Keywords
Jaundice, Obstructive; Lymphoma, Large B-Cell, Diffuse;
Lymphoma, Non-Hodgkin; Pancreatic Neoplasms
Abbreviations
BMCB bone marrow aspirate/biopsy; CNB core needle
biopsy; CT computerized tomography; DLBCL diffuse large B-cell
lymphoma; ERCP endoscopic retrograde cholangiopancreatography;
FDG-PET fluorodeoxyglucose positron emission tomography; FNAC
fine needle aspiration cytology; MRI magnetic resonance imaging;
NHL non-Hodgkin's lymphoma; PPL primary pancreatic lymphoma;
PTC percutaneous transhepatic catheter; RECIL Response Evaluation
Criteria In Lymphoma; TB total bilirubin
INTRODUCTION
Lithiasis is the most common cause of obstructive
jaundice followed by tumors. However, obstruction
by lymphoproliferative processes is extremely rare,
especially if it is a retroperitoneal lymphoma. Besides,
diffuse large B-cell lymphoma (DLBCL) primarily arising
in the retroperitoneal region has been rarely reported.
Lymphoma is a heterogeneous neoplasms group
originating from lymphocytes [1] and until 40% of all patient
with lymphoma have an extranodal lymphoma. DLBCL
is the most common histological subtype of NHL [2]. The
retroperitoneal localization is extremely rare and its diagnosis
is often difficult [3, 4]; during postKmortem studies of NHL
patients an incident of less than 1% was noted [3]. It often
requires a time consuming and costly diagnostic workup.
We report the clinical case of a female who presented
to our hospital with jaundice due to a retroperitoneal
lymphoma. It invaded the pancreas and simulated a
primary pancreas tumor.
CASE REPORT
A Sixty-three-year-old female presented with 7-day
history of obstructive jaundice and soft abdominal pain.
The patient denied any other symptomatology. Ultrasound
of the abdomen revealed a mass in the head of the pancreas.
Laboratory tests showed direct hyperbilirubinemia,
mild elevation of transaminases and significant elevation
of alkaline phosphatase, indicating obstructive jaundice.
Carbohydrate antigen 19-9, Carbohydrate antigen 125
and beta-2 microglobulin were elevated (103 IU/mL,
75.5 IU/mL and 2.65 mg/L respectively). There was also
coagulation times alteration (Prothrombin Time 16.20
seconds, INR 1.4, activated Partial Thromboplastin Time
38 seconds).
Computerized tomography (CT) showed a mass of soft
tissue density contacting the pancreas head, from which it
seems to depend, and dilating the common bile duct. This
mass also included inferior vena cava and the aorta and
displaced the mesenteric vessels. Other metastatic lesions
were not observed (Figure 1).
Figure 1. Computerized tomography showed a mass contacting the pancreas head, from which it seems to depend.
Fine needle aspiration cytology (FNAC) under control
by endoscopic ultrasound was negative for neoplastic
cell. Some days later, a ERCP (endoscopic retrograde
cholangiopancreatography) was performed, and we observed a deformation by compression of the bulb and
second duodenal portion, without being able to cannulate
the papilla. Percutaneous transhepatic catheter (PTC) of
the bile duct and core needle biopsy (CNB) was performed.
At that time, total bilirubin (TB) was at 21.31 mg/dl
and direct bilirubin was at 20.6 mg/dl. New magnetic
resonance imaging showed an increase of the lesion from 9
to 13 cm in its major axis in less than fifteen days. The CNB
sample was positive for diffuse large B-cell lymphoma.
The immunohistochemical staining was positive for the
following antigens: CD20, bcl-6, MUM-1 and bcl-2. It was
negative for CK, CD3, Cd5, CD10 and CD23. Ki67 (cell
proliferation index) was higher than 90% (Figures 2, 3).
Figure 2. (a, b). Hematoxylin eosin. Discohesive cell population of atypical large lymphocytes. CD20 positive shows the nature B of lymphocytes. CD5 negative shows the low cellularity of T lymphocytes.
Figure 3. Cell proliferation index (Ki67) higher than 90%.
Bone marrow aspirate/biopsy (BMAB) was negative.
FDG-PET (Fluorodeoxyglucose positron emission
tomography) was performed and, in addition to the
retroperitoneal lesion, showed a right femur metastasis.
Based on these data, the disease was stage IV, according to
the Ann Arbor classification.
Twelve days after PTC, when TB decreased to 4.49 mg/dl,
the patient was treated by Rituximab-CHOP chemotherapy.
