Keywords
Endoscopic Ultrasound-Guided Fine Needle Aspiration;
Neuroendocrine Tumors; Surgical Procedures, Operative
Abbreviations
DFS disease-free survival; DP distal pancreatectomy;
DPPHR duodenum-preserving pancreatic head resection; EUSFNA
Endoscopic ultrasound-guided fine-needle aspiration; IPMN
intraductal papillary mucinous neoplasm; ISGPF International Study
Group on Pancreatic Fistula; Lap laparoscopic; LN lymph node; lyv-ne microinvasion lymphovascular or perineural microinvasion;
MP middle pancreatectomy; NF-pNET non-functional pancreatic
neuroendocrine tumor; PD pancreaticoduodenectomy; PDAC
pancreatic ductal adenocarcinoma; POPF postoperative pancreatic
fistula; SPN solid pseudo-papillary neoplasm
INTRODUCTION
A pancreatic neuroendocrine tumor (pNET) is a
rare disease which constitutes 1%-2% of all pancreatic
cancers [1]. This tumor is clinically divided into two major
categories; functional tumors with excess production of hormones and non-functional (NF) tumors
without excess hormone production. The tumor biology
is still largely unknown. For functional pNET, treatment
is planned based on not only oncological, but also
endocrinological aspects to relieve symptoms caused
by adverse effects of the excess hormones. It has been
reported that the incidence of pNET is increasing in
Japan and the United States [2, 3]. In recent years, the
incidence of non-symptomatic pNET with smaller size
has increased, implying widespread and frequent use of
high-resolution medical imaging in recent clinical practice
[4, 5]. This change in demography emphasizes some
controversies in the management of NF-pNET, especially
when the tumor is small and non-symptomatic. Generally,
pNET has a more indolent tumor biology than that of
pancreatic ductal adenocarcinoma (PDAC), and there
is no established way to precisely evaluate malignant
potential. Intraductal papillary mucinous neoplasm
(IPMN), the most common cystic tumor of the pancreas,
also has more indolent features than PDAC. For IPMN, precise oncological evaluation, especially with the goal
of evaluating malignant potential, has been pursued by
means of cumulative findings and the establishment of
clinical guidelines [6, 7, 8]. In this context, it seemed useful
to review and analyze cases for the purpose of shedding
light on the tumor biology of NF-pNET. The present study
focused on curatively resected NF-pNET with the goal of
clearly revealing oncological features and tumor behavior
after curative resection. First, we evaluated the impact of
our surgical procedures, especially concentrating on lymph
node (LN) dissection. Then, we investigated the influence
of tumor grade determined by the Ki-67 proliferative index
and LN metastasis as important malignant features of NFpNET
to assess oncological outcome.
METHODS
Data Collection
Fifty-two patients underwent surgery for
neuroendocrine tumors in the hepato-biliary-pancreatic
region including the duodenum consecutively from
January 2003 to December 2016 at Sapporo Medical
University Hospital. These patients were retrospectively
analyzed, and 31 patients with NF-pNET were selected
for analysis according to the following criteria: A)
exhibited no symptoms or signs suggestive of excess
hormone production, B) showed no distant metastasis
in preoperative diagnostic imaging or intraoperative
observation and underwent curative pancreatic resection,
C) had pathologically proven primary pNET in the
pancreas, D) received observation for more than six
months after operation. For these 31 patients, information
on clinical presentation, demographics, surgical procedure,
postoperative course, pathological diagnosis, and followup
including recurrence and survival were collected
from the medical records at Sapporo Medical University
Hospital. The study was approved by the Institutional
Review Board and conducted in adherence with the
Declaration of Helsinki.
