Keywords
Pancreatic Fistula; Pancreatectomy; Pancreatic Ducts
Abbreviations
DP Distal Pancreatectomy; POPF Postoperative
Pancreatic Fistula; ISGPF International Study Group of Pancreatic
Fistula; PDS Polydioxanone Suture;
BACKGROUND
Postoperative pancreatic fistula (POPF) is the most
common cause of morbidity and mortality after distal
pancreatic resection [1]. The incidence of POPF in distal
pancreatectomy (DP) remains high, ranging from 10 to 40%
in recent reports [2, 3]. Different surgical groups have used
various methods in their attempts to prevent pancreatic
fistula after DP, including hand-sewing, compression
suturing with a linear stapler, spraying of fibrin sealment,
and anastomosis of the jejunum and pancreatic duct at
the stump; however, there is no consensus regarding a
standard surgical technique for pancreatic stump closure
after DP [4].
According to a recent meta-analysis, the rate of POPF
after DP in patients who received hand-sewing (28%)
and those who received automated suturing (32%) did
not differ to a statistically significant extent [5]. Recently,
however, stapler closure has come to be commonly
performed. In addition, stapler techniques can be used to close both the main pancreatic duct and the branch duct at
the same time.
A laceration occurs in a straight line and fistula may
develop from both ends of the pancreas even if we use a
straight stapler suture device [6]. We hypothesized that
this is one of the reasons why POPF cannot be completely
prevented. We have therefore begun using a Curved Cutter
Stapler® (Ethicon Endo-surgery, Cincinnati, OH, USA) as a
pancreatic transection device. The aim of this study was
to analyze POPF occurrence after closure of the pancreatic
remnant after DP by using a Curved Cutter Stapler®.
PATIENTS AND METHODS
Thirty-five patients who underwent DP in Shikoku
Central Hospital and Tokushima Red Cross Hospital
between 2008 and 2019 were retrospectively analysed. The
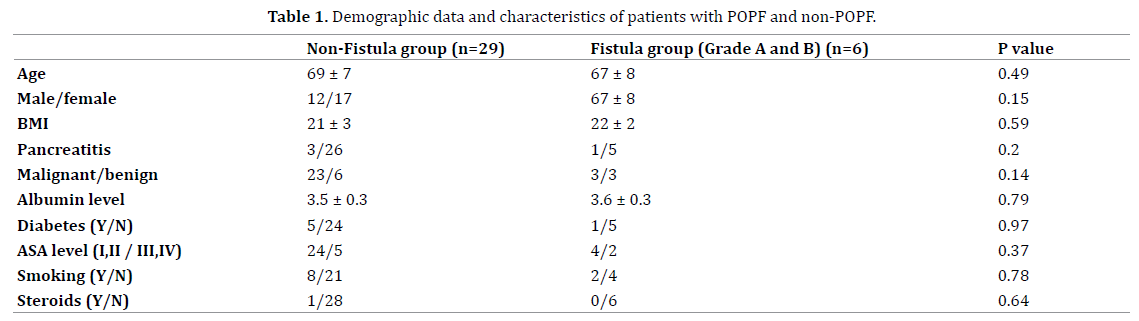
patients’ characteristics are summarized in Table 1. Age,
sex, BMI, history of pancreatitis, malignant disease, serum
albumin level, coexist diseases such as diabetes mellitus,
hypertension, ASA level, history of smoking and steroids
use were evaluated as preoperative characteristics. The
following operative factors were recorded: operation
time, blood loss, thickness of the stump, pancreatic duct
size, texture of the pancreas, and the use of green or
blue cartridges, multi-organ resection and laparoscopic
surgery.
All patients (male, n=17; female, n=18; age, 30-82
years) underwent stapler closure with a Curved Cutter
Stapler. The Curved Cutter Stapler is a single-patient-use
stapler with a curved head that cuts and staples [7]. The device delivers four staggered rows of titanium staples,
with a knife between the second and third row of staples.
The Curved Cutter Stapler is available with green and blue
stapler cartridges that compress tissue to approximately 2
mm and 1.5 mm, respectively. When the handle is applied,
it occludes the tissue on both sides of a 40-mm transection.