The dose was adjusted by hyperbilirubinemia: standard
dose of rituximab, 1000 mg cyclophosphamide
intravenously, 1 mg vincristina intravenously and 25%
of doxorubicin dose intravenously on day 1. In the third
cycle, it was possible to continue with full doses since
bilirubin had normalized. In addition, from the beginning
of rituximab, we had to start treatment with lamivudine
for positive hepatitis B virus serology (Anti-HBc and Anti-
HBs positive), and it should be continued until 12 months
after the last dose of rituximab, as a VHB reactivation
prophylaxis. Epstein Barr virus, hepatitis C virus and
HIV were negative. At the fourth cycle of chemotherapy, according to the standard RECIL (Response Evaluation
Criteria In Lymphoma) criteria, our patient presented a
partial response, with a significant reduction in tumor size
(4.2×4.8×10 cm, previously 9.2×10×14.8 cm). PTC could
be removed in the sixth cycle, when a plastic prosthesis
could be placed by ERCP due to the decrease in tumor size.
The patient has completed eight chemotherapy cycles and
now radiotherapy is being performed. From the moment
of diagnosis, the patient has a 10-month of follow-up
with good performance status and stable tumor size since
fourth chemotherapy cycle.
DISCUSSION
A primary retroperitoneal localization of non-
Hodgkin's lymphoma (NHL) is quite rare and, according to
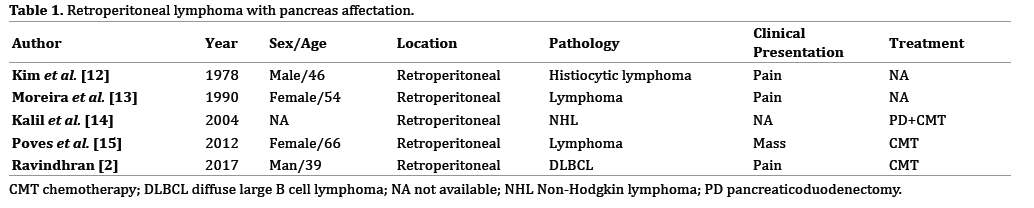
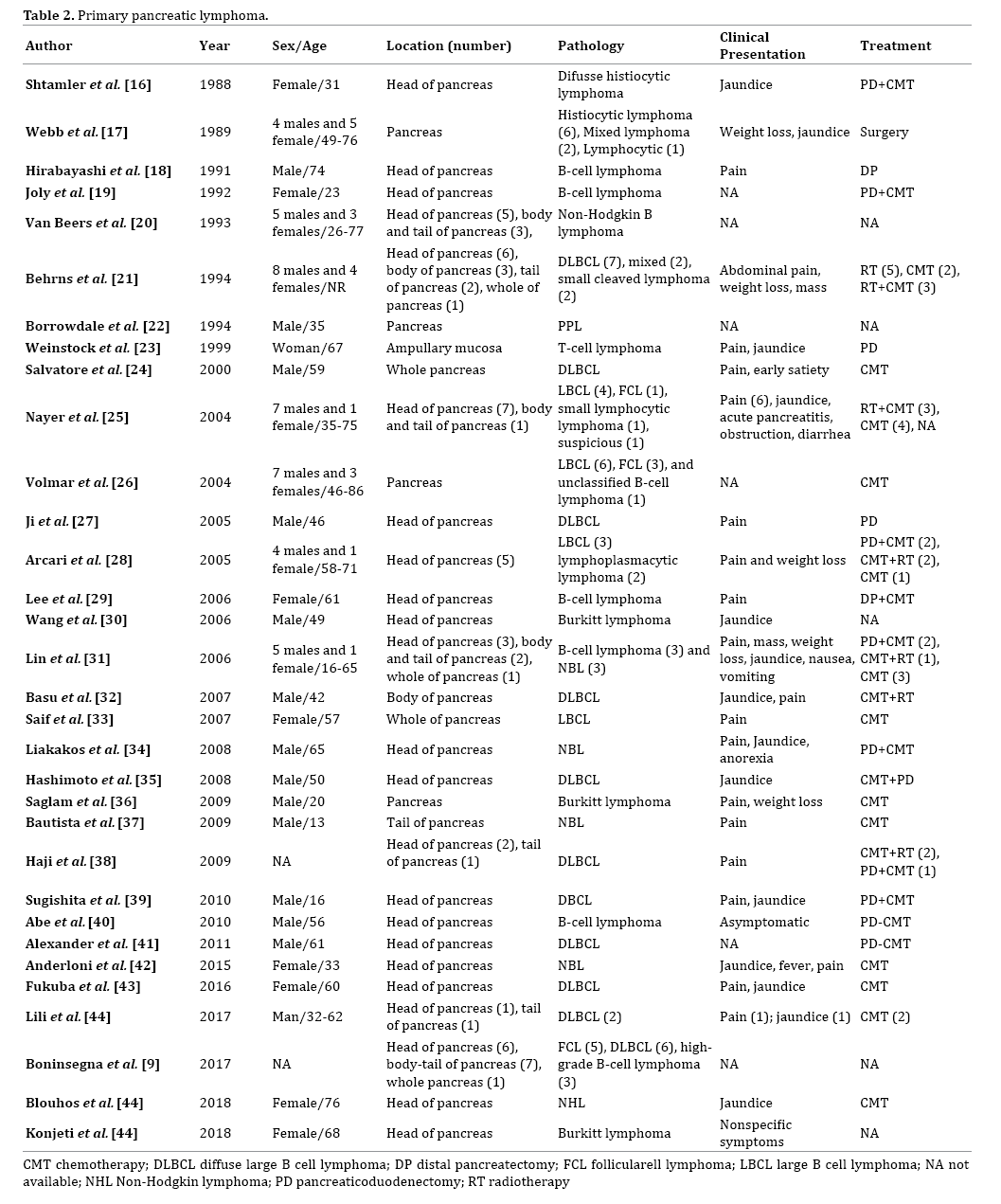
our knowledge and after review of literature (Tables 1, 2),
a retroperitoneal diffuse large B-cell lymphoma (DLBCL)
with pancreatic invasion and obstructive jaundice has not
yet been described.