Surgical Procedures
Basically, pancreaticoduodenectomy (PD), mainly
pylorus-preserving PD, was conducted for pancreatic
head lesions. Distal pancreatectomy with splenectomy
(DP) including total resection of the pancreatic tail
with or without total resection of the pancreatic body,
was conducted for lesions of the pancreatic body and
tail depending on locations. In PD and DP, regional
peripancreatic lymph nodes were dissected. Further lymph
node dissection around the celiac trunk, common hepatic
artery, hepatoduodenal ligament, or superior mesenteric
artery was conducted depending on tumor status and the
surgeon’s discretion. Six patients underwent laparoscopic
distal pancreatectomy (Lap-DP). We applied the
techniques of laparoscopic gastric cancer surgery to Lap-DP for additional lymph node dissection around the celiac
trunk, common hepatic artery or proximal splenic artery,
in anticipation of obtaining more information regarding LN
status. Pancreatic parenchyma-preserving resection such as middle pancreatectomy (MP) or duodenum-preserving
pancreatic head resection (DPPHR) was conducted
depending on tumor status and the surgeon’s judgment.
Even in MP and DPPHR, at least one lymph node was
harvested. Postoperative pancreatic fistula (POPF) was
graded according to the classification of the International
Study Group on Pancreatic Fistula (ISGPF) [9].
Pathological Analysis
In addition to routine diagnosis by hematoxylin
and eosin (H & E) staining, immunohistochemistry for
chromogranin A (CgA), synaptophysin, or CD56 was used
to diagnose NET. All cases were reviewed and classified
according to the World Health Organization 2010 (WHO
2010) classification with determination of the Ki-67
proliferative index. The tumor factor, LN status, and quality
of resection were evaluated according to the classification
of the Union for International Cancer Control (UICC) [10].
Statistical Analysis
Continuous variables are described as median and
range. Qualitative variables are described as nominal scales
and percentages. Comparison of continuous variables and
qualitative data between two groups were conducted by the
Mann-Whitney U test and Fisher’s exact test, respectively.
Disease-free survival (DFS) was defined as the time from
operation to disease recurrence. A patient was censored at
the last observation time if no event had occurred. Survival
curves were plotted by the Kaplan-Meier method and
compared by the log-rank and Wilcoxon tests. Binomial
logistic regression analysis was performed to determine
associations between the variables that were significant in
univariate analysis and LN metastasis. Receiver operating
characteristic (ROC) analysis was conducted to analyze the
cut-off value of tumor size, which is the most predictive of
LN metastasis. Statistical analysis was performed using
GraphPad Prism 7 software (GraphPad Software, Inc.; La
Jolla, CA, USA) and IBM SPSS Statistics v. 20 (IBM Japan;
Tokyo, Japan).
RESULTS
Demography, Surgical Procedures, Pathological
Findings, and Outcomes of the 31 Study Patients
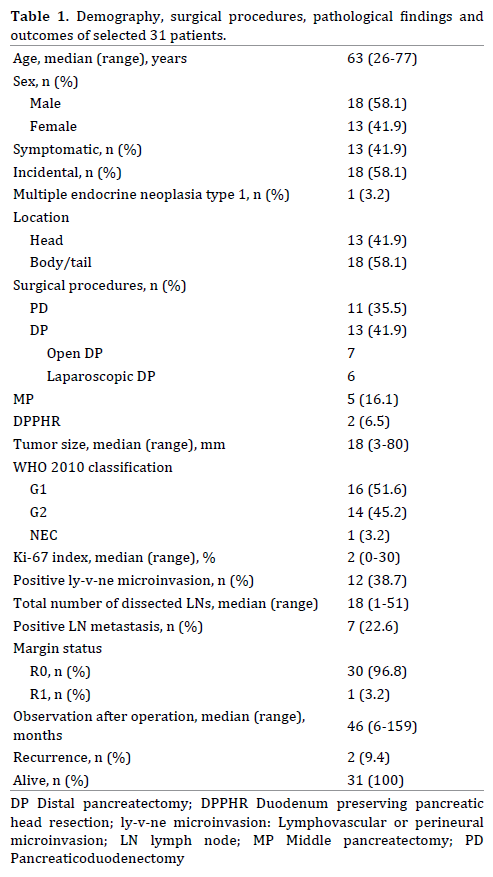
Thirty-one patients who underwent curative resection
for NF-pNET without distant metastasis at the time of
resection were selected for analysis over the 14-year
study period (Table 1). In this retrospective cohort, 13
patients (41.9%) manifested symptoms before surgery.