Data were collected retrospectively and the clinicpathological
features were reviewed from medical charts.
All patients were divided into two groups according to the
absence or presence of POPF.
Surgical Procedures and Methods
DP was performed as open surgery in 30 patients
and as laparoscopic surgery in 5 patients. All pancreatic
resections were performed in accordance with the
standard procedure, which has been described elsewhere.
Using vinyl tape, the pancreas was lifted, and reusable
intestinal clips were placed horizontal to the resection
line. The position of the pancreatic duct and thickness of
the pancreas were measured by intraoperative US. The
hardness of the pancreas was measured by ultrasonic
elastography. The pancreas was compressed for 10
minutes. After pre-compression, a Curved Cutter Stapler
was inserted and carefully placed over the resection
line (Figure 1). Firing was performed slowly so that the
operator could feel the tightening one line at a time. Both
jaws were closed slowly, and the pancreas was compressed
on the planned transection line for 5 minutes, followed by
gradual stapling for 5 min and cutting. The surgeon can
select whether to use the Curved Cutter Stapler with a
green or blue cartridge.
Figure 1. After pre-compression, a Curved Cutter Stapler was inserted and carefully placed over the resection line.
Although the green cartridge was usually used, if the
thickness of the pancreas was estimated to be <12 mm, the
blue cartridge would be used for transection. If the Curved
Cutter Stapler could not completely cut off the pancreas
the first time, a linear stapler was subsequently used to
cut off the remaining pancreas. The isolation stump of the
pancreas showed a fish mouth form Figure 2. One 5-0 PDS
stitch was added at the expected site of the pancreatic duct.
Figure 2. The isolation stump of the pancreas became the fish mouth form (Arow). One stitch of 5-0 PDS would be added in the site expecte tdhat there is a pancreatic duct.
Post-operative Management
In all cases, a drain was inserted into the pancreatic
stump. The amylase and lipase levels of the serum
and drainage fluid were monitored on postoperative
days 1 and 3. Perioperative antibiotics were routinely administered three times, either intra-operatively or for
one day postoperatively. Somatostatin analog was used in
cases with Grade B POPF and was not used as prophylaxis
against POPF. Oral intake was started if the patient showed
no clinical signs of POPF. Patients with clinical signs of POPF
received somatostatin analog for 7 days after surgery.
POPF was diagnosed according to the definition of the
International Study Group of Pancreatic Fistula (ISGPF)
[8].
Statistical analyses
Data were expressed as the mean ± standard deviation.
Statistical analyses were performed using the Statistical
Package for Social Science for Windows (SPSS Inc; Chicago,
IL, USA). The patient characteristics and intraoperative and
postoperative factors of the POPF and non-POPF groups
were compared by the chi-squared test and Student’s
t-test. Univariate and multivariate logistic analysis were
performed to identify independent predictors of POPF
development. P values of <0.05 were considered to indicate
statistical significance.
This study was approved by the Ethics Committee of
Shikoku Central Hospital.
RESULTS
The mean age of the patients was 68 ± 8 years. Overall,
pathological examinations revealed malignant disease in
26 patients (74%) and benign disease in 9 patients (26%).
As additional surgical procedures, splenectomy was
performed in 33 patients (94%), partial gastrectomy was
performed in 2 patients (6%), liver resection (3%) was
performed in one patient and adrenal gland resection was
performed in one patient (3%).
Thirty-five patients who underwent DP were classified
into the non-fistula or Grade A/B fistula groups. In the
overall study population, Grade A POPF occurred in 4
(11%) patients and Grade B POPF occurred in 2 (6%)
patients. Thus, six (17%) patients who underwent DP using
a Curved Cutter Stapler developed Grade A/B POPF and 29
patients (83%) did not develop POPF. The postoperative
hospital stay of the non-fistula group was significantly
shorter than that of the fistula group (12.5 ± 3.5 days vs.