Lymphoma is a heterogeneous neoplasms group
originating from lymphocytes [1] and until 40% of all
patient with lymphoma have an extranodal lymphoma.
DLBCL is the most common histological subtype of
NHL [2]. Nearly 70% of lymphomas present a generally
multilocalized, single or multiple lymphoadenomegaly,
with involvement in almost 30-40% of latero-cervical
lymphonodes. The retroperitoneal localization is extremely
rare and its diagnosis is often difficult [3, 4]; during postmortem
studies of NHL patients an incident of less than
1% was noted [3]. It often requires a time consuming and
costly diagnostic workup. On the other hand, primary
pancreatic lymphomas (PPL) is a rare entity that accounts
for about 0.5% of pancreatic tumors [5] and less than 1% of NHL [6]. Although almost 30% of NHL can affect to the
pancreatic gland, less than 1% are considered PPL [5]. The
PPL diagnosis needs the next criteria: dominant mass in
the pancreas, the absence of superficial or mediastinal
lymphadenopathy on chest imaging, a normal leukocyte
count in the peripheral blood, and the absence of hepatic
or splenic involvement [7, 8]. Our patient had a large size
neoplasm that invaded the pancreas (initially without being
able to rule out a primary pancreatic neoplasm, although
the radiological behaviour was not typical and the major volume of tumor was out pancreas), and that produced
the displacement of the pancreatic head which caused
obstruction of the bile duct, with secondary jaundice.
The incidence of NHL has increased approximately 80%
since the 1970s [7]. The stage of the disease is classified
according to the Ann Arbor staging system. Due to the
uncommon anatomical location and the lack of symptoms
in many of them for a long time, the diagnosis is usually
late and the management of these patients is difficult. First
presentation of NHL varies depending on the subtype
and involved area [3]. Probably, although our patient had
metastatic involvement at diagnosis, if the patient had
not presented jaundice, she would have diagnosed later,
because she was asymptomatic.
Morphologic tests (contrast-enhanced CT or magnetic
resonance imaging (MRI)) are necessary for the
diagnostic because they allow the lesion localization and
characterization. CT is the diagnostic modality of choice,
but MRI offers superior soft-tissue contrast in comparison
with CT [9]. However, biopsy is the tool that offers the
definitive diagnosis [1]. The radiological behaviour
of our patient's tumor was not typical of pancreatic
adenocarcinoma, since it displaced nearby structures but
did not invade them. It only invaded the pancreas. The
biopsy confirmed our suspicion.
Complete diagnostic evaluation requires the use of
FDG-PET, a functional metabolic imaging test, which
combined with computed tomography (PET-CT), has
become standard pre-treatment imaging in DLBCL and
may be a noninvasive alternative to BMAB to ascertain
bone marrow involvement [1, 4, 10] . FDG-PET is an useful
staging, prognostic and evaluation of response tool [1].
The poly-chemotherapy with CHOP represent the
standard chemotherapy regimen for NHL treatment. It
obtains a complete response in about 45-53% of cases,
with a long– term survival of 30-37%, and few sideeffects
[4]. New strategies with rituximab combination are
being used to improve the prognosis of these patients [3].