The most frequent symptom was weight loss (n=4), and
the second most frequent symptom was back pain (n=3) or
abdominal pain (n=3). In addition to PD and DP, pancreatic
parenchyma-preserving resection, such as MP or DPPHR,
was performed for 7 patients (22.6%). Laparoscopic
DP was conducted in 6 patients (19.4%). All of the other
operations were conventional open laparotomy. According
to the WHO 2010 classification, 51.6%, 45.2% and 3.2%
of patients were diagnosed as having G1, G2 and NEC
tumors, respectively. Lymphovascular or perineural (ly-v-ne) microinvasion was observed in 12 patients (38.7%).
LN metastasis was observed in 7 patients (22.6%). The
R0 resection rate was 96.8%. Only one patient who was
diagnosed with a solid pseudo-papillary neoplasm (SPN)
preoperatively underwent R1 resection by Lap-DP due to
peripancreatic invasion of a G2 NF-pNET. Radical open
resection of the pancreatic bed, remnant pancreatic body,
and left prerenal fascia with extended LN dissection was
conducted after the initial operation.
Recurrence occurred in 2 patients (3.2%), which
was detected only in the liver at 29 and 38 months after
surgery, respectively, and there were no local recurrences
recorded in either of the patients. All study patients were
alive within the median observation period of 46 months.
The five-year DFS rate was 89.4% (Figure 1a).
Figure 1.Disease-free survival curves by the Kaplan-Meier method. a: for all patients (n=31), b: the blue line is for the patients without lymph node metastasis (n=24) and the red line is for those with lymph node metastasis (n=7). The difference was statistically significant (P < 0.05).
Surgical Procedures and LN Dissection
The impact of type of operation on LN dissection was
evaluated (Table 2). In all types of surgery, at least one LN
was always harvested and then pathologically evaluated.
The total number of dissected LNs was significantly higher in patients who underwent PD (P=0.004) and DP (P<0.001)
than in the patients who received pancreatic parenchymapreserving
surgery; however, there was no significant
difference between PD and DP (P=0.638).

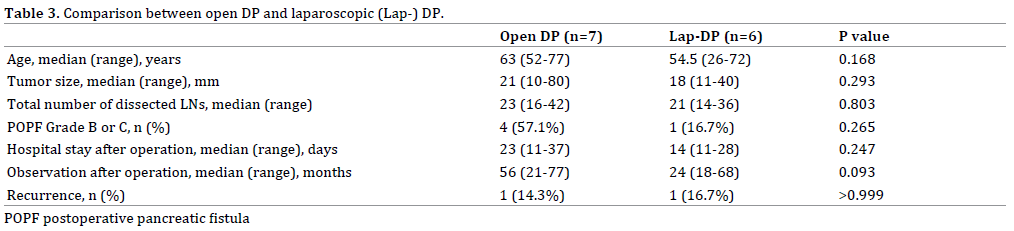
Further evaluation was performed between open DP
and Lap-DP (Table 3). We conducted additional lymph
node dissection around the celiac trunk, common hepatic
artery, and proximal splenic artery during Lap-DP.
Pathological diagnosis revealed that six LNs on average
were evaluated in addition to peripancreatic LNs after
Lap-DP. There were no significant differences between
patient age, tumor size, total number of dissected LNs,
outcome including the rate of POPF, length of hospital stay
and observation after operation, and recurrence rate. We
conjectured that Lap-DP with additional LN dissection
around the celiac trunk, common hepatic artery, and
proximal splenic artery were as feasible as open DP for the
quality of LN dissection and gross outcome.
