Keywords
Omental flap, Roll up, Pancreatic cancer, fistula, Whipple procedure
Abbreviations
PDE Pancreaticoduodenectomy; PF Pancreatic fistula, POD Post operative day; WP Whipple procedure
INTRODUCTION
Pancreaticoduedenectomy (PDE) or Whipple procedure (WP) remains the procedure of choice and the only therapeutic option that obtains long survival in pancreatic-head cancer. It is currently performed at specialized centers and carries a mortality of less than 5%. Despite the evolution in surgery the morbidity rates remain high, ranging from 30% to 65%. Because of improvements in the surgical technique and perioperative care its mortality has fallen dramatically to 5%. The three most common complications following a WP are the formation of pancreatic fistula ranging from 5% to 53%, delayed gastric empting with a 25% rate as well as postoperative bleeding ranging from 1% to 10%.
Few studies have been published describing the benefits of wrapping the omentum around the anastomosis. Quite recently in 2014 a meta-analysis and systematic review of the literature, concluded that there is no clear evidence that omental wrapping can prevent pancreatic fistulas after WP.
In our prospective consecutive case series study we compare the frequency of pancreatic fistula formation between patients undergone omental roll up of the pancreatojejunostomy and the ones who have not.
MATERIALS AND METHODS
Study Group
From January 2010 to May 2016, twenty-two (n=22) patients underwent pancreatoduodenectomy (PDE) in our department. Seventeen patients underwent surgery due to adenocarcinoma of the pancreas and five patients due to carcinoma of the Vater. The patients were divided into two groups. The first group consisting of seven patients (n=7) underwent PDE without using the omental flap technique, within a period of time from January 2010 till December 2011. The second group consisting of fifteen patients (n=15), underwent PDE using the omental roll-up technique, within a period of time between January 2012 and May 2016. The perioperative as well as the postoperative outcome of these two groups were compared. A prospective consecutive case series was conducted.
Parameters Measured
Preoperatively the patients underwent a full check up with lab results as well as ECG (echocardiogram), chest X-ray, spirometry and CT scan of chest and abdomen. Moreover albumin levels and cancer markers (CEA, Ca 19-9, aFP) where measured in all 22 of the patients. The nutritional status of the patients was evaluated.
Perioperatively blood tests where measured to evaluate the need for blood transfusion as well as to check the levels of the electrolytes and the renal/liver function. Furthermore, the pancreatic tissue was evaluated as hard or soft by the surgeon with palpation. The pancreatic duct was also measured and evaluated as dilated (diameter >3 mm) or not dilated (diameter <3 mm). Moreover, the bile duct was measured and evaluated as dilated or not. The infusion of somatulin analogue was also evaluated.
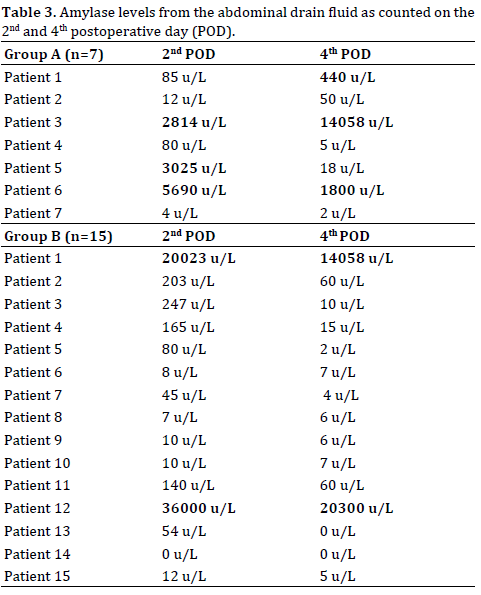
Postoperatively blood tests where counted daily as well as the amylase levels of the fluid coming out of the drainage on the 2nd and 4th postoperative day. The wound was evaluated as well as the nutritional status. Postoperatively all the patients remained in the (Intensive Care Unit) ICU for monitoring. According to our protocol, amylase levels from the abdominal drain fluid where measured on the 2nd and 4th postoperative day. The drain was removed on the 5th - 7th postoperative day when no fistula was detected. Otherwise the drainage was maintained intact. On the 5th - 7th postoperative day the patients underwent upper gastrointestinal tract pacification with water-soluble contrast to visualize a potential anastomotic leak.
