Suppl):14055.
- Milella M, Gelibter A, Di Cosimo S, Bria E, Ruggeri EM, Carlini P, et al. Pilot study of celecoxib and infusional 5-fluorouracil as second-line treatment for advanced pancreatic carcinoma. Cancer 2004, 101:133-8. [PMID 15221998]
- Kawamoto K, Yamaguchi K, Okabe M, Tsuruta A, Morimoto Y, Niwano M, et al. A case of advanced pancreatic cancer successfully treated by combined chemotherapy of S-1 and gemcitabine as second-line chemotherapy. Gan To Kagaku Ryoho 2007, 34:1131- 4. [PMID 17637556]
- Androulakis N, Syrigos K, Polyzos A, Aravantinos G, Stathopoulos GP, Ziras N, et al. Oxaliplatin for pretreated patients with advanced or metastatic pancreatic cancer: a multicenter phase II study. Cancer Invest 2005, 23:9-12. [PMID 15779862]
- Demols A, Peeters M, Polus M, Marechal R, Gay F, Monsaert E, et al. Gemcitabine and oxaliplatin (GEMOX) in gemcitabine refractory advanced pancreatic adenocarcinoma: a phase II study. Br J Cancer 2006, 94:481-5. [PMID 16434988]
- Cantore M, Rabbi C, Fiorentini G, Oliani C, Zamagni D, Iacono C, et al. Combined irinotecan and oxaliplatin in patients with advanced pre-treated pancreatic cancer. Oncology 2004, 67:93-7. [PMID 15539911]
- Tschoep KE, Milani V, Schmidt G, Schiel X, Abdel-Rahman S, Kuhlencordt MF, et al. Gemcitabine + cisplatin (GEM+CIS) in combination with regional hyperthermia (RHT) in second-line therapy of gemcitabine-refractory metastatic pancreatic cancer. J Clin Oncol 2006 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 24, No. 18S (June 20 Suppl):14073.
- Park Y, Yi S, Kim H, Lee S, Hwang I, Park S, et al. Irinotecan monotherapy as second-line treatment in advanced pancreatic cancer. J Clin Oncol 2007 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 25, No. 18S (June 20 Suppl):15111.
- Mercalli A, Sordi V, Formicola R, Dandrea M, Beghelli S, Scarpa A, et al. A preclinical evaluation of pemetrexed and irinotecan combination as second-line chemotherapy in pancreatic cancer. Br J Cancer 2007, 96:1358-67. [PMID 17426706]
- Ulrich-Pur H, Raderer M, Verena Kornek G, Schüll B, Schmid K, Haider K, et al. Irinotecan plus raltitrexed vs raltitrexed alone in patients with gemcitabine-pretreated advanced pancreatic adenocarcinoma. Br J Cancer 2003, 88:1180-4. [PMID 12698181]
- Taïeb J, Lecomte T, Aparicio T, Asnacios A, Mansourbakht T, Artru P, et al. FOLFIRI.3, a new regimen combining 5-fluorouracil, folinic acid and irinotecan, for advanced pancreatic cancer: results of an Association des Gastro-Enterologues Oncologues (Gastroenterologist Oncologist Association) multicenter phase II study. Ann Oncol 2007, 18:498- 503. [PMID 17158774]
- Burris HA 3rd, Rivkin S, Reynolds R, Harris J, Wax A, Gerstein H, et al. Phase II trial of oral rubitecan in previously treated pancreatic cancer patients. Oncologist 2005, 10:183-90. [PMID 15793221]
- Jacobs AD, Burris HA, Rivkin S, Ritch PS, Eisenberg PD, Mettinger KL, et al. A randomized phase III study of rubitecan (ORA) vs. best choice (BC) in 409 patients with refractory pancreatic cancer report from a North-American multi-center study. J Clin Oncol 2004 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 22, No 14S (July 15 Suppl):4013.
- Ignatiadis M, Polyzos A, Stathopoulos GP, Tselepatiotis E, Christophylakis C, Kalbakis K, et al. A multicenter phase II study of docetaxel in combination with gefitinib in gemcitabine-pretreated patients with advanced/metastatic pancreatic cancer. Oncology 2006, 71:159-63. [PMID 17646699]
- Blaszkowsky LS, Ryan DP, Earle C, Kwak E, Fuchs C, Meyerhardt JA, et al. A phase II study of docetaxel in combination with ZD1839 (gefitinib) in previously treated patients with metastatic pancreatic cancer. J Clin Oncol 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Suppl):15080.