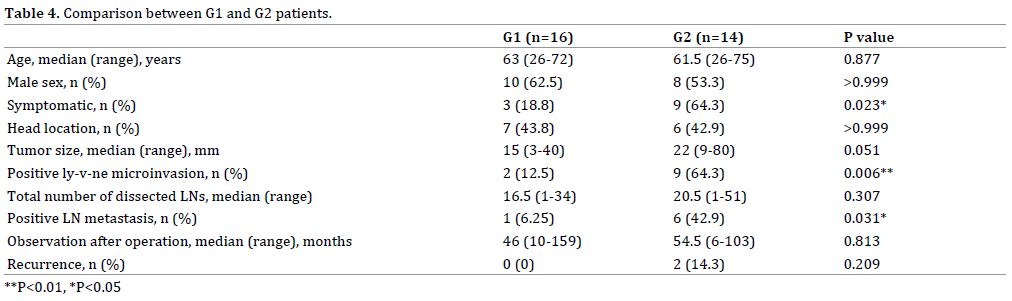
Tumor Grade and Features
Features of G2 patients (n=14) were compared
with those of G1 patients (n=16) (Table 4). Univariate
analysis showed no significant differences in tumor size,
total number of dissected LNs, length of observation, or
recurrence rate between G2 and G1 patients. The 5-year
DFS rates of G2 and G1 patients were 79.5% and 100%,
respectively, with no significant difference (P=0.164
by the log-rank test and P=0.1687 by the Wilcoxon
test). However, the G2 patients were significantly more
symptomatic than the G1 patients, with high prevalence of
ly-v-ne microinvasion and LN metastasis.
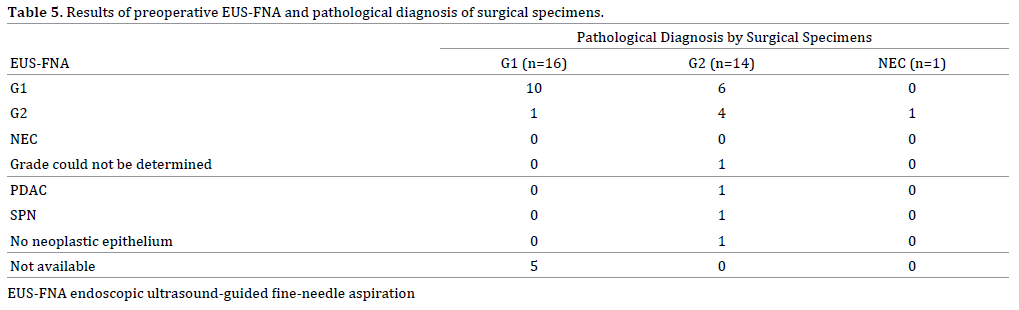
Pathological information about preoperative
endoscopic ultrasound-guided fine-needle aspiration
(EUS-FNA) was available in 26 of the patients (Table 5).
The EUS-FNA specimens were diagnosed as NET in 23
patients (88.5%). In the other 3 patients, one patient was
diagnosed with PDAC, one patient was diagnosed with
SPN, and the final patient was diagnosed as not having
neoplastic epithelium. The WHO 2010 grade according to
Ki-67 staining could be determined in 22 of the patients.
The grade of surgical specimens matched the EUS-FNA
findings in 14 patients, for a concordance rate of 63.6%
(14/22). The positive predictive value (PPV) of the EUSFNA
results was 62.5% (10/16) for G1 and 66.7% (4/6)
for G2. However, in the 14 patients with G2 who were
diagnosed via surgical specimens, only 4 of those patients
were diagnosed by preoperative EUS-FNA, indicating
that the sensitivity in the G2 patients was 28.6% (4/14).
On the other hand, the sensitivity in the G1 patients who
underwent EUS-FNA was 90.9% (10/11).
LN Metastasis and Features
The G2 tumor grade was significantly associated with
LN metastasis; however, preoperative diagnosis by EUSFNA
showed limited sensitivity in the G2 patients. To
reveal the detailed features of LN metastasis in NF-pNET,
the patients with LN metastasis (n=7) were compared with
the patients without LN metastasis (n=24), as summarized in Table 6. Among the patients with LN metastasis, the
tumor size and the total number of dissected LNs were
significantly larger, and there was a higher prevalence of
ly-v-ne microinvasion and G2 tumors than in the patients
without metastasis. Finally, LN metastasis was significantly
associated with recurrence. The 5-year DFS rates of the
patients with and without LN-metastasis were 62.5% and
100%, respectively, with statistically significant difference
(P=0.019 by the log-rank test and P=0.020 by the Wilcoxon
test) (Figure 1b). Multivariate analysis was performed
to determine predictive variables for LN metastasis or
recurrence from the significant factors found through
univariate analysis. No independent predictive variables were detected by binomial logistic regression analysis
(data not shown). From ROC analysis of the tumor size,
a cut-off size of 20. 5 mm was determined to predict
LN metastasis, which showed an area under the curve
(AUC) value of 0.893 (P<0.001), sensitivity of 0.857, and
specificity of 0.792 (Figure 2).