22.5 ± days, P<0.01). The closing duration for pancreatic
fistula from the onset was 10 ± 7 days in cases with Grade
A POPF and 16 ± 11days in cases with Grade B POPF. There were no significant differences in the preoperative
or clinic-pathological data of the non-fistula and fistula
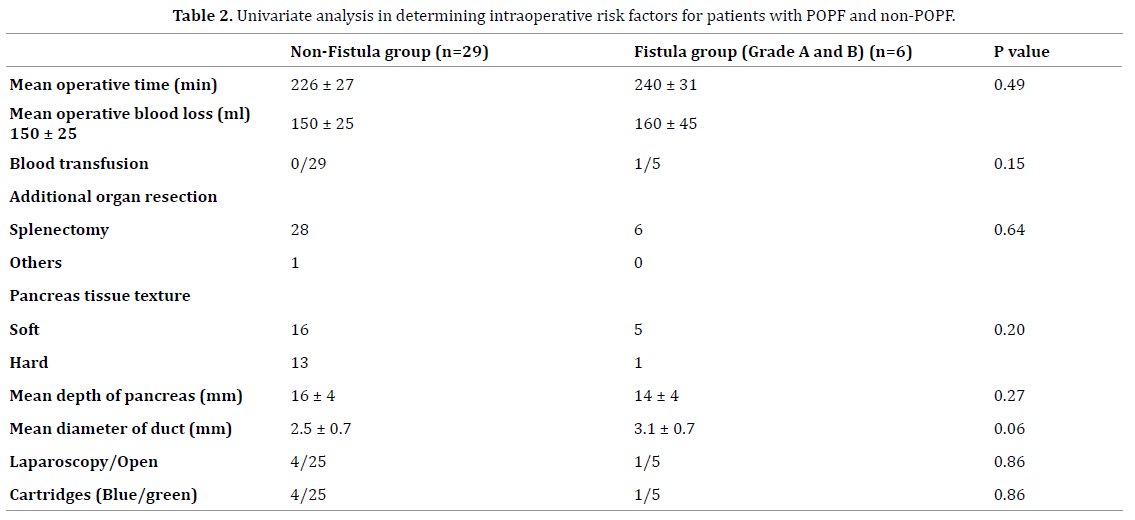
groups (Table 1). Furthermore, no intraoperative factors,
such as operation time, blood loss, thickness of the stump
and pancreatic duct size, texture of the pancreas, the
use of green or blue cartridges, multi-organ resection or
laparoscopic surgery were significantly associated with
the development of fistula the univariate and multivariate
analyses (Table 2). The thickness of the parenchyma of the
transacted portion was 16 ± 4mm in the non-fistula group
and 14 ± 4 mm in the fistula group. The non-fistula group
included 16 cases with a soft tissue texture and 13 with a
hard tissue texture, while the fistula group included 5 cases
with an in soft tissue texture and 1 case with a hard tissue
texture; the difference was not statistically significant. The
POPF rate was 24% (5/21) in the soft pancreas group and
7% (1/14) in the hard pancreas group; this difference was
not statistically significant. Thus, the preoperative and
intraoperative demographic data and relevant risk factors
of the two groups did not differ to a statistically significant
extent.
DISCUSSION
Our study showed that the Grade A POPF (according
to the ISGPF definition) occurred in 4 patients (11%) and
Grade B POPF occurred in 2 patients (6%); no patients
developed Grade C POPF. Thus, relevant POPF was only
detected in 2 (6%) of our patients. Although there are
many methods for the prevention of POPF, no techniques
are fully effective and the incidence of clinical POPF was
>20% in most studies [9, 10]. The incidence of POPF in
the present study was considerably low in comparison to
other studies. To the best of our knowledge, this is the first
report to describe the use of the Curved Cutter Stapler for
pancreatic resection.
Surgeons have used various surgical techniques to
prevent the occurrence of pancreatic fistula after resection
of the pancreatic body and tail. In the hand-sewing
method, techniques such as 1) secure tubal ligation of the
pancreatic duct and 2) suture closure of the pancreatic
resection stump in the shape of a fish mouth are used [11].