Surgical Procedure
Preoperatively all the patients received prophylactic antibiotic therapy as well as intestinal preparation, intravenous hydration and respiratory physiotherapy. Right before the surgery, epidural analgesia was conducted, a urine catheter and a nasogastric tube were placed as well as a central venous catheter and an arterial catheter. Intraoperatively the patients underwent Traverso procedure as described in the literature. A Kocher-Chevron incision was conducted 2cm below the costal margin. Cholecystectomy was performed as well as excision of the head and neck of the pancreas and duodenectomy removing the 2nd, 3rd and 4th part of the duodenum. The hepatic artery, the portal vein, the celiac trunk and the superior mesenteric artery where routinely skeletonized. The pylorus was preserved as well as 2 cm of the 1st part of the duodenum. Later on, the jejunum helix was mobilized and three anastomosis where conducted: an endsided pancreatojejunostomy, an endsided choledochojejunostomy as well as an endsided duodenojejunostomy. The nasogastric tube was inspected within the stomach and was set with a stitch on patients’ nose. A feeding jejunostomy was performed using either a Folley catheter or a jejunostomy set when available. Before closing, an abdominal drain was placed through the hiatus of Winslow near the right side of the pancreaticojejunostomy.
Omental Roll-Up Technique
After performing all three of the anastomosis and the peritoneal cavity was washed up with water for injection, the greater omentum, which was detached from the colon to reveal the lesser epiploic sac, was divided using a Ligasure Precise, longitudinally up to the left gastroepiploic vessels which were systematically preserved (Figure 1). The flap which was evaluated viable, was then mobilized and placed circumferentially anteriorly on the pancreaticojejunostomy and fixed by three non-absorbable sutures (Figures 2ab).
Figure 2(ab). Roll up in pancreaticojejunostomy.
RESULTS
Patients’ Characteristics
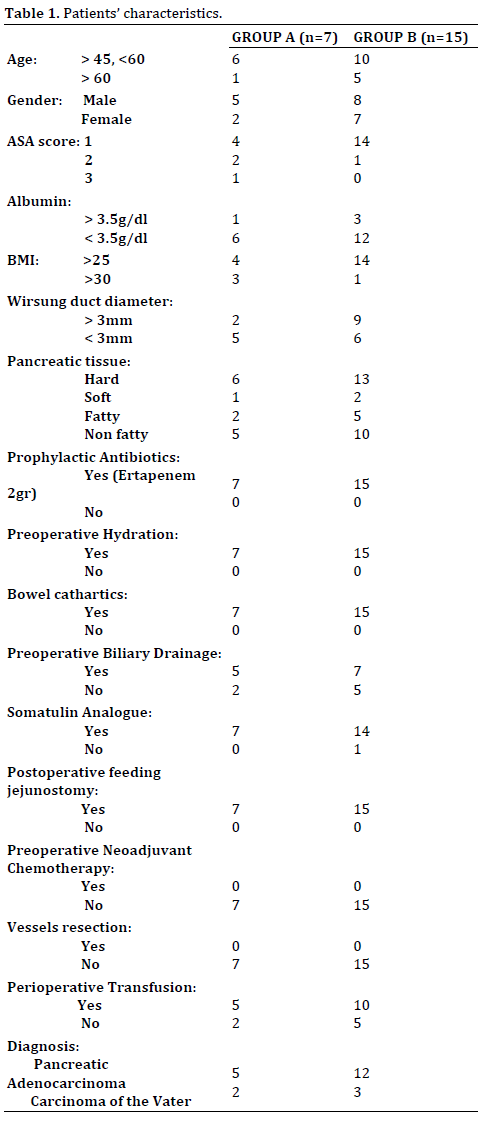
The 1st group (Group A) consisted of seven patients, five of which were males and two of which were females. The 2nd group (Group B) consisted of fifteen patients - eight of which were males and seven were females. All patients aged >45 years old. ASA score was 1 in eighteen patients (four from Group A and fourteen from Group B), 2 in three patients (two from Group A and one from Group B) and 3 in one patient (from Group A) (Table 1). Eighteen patients where malnourished (Albumin level was counted preoperatively as well as BMI) (four from Group A and fourteen from Group B) while four patients were overweight (30>BMI>25) (three from Group A and one from Group B). The diameter of Wirsung duct was dilated >3 mm in eleven patients (two from Group A and nine from Group B) while normal in the other eleven study patients. Two patients from Group A and five patients from Group B had a fatty pancreas. All of the twenty two patients preoperatively where infused with prophylactic antibiotic Ertapenem 2gr and received intravenous hydration and bowel preparation with cathartics. Furthermore preoperative biliary drainage was performed in twelve patients in total (five from Group A and seven from Group B). Nineteen patients had a hard pancreatic tissue (six from Group A and thirteen from Group B) while three patients has a soft pancreas (one from Group A and two from Group B). Somatulin analogue was infused perioperatively in twenty one of the patients while one patient from study Group B received no analogue. All of the twenty two patients postoperatively carried a feeding jejunostomy. None of the patients required portal vein or arterial resection. None of the patients either from Group A or from Group B received preoperative chemotherapy.