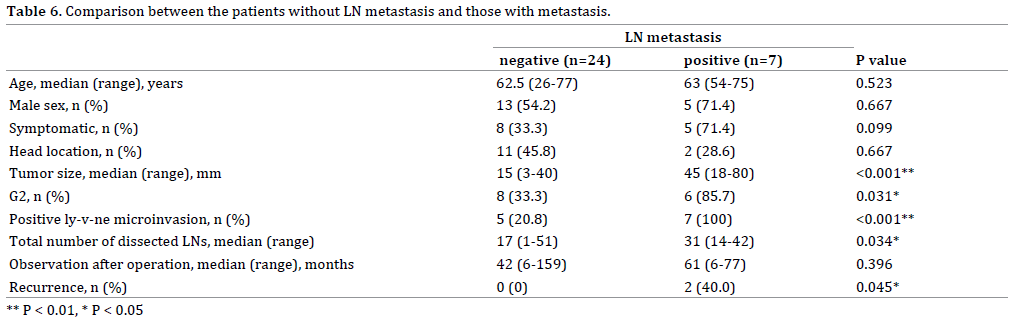
Figure 2. Receiver operating characteristic curve of tumor size to predict
lymph node metastasis. The black arrow indicates the most predictive
point of sensitivity 0.857 and specificity 0.792.
DISCUSSION
NF-pNETs without excess production of hormones
are less symptomatic than functional pNETs. At present,
the number of non-symptomatic NF-pNETs with small
tumor size that are incidentally discovered is increasing.
Vagefi et al. reported that in the early 2000s, the majority of surgically resected pNETs were non-functional (65.9%)
and were incidentally discovered (60.4%) [4]. In another
study, the tumor size of incidentally discovered and
surgically resected NF-pNETs ranged 4 mm to 170 mm,
with a median size of 30 mm [11]. In our cohort, 58.1%
of the NF-pNETs were discovered incidentally without
symptoms during medical exams for the other diseases
and regular medical checkups. Tumor size ranged from 3
mm and 80 mm, with a median size of 18 mm, which was
smaller than in previous reports [4, 11]. These features might depend on the data collection period, as the data
on our patients were collected from 2003 to 2016, for the
latest 14 years.
Pancreatic parenchyma-preserving resections—MPs
and DPPHRs—were performed in 22.6% of the patients
in our cohort. The total number of dissected LNs was
significantly lower in parenchyma-preserving resections
than in PDs and DPs, as previously reported [12], although
at least one LN was always harvested to evaluate LN status
as much as possible. There were no local recurrences and
disease-specific or non-specific deaths recorded among our
study patients; the median length of observation was 46
months after curative resection. We compared the patients
who underwent Lap-DP with the patients who received
open DP, noting the comparable quality of LN dissection
and oncological outcome. The performance of Lap-DP has
become more widespread as a minimally invasive surgery
(MIS) for pNET. A meta- analysis of the MIS approach
specific for pNETs suggested better short-term outcomes
[13]. Oncological indications for parenchyma-preserving
resection or LN dissection are more complicated and
represent a controversial topic for treating NF-pNET.
Fernández-Cruz et al. reported acceptable oncological
outcomes of laparoscopic enucleation for NF-pNET with
regional LN dissection, paying close attention to the status
of LNs [14]. Recurrence of G1 NF-pNET at a local LN was
reported after spleen-preserving DP without LN dissection
[15]. Lombardi et al. [16] pointed out that 39% of NFpNETs
with a size of ≤ 2 cm showed malignant potential,
including distant metastasis, local LN metastasis, and local
infiltration. Furthermore, among 40 resected NF-pNETs, with size ranging from 1 cm to 2 cm, two disease-specific
deaths were reported [17]. In contrast to these data on
individuals, Conrad et al. [18] analyzed surgically resected
pNETs without distant metastasis from a large database and
found that LN metastasis was a negative predictor for survival
only when tumors were confined to the pancreas; extended
LN dissection did not show significant survival advantage in
any stage group. Further accumulation of surgical cases of NFpNET
and prospective randomized control trials are urgently
needed to determine detailed indications for parenchymapreserving
resection and LN dissection.