On the other hand, pancreatic dissection with a stapler
suture device after tail resection of the pancreatic body has
become easier to perform and is more commonly applied in
many institutions [12, 13]. In 2005 and 2010, respectively,
Knaebel et al and Zhou et al performed meta-analyses on
the application of hand-sewn anastomosis and stapler
suture, and reported that the use of a stapler suture device
reduced the incidence of pancreatic fistula in comparison
to hand-sewn anastomosis. However, in these studies, the
incidence of POPF after DP did not differ to a statistically
significant extent [14, 15]. In 2011, a large multicentre
RCT trial (DISPACT trial) was conducted to compare the
impact of automatic suture and hand-stitched methods on
pancreatic fistula development after DP [5]. The incidence
of pancreatic fistula was 32% (56/177 cases) in the stapler
group and 28% (49/175 cases) in the hand-stitched
group, which did not amount to a statistically significant difference. The study concluded that the use of a surgical
stapler did not contribute to the prevention of pancreatic
fistula due to the crushing and tearing of the pancreas
when stapler closure was adopted. In a retrospective
analysis of 284 cases of DP, Chikhladze et al reported that
the technique of pancreatic stump closure after DP did not
influence the incidence of POPF; however, it was associated
with the pancreatic function and parenchymal texture, and
that it seemed unsafe to use a stapler in cases involving a
pancreas with a thick parenchyma [16, 17].
It was thought that the damage of the pancreatic
membrane might have caused pancreatic fistula when
a stapler was used in DP [18, 19]. Reinforcement of the
pancreatic membrane at the transection line would be
important for the prevention of pancreatic fistula [20, 21].
Thus, some studies using mesh reinforcement have been
reported to reduce pancreatic fistula. However, a metaanalysis
based on 5 retrospective and 5 prospective nonrandomized
studies compared reinforced staplers and
bare staplers, and showed that the incidence of pancreatic
fistula in the bare metal stapling group was 24% (61/249
cases), while that in the reinforced stapler group was 17%
(39/234 cases) [22]. Reinforced stapler resection was not
found to have a significant benefit. Further evaluation in
multi-centre RCTs is necessary to clarify the utility of mesh
reinforcement when it is applied in stapler closure.
The Curved Cutter Stapler has been used to perform
rectal transection in the narrow pelvic cavity [7]. The
reasons for using a Curved Cutter Stapler in our study
were as follows: 1) pancreatic resection in a single session
was possible; 2) the isolated stump has a fish mouth form;
3) there is little bleeding from the isolated stump; 4) the
procedure is simple. In our study, the use of Curved Cutter
Stapler was found to result in a remarkably low rate of
Grade B fistula.
Kleeff et al suggested that the use of stapler may cause
focal pancreatic necrosis in the surrounding stapling site;
however, we hypothesized that a Curved Cutter Stapler
would not cause so much damage to the stump of the
pancreas because of its shape [23]. Thus, a Curved Cutter
Stapler would not impair the outflow of the pancreatic
juice through Wirsung’s duct.
The complication rates after DP are dependent on both
the surgical technique and patient factors [24]. In addition
to aggressive surgery, obesity, significant comorbidities,
male sex and low serum albumin levels are independent
risk factors for fistula formation [25, 26, 27, 28]. Several
studies have suggested that a pancreas with a soft texture
is more prone to leak when a stapler is used [22, 29].
Thus, higher stapler or pancreatoenteric anastomosis
might be recommended for the prevention of POPF when
transecting a thick pancreas [30]. However, in the present
study, the texture of the pancreatic parenchyma was not
associated with the risk of POPF and the frequency of
pancreatic fistula was not also related to the thickness of
the pancreas when the green cartridge was use in cases
involving thick pancreas.
The outcomes of pancreatic resection using a Curved
Cutter Stapler are difficult to interpret due to the relatively
small number of cases; however, we believe that our new
method can contribute to reducing the incidence of POPF.
Multi-centre prospective studies that include large groups
of patients undergoing DP using the Curved Cutter Stapler
are necessary to determine the best methods for the
prevention of POPF.