Postoperative Results
All of the twenty two patients remained postoperatively routinely in the Intensive Care Unit (ICU) for 24 hourmonitoring. Overall morbidity in the Group A was measured 71.4% and in the Group be it was counted 26.6%. In details, four patients from Group A developed pancreatic fistula versus two patients from Group B (Table 2). The pancreatic fistula where detected by measuring the amylase levels from the abdominal drain fluid on the 2nd and 4th postoperative day. The amylase levels (u/L) are presented in Table 3. Four patients from Group A developed pancreatic fistula in comparison with two patients from Group B who underwent PDE with the roll up technique. Moreover, one patient from each group appeared with postoperative bleeding due to splenic vessels and passed away. None of the patients presented with delayed gastric empting as proved with undergoing upper gastrointestinal tract opacification with watersoluble contrast to visualize a potential anastomotic leak. One patient from each group developed intra abdominal collection as appeared in the abdominal ultrasound and was imbibed (absorbed) on the 6th POD on both cases. Perianastomotic collection was observed on the 4th POD in two patients of Group B versus four patients from Group A. These patients where the ones who developed pancreatic fistula. Dysfunction of the feeding jejunostomy was observed. The jejunostomy was either removed or kept closed. Most patients were discharged within 12 days postoperatively.

The univariate analysis revealed that patients who underwent PDE using the omental flap technique appeared to develop less postoperative complications specifically lower percentage of pancreatic fistula or anastomotic leaks and less days of hospitalization.
DISCUSSION
The great omentum could be characterized as the “Knight of the Abdominal Cavity” since it has several advantages and offers plenty of benefits. In details the omentum offers the benefits of proper vascularization, neovascularization, prothromvin activation, fluid absorbance, formation of adhesions around the anastomosis offering protection as well as protection against infections and acceleration of the healing process [1, 2, 3]. First described by Moriura et al. in 1994, wrapping in pancreatic surgery involves the use of the omentum or the falciparum ligament to wrap the panceraticojejunostomy as well as local retroperitoneal vessels [3, 4, 5]. This technique mostly popular in Asia rather than in Europe or in USA, offers two purposes; Firstly, it reduces the rate of postoperative hemorrhage avoiding the slipping of vascular ligatures due to the action of pancreatic juices. Secondly, this technique decreases the formation of pancreatic fistula around the pancreaticojejunostomy preventing serious complications [2, 4, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16]. Of course, many studies are in progress since no clear evidence exists at present, proving the benefits of this technique.
Pancreatic fistula formation is the most serious complication following PDE. It is accompanied by a high rate of mortality that ranges from 8% to 28%. Its direct and indirect morbidity rates are also high as it causes intra-abdominal infection often accompanied by bleeding of the great abdominal vessels in 16-40% of the patients [2, 5, 6, 7, 17, 12]. Factors that may lead to formation of pancreatic fistula are small pancreatic duct (diameter <3 mm), soft pancreatic parenchyma, postoperative bleeding, heart disease, advanced age and need for transfusion perioperatively [2, 6, 12, 16].
Many technical variations have been tested in order to create a safe anastomosis between the pancreas and the jejunum just to avoid the formation of pancreatic fistula; various types of pancreaticojejunostomy like end-to-end/ end-sided/nucleation of the pancreas or duct to mucosa anastomosis or even the use tutors/biological adhesives, duct occlusion, external drainage and many more [2, 7, 12, 15, 16, 17]. One of the above techniques which are quite promising is the wrapping of the omentum.
The wrapping technique involves the use of the omentum surrounding the pancreaticojejunostomy offering two main benefits: 1) placing the omentum around the pancreaticojejunostomy may form a barrier to avoid the formation of pancreatic fistula and 2) the omentum may protect the surrounding organs against the autolytic effect and proteolytic activity of the pancreatic fluids (which are rich in trypsin and elastate), especially the local vessels like gastroduodenal artery, portal vein, hepatic artery and celiac truck [2, 6, 10, 14, 15, 16, 17].
The use of the omentum has been previously described in the gastrointestinal trunk especially in colorectal anastomosis or anastomosis of the small intestine with many benefits [3]. The omental wrapping in pancreaticojejunostomy has been described in recent studies.
In their retrospective series of 54 pancreaticoduodenectomies, Kurosaki et al. in 2004 used the omentum to protect vessels, placing it in the retroperitoneum and behind the pancreaticojejunostomy. The pancreatic fistula rate was 9.3% and there was no bleeding [17].