In our cohort, G2 patients were significantly more
symptomatic, with a higher prevalence of ly-v-ne
microinvasion and LN metastasis. However, there were
no significant associations between G2 and tumor size,
recurrence rate, or DFS. We conjectured that our cohort
without distant metastasis was diagnosed and resected
at the very early stage of tumor development before the
differences between G1 and G2 tumor were manifested
clearly. The other possibility was that the accuracy
of preoperative tumor grade evaluation might have
influenced the subsequent treatment plan (i.e., surgical
procedure or extent of LN dissection) and consequently
the oncological outcome. The concordance rate of our
preoperative EUS-FNA was 63.6%, which was relatively
lower than the rate of 74% to 89% in previous studies [19, 20, 21]. Furthermore, only 28.6% of the G2 patients were
diagnosed by preoperative EUS-FNA, highlighting need
for caution in depending on EUS-FNA to make treatment
decisions. LN metastasis was found to be significantly
associated with DFS, recurrence rate, larger tumor size,
and higher rate of G2 and ly-v-ne microinvasion. Venous
or perineural microinvasion has also been reported as
an independent predictor of recurrence [22, 23]. In our
cohort with a lower number of total and recurrent cases
than in the previous reports, ly-v-ne microinvasion was
not associated with recurrence (P=0.141). ROC analysis
revealed that the prognostic cut-off value of tumor size
for LN metastasis was 20.5 mm, which was within the
range of previous reports, although the cut-off value
widely varied among previous studies, ranging from 15
mm to 40 mm including pathological and radiological
size [12, 24, 25, 26, 27, 28, 29]. LN metastasis might be
difficult to predict precisely based on routine clinical
information such as symptoms, tumor size, and tumor
grade. Recently, Jiao et al. detected frequently mutated
genes in pNET; important gene alterations in pNET were
almost completely different from common gene mutations
in PDAC and newly discovered gene mutations in IPMN [30, 31], suggesting unique tumorigenic mechanisms of pNET
that are distinguished from PDAC and IPMN. The genetic and
molecular pathogenesis of pNETs is important fundamental
information for future improvements in prognosis and
selection of treatment [32]. Further studies are warranted.
A limitation of the present study was that it was a
retrospective analysis of a small number of patients in
a single institute. In addition, preoperative diagnosis
of tumor grade by EUS-FNA might have influenced the selection of the surgical procedures and consequently the
outcomes. Another limitation was that the small number
of total and recurrent cases hindered the detection of
independent predictive factors.
CONCLUSION
The present study retrospectively analyzed the
features of curatively resected NF-pNET without distant
metastasis. In accordance with the current trend, the
majority of cases were incidentally detected. The 5-year
DFS rate was 89.4% with no deaths. At least one LN was
evaluated independently of surgical procedures. Lap-DP with additional LN dissection around the celiac trunk
demonstrated feasible outcomes comparable to the
outcomes of open DP. Tumor grade of G2 was significantly
associated with LN metastasis; however, preoperative
diagnosis by EUS-FNA showed a limited sensitivity in
G2 patients. LN metastasis was significantly associated
with recurrence, and the cut-off value of tumor size for
predicting LN metastasis was 20.5 mm. Further studies
are needed for better prediction of LN metastasis and
selection of treatment.
Conflict of Interest
None of the authors have any conflict-of-interest to
disclose related to this article.
References
- Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic
neuroendocrine tumors (PNETs): incidence, prognosis and recent
trend toward improved survival. Ann Oncol 2008; 19:1727-33.