CONCLUSION
Pancreatic resection using a Curved Cutter Stapler
would contribute to reducing the incidence of pancreatic
fistula and the avoidance of serious complications and would
shorten hospitalization. The use of a Curved Cutter Stapler
could reduce the incidence of severe and potentially fatal
POPF formation. However, it is not possible to completely
prevent the development of Grade A or B fistula.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- Bilimoria MM, Cormier JN, Mun Y, Lee JE, Evans DB, Pisters DWT. Pancreatic leak after pancreatectomy is reduced following main pancreatic duct ligation. Br J Surg 2003; 90:190-196. [PMID: 12555295]
- Katarzyna M, Lukasz W, Tomasz G, Makiewicz M, Nyckowski P, Słodkowski M. A review of methods for preventing pancreatic fistula after distal pancreatectomy. Pol Przegl Chir 2018; 90:38-44. [ PMID: 29773760]
- Serene TEL, Vishalkkumar GS, Padmakumar JS, Terence HCW, Keem LJ, Bei W, et al. Predictive value of post-operative drain amylase levels for post-operative pancreatic fistula. Ann Hepatobiliary Pancreat Surg. 2018; 22:397-404. [PMID: 30588532]
- Loos M, Strobel O, Legominski M, Dietrich M, Hinz U, Brenner T, et al. Postoperative pancreatic fistula: Microbial growth determines outcome. Surgery 2018; 164:1185-1190. [PMID: 30217397]
- Diener MK, Seiler CM, Rossion I, Kleeff J, Glanemann M, Butturini G, et al. Efficacy of stapler versus hand-sewn closure after distal pancreatectomy (DISPACT): a randomised, controlled multicentre trial. Lancet. 2011; 377:1514-1522. [PMID: 21529927]
- Adem Y, Erdal B, Muhammet C, et al. Pancreatic stump closure using only stapler is associated with high postoperative fistula rate after minimal invasive surgery. Turk J Gastroenterol. 2018; 29:191-197. [PMID: 29749326]
- Ishii Y, Hasegawa H, Nishibori H, Endo T, Kitajima M. The application of new stapling device for open surgery (Contour Curved Cutter Stapler) in the laparoscopic resection of rectal cancer. Surg Endosc 2006; 20:1329-1331. [PMID: 16763925]
- Bassi C, Butturini G, Molinari E, Mascetta G, Salvia R, Falconi M, et al. Pancreatic fistula rate after pancreatic resection. The importance of definitions. Dig Surg 2004; 21:54-59. [PMID: 14707394]
- Makino I, Kitagawa H, Nakagawara H, Tajima H, Ninomiya I, Fushida S, et al. Management of remnant pancreatic stump to prevent the development of postoperative pancreatic fistulas after distal pancreatectomy: current evidence and our strategy. Surg Today 2013; 43:595-602. [PMID: 23093346]
- Kawai M, Hirono S, Okada K, Sho M, Nakajima Y, Eguchi H, et al. Randomized Controlled Trial of pancreaticojejunostomy versus stapler closure of the pancreatic stump during distal pancreatectomy to reduce pancreatic fistula. Ann Surg 2016; 264:180-187. [PMID: 26473652]
- Olah A, Issekutz A, Belagyi T, Hajdú N, Romics L, et al. Randomized clinical trial of techniques for closure of the pancreatic remnant following distal pancreatectomy. Br J Surg. 2009; 96:602-607. [PMID: 19434697]
- Ban D, Shimada K, Konishi M, Saiura A, Hashimoto M, Uesaka K. Stapler and nonstapler closure of the pancreatic remnant after distal pancreatectomy: multicenter retrospective analysis of 388 patients. World J Surg 2012; 36:1866-1873. [PMID: 22526040]
- Bassi C, Butturini G, Falconi M, Salvia R, Sartori N, Caldiron E, et al. Prospective randomised pilot study of management of the pancreatic stump following distal resection. HPB (Oxford) 1999; 1:203-207.