- Oettle H, Arnold D, Esser M, Huhn D, Riess H. Paclitaxel as weekly second-line therapy in patients with advanced pancreatic carcinoma. Anticancer Drugs 2000; 11:635-8. [PMID 11081455]
- Boeck S, Weigang-Köhler K, Fuchs M, Kettner E, Quietzsch D, Trojan J, et al. Second-line chemotherapy with pemetrexed after gemcitabine failure in patients with advanced pancreatic cancer: a multicenter phase II trial. Ann Oncol 2007, 18:745-51. [PMID 17229775]
- Wallace JA, Locker G, Nattam S, Kasza K, Wade- Oliver K, Vokes EE, Kindler HL. Sorafenib (S) plus gemcitabine (G) for advanced pancreatic cancer (PC): A phase II trial of the University of Chicago Phase II Consortium. J Clin Oncol 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Suppl): 4608.
- Kindler HL, Niedzwiecki D, Hollis D, Oraefo E, Schrag D, Hurwitz H, et al. A double-blind, placebocontrolled, randomized phase III trial of gemcitabine (G) plus bevacizumab (B) versus gemcitabine plus placebo (P) in patients (pts) with advanced pancreatic cancer (PC): A preliminary analysis of Cancer and Leukemia Group B (CALGB). J Clin Oncol 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Suppl):4508.
- Epelbaum R, Schnaider J, Gluzman A, Figer A. Erlotinib as a single-agent therapy in patients with advanced pancreatic cancer. ASCO 2007:GCSA; No:202.
- Kulke MH, Blaszkowsky LS, Ryan DP, Clark JW, Meyerhardt JA, Zhu AX, et al. Capecitabine plus erlotinib in gemcitabine-refractory advanced pancreatic cancer. J Clin Oncol 2007, 25:4787-92. [PMID 17947726]
- Burtness BA, Powell M, Berlin J, Liles D, Chapman A, Mitchell E, et al. Phase II trial of irinotecan/docetaxel for advanced pancreatic cancer with randomization between irinotecan/docetaxel and irinotecan/docetaxel plus C225, a monoclonal antibody to the epidermal growth factor receptor (EGF-r) : Eastern Cooperative Oncology. J Clin Oncol 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Suppl):4519.
- Bakkevold KE, Pettersen A, Arnesjø B, Espehaug B. Tamoxifen therapy in unresectable adenocarcinoma of the pancreas and the papilla of Vater. Br J Surg 1990, 77:725-30. [PMID 2200555]
- Keating JJ, Johnson PJ, Cochrane AM, Gazzard BG, Krasner N, Smith PM, et al. A prospective randomised controlled trial of tamoxifen and cyproterone acetate in pancreatic carcinoma. Br J Cancer 1989, 60:789-92. [PMID 2529892]
- Taylor OM, Benson EA, McMahon MJ. Clinical trial of tamoxifen in patients with irresectable pancreatic adenocarcinoma. The Yorkshire Gastrointestinal Tumour Group. Br J Surg 1993, 80:384-6. [PMID 8472160]
- Roy A, Jacobs A, Bukowski R, Cunningham D, Hammet J, et al. Phase 3 trial of SMS 201-995 pa LAR (SMS PA LAR) and continuous infusion 5FU in unresectable stage II, III, and IV pancreatic cancer. Proc Am Soc Clin Oncol 1998; 17:257.
- Ueno H, Kiyosawa K, Kaniwa N. Pharmacogenomics of gemcitabine: can genetic studies lead to tailor-made therapy? Br J Cancer 2007, 97:145- 51. [PMID 17595663]
- Maitland ML, Ratain MJ, Cox NJ. Interpreting P values in pharmacogenetic studies: a call for process and perspective. J Clin Oncol 2007, 25:4513-5. [PMID 17925544]
- Budd GT, Cristofanilli M, Ellis MJ, Stopeck A, Borden E, Miller MC, et al. Circulating tumor cells versus imaging--predicting overall survival in metastatic breast cancer. Clin Cancer Res 2006, 12:6403-9. [PMID 17085652]
- Ko AH, Scott J, Tempero MA, Park JW. Detection and significance of circulating tumor cells (CTC) in patients with metastatic pancreatic cancer (PC) receiving systemic therapy. J Clin Oncol 2007 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Part I. Vol 25, No. 18S (June 20 Suppl):4596.
- Nakachi K, Furuse J, Ishii H, Suzuki E, Yoshino M. Prognostic factors in patients with gemcitabinerefractory pancreatic cancer. Jpn J Clin Oncol 2007, 37:114-20. [PMID 17272317]