[PMID: 18515795]
- Ito T, Lee L, Hijioka M, Kawabe K, Kato M, Nakamura K, et al. The
up-to-date review of epidemiological pancreatic neuroendocrine tumors
in Japan. J Hepatobiliary Pancreat Sci 2015; 22:574-7. [PMID: 25689058]
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One
hundred years after "carcinoid": epidemiology of and prognostic factors
for neuroendocrine tumors in 35,825 cases in the United States. J Clin
Oncol 2008; 26:3063-72. [PMID: 18565984]
- Vagefi PA, Razo O, Deshpande V, McGrath DJ, Lauwers GY, Thayer
SP, et al. Evolving patterns in the detection and outcomes of pancreatic
neuroendocrine neoplasms: the Massachusetts General Hospital
experience from 1977 to 2005. Arch Surg 2007; 142:347-54. [PMID:
17438169]
- Song KB, Kim SC, Kim JH, Hong SM, Park KM, Hwang DW, et al.
Prognostic factors in 151 patients with surgically resected nonfunctioning
pancreatic neuroendocrine tumours. ANZ J Surg 2016;
86:563-7. [PMID: 25040037]
- Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang
JY, et al. International consensus guidelines 2012 for the management of
IPMN and MCN of the pancreas. Pancreatology 2012; 12:183-97. [PMID:
22687371]
- Del Chiaro M, Verbeke C, Salvia R, Klöppel G, Werner J, McKay C,
et al. European experts consensus statement on cystic tumours of the
pancreas. Dig Liver Dis 2013; 45:703-11. [PMID: 23415799]
- Vege SS, Ziring B, Jain R, Moayyedi P. American gastroenterological
association institute guideline on the diagnosis and management of
asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;
148:819-22. [PMID: 25805375]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al.
Postoperative pancreatic fistula: an international study group (ISGPF)
definition. Surgery 2005; 138:8-13. [PMID: 16003309]
- Sobin LH, Gospodarowicz MK, Wittekind C, eds. TNM Classification of
Malignant Tumours, 7th Edition. New York: Wiley-Blackwell, 2011.
- Haynes AB, Deshpande V, Ingkakul T, Vagefi PA, Szymonifka J,
Thayer SP, et al. Implications of incidentally discovered, nonfunctioning
pancreatic endocrine tumors: short-term and long-term patient
outcomes. Arch Surg 2011; 146:534-8. [PMID: 21576607]
- Partelli S, Gaujoux S, Boninsegna L, Cherif R, Crippa S, Couvelard
A, et al. Pattern and clinical predictors of lymph node involvement in
nonfunctioning pancreatic neuroendocrine tumors (NF-PanNETs). JAMA
Surg 2013; 148:932-9. [PMID: 23986355]
- Drymousis P, Raptis DA, Spalding D, Fernández-Cruz L, Menon D,
Breitenstein S, et al. Laparoscopic versus open pancreas resection for
pancreatic neuroendocrine tumours: a systematic review and metaanalysis.
HPB (Oxford) 2014; 16:397-406. [PMID: 24245906]
- Fernández-Cruz L, Molina V, Vallejos R, Jiménez Chavarria E, López- Boado MA, Ferrer J. Outcome after laparoscopic enucleation for nonfunctional
neuroendocrine pancreatic tumours. HPB (Oxford) 2012;
14:171-6. [PMID: 22321035]
- Yoo YJ, Yang SJ, Hwang HK, Kang CM, Kim H, Lee WJ. Overestimated
oncologic significance of lymph node metastasis in G1 nonfunctioning
neuroendocrine tumor in the left side of the pancreas. Medicine
(Baltimore) 2015; 94:e1404. [PMID: 26356692]
- Lombardi M, De Lio N, Funel N, Sardella C, Russo D, Urbani C, et al.
Prognostic factors for pancreatic neuroendocrine neoplasms (pNET) and
the risk of small non-functioning pNET. J Endocrinol Invest 2015; 38:605-13. [PMID: 25501604]
- Cherenfant J, Stocker SJ, Gage MK, Du H, Thurow TA, Odeleye M,
et al. Predicting aggressive behavior in nonfunctioning pancreatic
neuroendocrine tumors. Surgery 2013; 154:785-91. [PMID: 24074416]
- Conrad C, Kutlu OC, Dasari A, Chan JA, Vauthey JN, Adams DB, et al.