- Knaebel HP, Diener MK, Wente MN, Büchler MW, Seiler CM. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg 2005; 92:539-546. [PMID: 15852419]
- Zhou W, Lv R, Wang X, Mou Y, Cai X, Herr I. Stapler vs suture closure of pancreatic remnant after distal pancreatectomy: a meta-analysis. Am J Surg 2010; 200:529-536. [PMID: 20538249]
- Chikhladze S, Makowiec F, Kusters S, Riediger H, Sick O, Fichtner-Feigl S, et al. The Rate of postoperative pancreatic fistula after distal pancreatectomy Is independent of the pancreatic stump closure technique – A retrospective analysis of 284 cases. Asian J Surg 2020; 43:227-233. [PMID: 30982560]
- Nathan H, Cameron JL, Goodwin CR, Seth AK, Edil BH, Wolfgang CL, et al. Risk factors for pancreatic leak after distal pancreatectomy. Ann Surg 2009; 250:277-281. [PMID: 19638926]
- Arai T, Kobayashi A, Yokoyama T, Ohya A, Fujinaga Y, Shimizu A, et al. Signal intensity of the pancreas on magnetic resonance imaging: prediction of postoperative pancreatic fistula after a distal pancreatectomy using a triple-row stapler. Pancreatology 2015; 15:380-386. [PMID: 26118649]
- Okano K, Oshima M, Kakinoki K, Yamamoto N, Akamoto S, Yachida S, et al. Pancreatic thickness as a predictive factor for postoperative pancreatic fistula after distal pancreatectomy using an endopath stapler. Surg Today 2013; 43:141-147. [PMID: 22782593]
- Hayashibe A, Ogino N. Clinical study for pancreatic fistula after distal pancreatectomy with mesh reinforcement. Asian Journal of Surgery. 2018; 41:236-240. [PMID: 27964997]
- Nicholas AH, Matthew RP, Fabian MJ, Gao F, Strasberg SM, Linehan DC, et al. Mesh reinforcement of pancreatic transection decreases incidence of pancreatic occlusion failure for left pancreatectomy: A single-Blinded, Randomized Controlled Trial. Ann Surg 2012; 255:1037-1042. [PMID: 22534422]
- Kollar D, Huszar T, Poharnok Z, Cselovszky E, Oláh A. A review of techniques for closure of the pancreatic remnant following distal pancreatectomy. Dig Surg 2016; 33:320-328. [PMID: 27215609]
- Kleeff J, Diener MK, Z’graggen K, Hinz U, Wagner M, Bachmann J, et al. Distal pancreatectomy: risk factors for surgical failure in 302 consecutive cases. Ann Surg 2007; 245:573-582. [PMID: 17414606]
- Hashimoto Y, Traverso LW. After distal pancreatectomy pancreatic leakage from the stump of the pancreas may be due to drain failure or pancreatic ductal back pressure. J Gastrointest Surg 2012; 16:993-1003. [PMID: 22392088]
- Ecker BL, Mcmillan MT, Allegrini V, Bassi C, Joal D, Beane JD, et al. Risk factors and mitigation strategies for pancreatic fistula after distal Ppancreatectomy: Analysis of 2026 resections from the international, multi-institutional distal pancreatectomy study group. Ann Surg 2019; 269:143-149. [PMID: 28857813]
- Kawaida H, Kono H, Amemiya H, Hosomura N, Saito R, Takahashi K, et al. Use of a reinforced triple-row stapler following distal pancreatectomy reduces the Incidence of postoperative pancreatic fistula in patients with a high BMI. Anticancer Res 2019; 39:1013-1018. [PMID: 30711989]
- Futagawa Y, Takano Y, Furukawa K, Kanehira M, Onda S, Sakamoto T, et al. Comparison of outcomes with hand-sewn versus stapler closure of pancreatic stump in distal pancreatectomy. Anticancer Res 2017; 37:2515-2521. [PMID: 28476821]
- Miyasaka Y, Mori Y, Nakata K, Ohtsuka T, Nakamura M. Attempts to prevent postoperative pancreatic fistula after distal pancreatectomy. Surg Today 2017; 47:416-424. [PMID: 27324393]
- Kawai K, Tani M, Okada K, Hirono S, Miyazawa M, Shimizu A, et al. Stump closure of a thick pancreas using stapler closure increases pancreatic fistula after distal pancreatectomy. Am J Surg 2013; 206:352-359. [PMID: 23806829]
- Michalski CW, Tramelli P, Buchler MW, Hackert T. Closure of pancreas stump after distal and segmental resection: Suture, stapler, coverage or anastomosis? Chirurg 2017; 88:25-29. [PMID: 27778058]