In 2005, Maeda et al. conducted a prospective series of 100 pancreaticoduodenectomies reporting a technique, dividing the greater omentum in order to create a flap that is positioned in front of the vessels (portal vein and hepatic artery) and behind the anastomosis in contact with the posterior face of the pancreaticojejunostomy and the hepaticojejunostomy without covering the front face of the pancreaticojejunostomy, covering and protecting arterial stumps such as the gastroduodenal artery stump. In the article, the authors stress the need to ensure that the stomach is not torsioned. They fix the flap only if it is deemed necessary and perform Doppler ultrasound during and after surgery to ensure proper portal flow. In this study, the pancreatic fistula rate was 15% and the post-operative bleeding rate was 1%. The only patient who presented bleeding had a body mass index of 15, and the omentum was extremely thin. The authors concluded that wrapping is effective for preventing bleeding but not for diminishing pancreatic fistula [6].
One year later, in 2006, Kapoor et al. presented a prospective series of 77 pancreaticoduodenectomies, in 25 of which a double omental flap was used: one wrap to cover pancreaticojejunostomy, and the other covering the duodenojejunostomy. No complications were reported. The pancreatic fistula rate was similar in the wrapping and non-wrapping groups, but the fistulas were less severe in patients with wrapping. The rates of bleeding and mortality were similar in the two groups, but there was no mortality related to post-operative bleeding in the wrapping group [7].
In 2011 Mimatsu et al. performed a prospective study (20 pancreatoduodenectomies) in which the omentum and FL were used together to protect vessels and the pancreatogastrostomy. They obtained a pancreatic fistula rate of 10% and no post-operative bleeding was recorded. Nor were there any complications associated with the double wrapping [18].
In 2012, Tani et al. conducted a multi-centre retrospective study of 2597 patients who underwent pancreatic surgery. Wrapping with omentum and/or Falciparum Ligament, was performed in 918 patients. Wrapping patients had a longer operative time, a higher PF rate, more severe fistulas and more wound infection. Interestingly, the amylase level in the drainage was lower in the group with wrapping. The location of the wrapping (vessel protection or peri-anastomotic) did not change the complication rate, which was higher in the group with wrapping in all cases. Wrapping did not decrease the postoperative bleeding rate [14].
Within the same year, three more studies were conducted. Choi et al. presented a retrospective series of 68 pancreaticoduodenectomis, dividing the patients into two non-randomized but comparable groups. In the first group, an omental flap was wrapped around the pancreaticojejunostomy to protect the anastomosis and to decrease the rate of pancreatic fistula, and also to protect retroperitoneal vessels. In the second group, the omental roll was not used. The overall pancreatic fistula rate for the series was high (42.3%). The group of patients who underwent omental wrapping of the pancreaticojejunostomy showed a significantly lower rate of fistulas (20.7% versus 59%), less severe fistulas (grade A) and shorter hospital stay. There was no difference in post-operative bleeding rate [12]. Also Rosso et al. presented a prospective series of 61 pancreaticoduodenectomies in which there were compared 33 patients with a double omental flap versus 28 patients without wrapping. The double flap protected regional vessels and pancreaticojejunostomy anastomosis. Morbidity rate was 27.8% and the pancreatic fistula rate was 13.1%. The omental flap group presented a reduced rate of relaparotomy (10.7% versus 0%) and perianastomotic collections, but more pleural effusions [19]. Matsuda et al. published a retrospective series of 229 patients, in 157 of which an omental flap was performed to protect regional vessels. The overall pancreatic fistula rate was 35.4% and the post-operative bleeding rate was 3.9%. The rate of bleeding in the group without the flap was 8.3%, compared with 1.9% in the group with the flap [5].
CONCLUSION
To summarize, the great omentum represents the “Knight of the Abdominal Cavity” and is characterized by many advantages. Its use in visceral surgery is undoubtedly, beneficial. The wrapping of the omentum, however, in oncologic pancreatic surgery is scarce. In bibliography, few studies have been reported. These studies are retrospective and prospective and not randomized. Thus there are no control groups, so their level of evidence is low. Different types of pancreatic surgery are also mixed up as well as various wrapping techniques, making it difficult to compare the results.