Prognostic value of lymph node status and extent of lymphadenectomy
in pancreatic neuroendocrine tumors confined to and extending beyond
the pancreas. J Gastrointest Surg 2016; 20:1966-74. [PMID: 27714644]
- Piani C, Franchi GM, Cappelletti C, Scavini M, Albarello L, Zerbi A, et
al. Cytological Ki-67 in pancreatic endocrine tumours: an opportunity
for pre-operative grading. Endocr Relat Cancer 2008; 15:175-81. [PMID:
18310285]
- Larghi A, Capurso G, Carnuccio A, Ricci R, Alfieri S, Galasso D, et al.
Ki-67 grading of nonfunctioning pancreatic neuroendocrine tumors on
histologic samples obtained by EUS-guided fine-needle tissue acquisition:
a prospective study. Gastrointest Endosc 2012; 76:570-7. [PMID:
22898415]
- Hasegawa T, Yamao K, Hijioka S, Bhatia V, Mizuno N, Hara K, et al.
Evaluation of Ki-67 index in EUS-FNA specimens for the assessment of
malignancy risk in pancreatic neuroendocrine tumors. Endoscopy 2014;
46:32-8. [PMID: 24218309]
- Nanno Y, Toyama H, Otani K, Asari S, Goto T, Terai S, et al. Microscopic
venous invasion in patients with pancreatic neuroendocrine tumor as a
potential predictor of postoperative recurrence. Pancreatology 2016;
16:882-7. [PMID: 27350059]
- Tsutsumi K, Ohtsuka T, Fujino M, Nakashima H, Aishima S, Ueda J,
et al. Analysis of risk factors for recurrence after curative resection of
well-differentiated pancreatic neuroendocrine tumors based on the new
grading classification. J Hepatobiliary Pancreat Sci 2014; 21:418-25.
[PMID: 24142395]
- Hashim YM, Trinkaus KM, Linehan DC, Strasberg SS, Fields RC, Cao
D, et al. Regional lymphadenectomy is indicated in the surgical treatment
of pancreatic neuroendocrine tumors (PNETs). Ann Surg 2014; 259:197-203. [PMID: 24253141]
- Kishi Y, Shimada K, Nara S, Esaki M, Hiraoka N, Kosuge T. Basing
treatment strategy for non-functional pancreatic neuroendocrine tumors
on tumor size. Ann Surg Oncol 2014; 21:2882-8. [PMID: 24740828]
- Taki K, Hashimoto D, Nakagawa S, Ozaki N, Tomiyasu S, Ohmuraya M,
et al. Significance of lymph node metastasis in pancreatic neuroendocrine
tumor. Surg Today 2017; 47:1104-1110. [PMID: 28229300]
- Toste PA, Kadera BE, Tatishchev SF, Dawson DW, Clerkin BM,
Muthusamy R, et al. Nonfunctional pancreatic neuroendocrine tumors <2
cm on preoperative imaging are associated with a low incidence of nodal
metastasis and an excellent overall survival. J Gastrointest Surg 2013;
17:2105-13. [PMID: 24101447]
- Postlewait LM, Ethun CG, Baptiste GG, Le N, McInnis MR, Cardona
K, et al. Pancreatic neuroendocrine tumors: Preoperative factors that
predict lymph node metastases to guide operative strategy. J Surg Oncol
2016; 114:440-5. [PMID: 27334541]
- Jiang Y, Jin JB, Zhan Q, Deng XX, Shen BY. Impact and clinical predictors
of lymph node metastases in nonfunctional pancreatic neuroendocrine
tumors. Chin Med J (Engl) 2015; 128:3335-44. [PMID: 26668149]
- Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, et al.
DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in
pancreatic neuroendocrine tumors. Science 2011; 331:1199-203. [PMID:
21252315]
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J
Med 2014; 371:1039-49. [PMID: 25207767]
- Pea A, Hruban RH, Wood LD. Genetics of pancreatic neuroendocrine
tumors: implications for the clinic. Expert Rev Gastroenterol Hepatol
2015; 9:1407-19. [PMID: 26413978]