In the existing bibliography, wrapping of the omentum is in favor of the reduction pancreatic fistula after pancreaticoduodenectomis. However, more randomized controlled studies are needed.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Liebermann-Meffert D. The greater omentum. Anatomy, Embryology, and surgical applications. Surg Clin North Am 2000; 80:275-93, xii. [PMID: 10685153]
- Ramia JM, de la Plaza R, Adel F, Ramiro C, Arteaga V, Garcia-Parreño J. Wrapping in pancreatic surgery: a systematic review. ANZ J Surg 2014; 84:921-924. [PMID: 25720806]
- Moriura S, Ikeda S, Ikezawa T, Naiki K. The inclusion of an omental flap in pancreatoduodenectomy. Surg. Today 1994; 24:940-1. [PMID: 7894198]
- Abe N, Sugiyama M, Suzuki Y, Yanagida O, Masaki T, Mori T, Atomi Y. Falciform ligament in pancreatoduodenectomy for protection of skeletonized and divided vessels. J Hepatobiliary Pancreat Surg 2009; 16:184-8. [PMID: 19169616]
- Matsuda H, Sadamori H, Umeda Y, Shinoura S, Yoshida R, Satoh D, Utsumi M, et al. Preventive effect of omental flap in pancreaticoduodenectomy against postoperative pseudoaneurysm formation. Hepatogastroenterology 2012; 59:578-83. [PMID: 21940374]
- Maeda A, Ebata T, Kanemoto H, Matsunaga K, Bando E, Yamaguchi S, Uesaka K. Omental flap in pancreaticoduodenectomy for protection of splachnic vessels. World J Surg 2005; 29:1122-6. [PMID: 16132400]
- Kapoor VK, Sharma A, Behari A, Singh RK. Omental flaps in pancreaticoduodenectomy. JOP 2006 10; 7:608-15. [PMID: 17095840]
- Iannitti DA, Coburn NG, Somberg J, Ryder BA, Monchik J, Cioffi WG. Use of the round ligament of the liver to decrease pancreatic fistulas: a novel technique. J am Coll Surg 2006; 203:857-64. [PMID: 17116554]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20-5. [PMID: 17629996]
- Abe N, Sugiyama M, Yanagida O, Masaki T, Mori T, Atomi Y. Wrapping of skeletonized and divided vessels using the falciform ligament in distal pancreatectomy. Am J Surg 2007; 194:94-7. [PMID: 17560917]
- Liang TB, Bai XL, Zheng SS. Pancreatic fistula after pancreaticojejunostomy: diagnosed according to International Study Group Pancreatic Fistula (ISGPF) definition. Pancreatology 2007; 7:325-34. [PMID: 17627097]
- Choi SB, Lee JS, Kim WB, Song TJ, Suh SO, Choi SY. Efficacy of the omental roll-up technique in panceraticojejunostomy as a strategy to prevent pancreatic fistula after pancreaticoduodenectomy. Arch Surg 2012; 147:145-50. [PMID: 22351908]
- Walters DM, Stokes JB, Adams RB, Bauer TW. Use of falciform ligament pedicle flap to decrease pancreatic fistula after distal pancreatectomy. Pancreas 2011; 40:595-9. [PMID: 21499214]
- Tani M, Kawai M, Hirono S, Hatori T, Imaizumi T, Nakao A, Egawa S et al. Use of omentum or falciform ligament does not decrease complications after pancreaticoduodenectomy: nationwide survey of the Japanese Society of Pancreatic Surgery. Surgery 2012; 151:183-91. [PMID: 21982073]
- Tian Y, Ma H, Peng Y, Li G, Yang H. Preventive effect of omental flap in pancreaticoduodenectomy against postoperative complications: a metaanalysis. Hepatogastroenterology 2015; 62:187-9. [PMID: 25911894]
- Fu SJ, Shen SL, Li SQ, Hu WJ, Hua YP, Kuang M, Liang LJ et al. Risk factors and outcomes of postoperative pancreatic fistula after pancreatico-duodenectomy: an audit of 532 consecutive cases. BMC Surg 2015 15:34. [PMID: 25887526]
- Kurosaki I, Hatakeyama K. Omental wrapping of skeletonized major vessels after pancreaticoduodenectomy. Int Sutg 2004; 89:90-4. [PMID: 15285241]
- Mimatsu K, Oida T, Kano H, Kawasaki A, Fukino N, Kida K, Kuboi Y et al. Protection of major vessels and pancreaticogastrostomy using the falciform ligament and greater omentum for preventing pancreatic fistula in soft pancreatic texture after pancreaticoduodenectomy. Hepatogastroenterology 2011; 58:1782-6. [PMID: 21940349]
- Rosso E, Lopez P, Roedlisch MN, Narita M, Oussoultzoglou E, Bachellier P. Double omental flap reduced perianastomotic collections and relaparotomy rates after pancreaticoduodenectomy with pancreatostomy. World J Surg 2012; 36:1672-8