Generally, the correct therapeutic approach to the extranodal
NHL requires the integration of chemotherapy,
radiotherapy and surgery, but it is the disease localization
that will determine treatment choice [3, 4]. On the other
hand, lamivudine should be used as a VHB reactivation
prophylaxis in patients with rituximab treatment [11].
CONCLUSION
The prognosis has improved in recent years owing to
the development of various aggressive chemotherapeutic
regimens depending on the histological type, stage and
age of each patient. Therefore, a definitive histological
diagnosis is essential for the survival of patients with
DLBLC and it should be included in the differential
diagnosis of pancreatic tumor.
Author Contributions
All authors have contributed equally to writing the
manuscript.
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Vinnicombe SJ, Reznek RH. Computerised tomography in the staging of Hodgkin's disease and non-Hodgkin's lymphoma. Eur J Nucl Med Mol Imaging 2003;30:42–55. [PMID: 12709830]
- Ravindhran B, Prakash C, Govindharaj S, Shawnaz Bahnou NM, Pavithra B. An Aggressive Primary Retroperitoneal Diffuse Large B-Cell Lymphoma Mimicking a Pancreatic Neoplasm, Presenting as Duodenal Stenosis. J Clin Diagn Res 2017;11:9-11. [PMID:29207777]
- Cai YL, Xiong XZ, Lu J, Lin YX, Cheng NS. Non-Hodgkin's lymphoma with uncommon clinical manifestations: A case report. Oncol Lett 2015;10:1686–1688. [PMID: 26622732]
- Fulignati C, Pantaleo P, Cipriani G, Turrini M, Nicastro R, Mazzanti R, et al. An uncommon clinical presentation of retroperitoneal non-Hodgkin lymphoma successfully treated with chemotherapy: a case report. World J Gastroenterol 2005;11:3151–3155. [PMID: 15918208]
- Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas of the pancreas. Cancer1972;29:252-260. [PMID: 5007387]
- Yu L, Chen Y, Xing L. Primary pancreatic lymphoma: two case reports and a literature review. Onco Targets Ther 2017;10:1687–1694. [PMID: 28356755]
- Chiu BC, Weisenburger DD. An update of the epidemiology of non-Hodgkin's lymphoma. Clin Lymphoma 2003; 4:161-168. [PMID: 14715098]
- Yu L, Chen Y, Xing L. Primary pancreatic lymphoma: two case reports and a literature review. Onco Targets Ther 2017;10:1687–1694. [PMID: 28356755]
- Boninsegna E, Zamboni GA, Facchinelli D, Triantopoulou C, Gourtsoyianni S, Ambrosetti MC, et al. CT imaging of primary pancreatic lymphoma: experience from three referral centres for pancreatic diseases. Insights Imaging 2018; 9:17–24. [PMID: 29335928]
- Vishnu P, Wingerson A, Lee M, Mandelson MT, Aboulafia DM. Utility of Bone Marrow Biopsy and Aspirate for Staging of Diffuse Large B Cell Lymphoma in the Era of Positron Emission Tomography With 2-Deoxy-2-[Fluorine-18] fluoro-deoxyglucose Integrated With Computed Tomography. Clin Lymphoma Myeloma Leuk 2017;17:631-636. [PMID: 28684378]
- Loomba R, Liang TJ. Hepatitis B Reactivation Associated With Immune Suppressive and Biological Modifier Therapies: Current Concepts, Management Strategies, and Future Directions. Gastroenterology 2017;152:1297–1309. [PMID: 28219691]
- Kim EE, DeLand FH. Retroperitoneal lymphoma involving páncreas-Complementary radionuclide scan and ultrasonography. Oncology 1978;35:271-273. [PMID: 370705]
- Moreira VF, López-San Román A, Ledo L, Meroño E, Erdozain JC. Retroperitoneal lymphoma causing pancreatic ductal obstruction on endoscopic retrograde cholangiopancreatography. Gastrointest Endosc1990;36:80-81. [PMID: 2311899]
- Kalil AN, Reck dos Santos PA, Azambuja DB, Beck PE. A case ofretroperitoneal lymphoma presenting as pancreatic tumor. Hepatogastroenterology 2004;51:259-261. [PMID: 15011880]
- Poves I, Alonso S, Jimeno M, Bessa X, Burdio F, Grande L. Retroperitoneal inflammatory pseudotumor presenting as a pancreatic mass. J Pancreas 2012; 13:308-311. [PMID: 22572139]
- Shtamler B, Bickel A, Manor E, Ben Shahar M, Kuten A, Suprun H. Primary lymphoma of the head of the pancreas. J Surg Oncol 1988;38:48-51. [PMID: 3287006]
- Webb TH, Lillemoe KD, Pitt HA, Jones RJ, Cameron JL. Pancreatic lymphoma. Is surgery mandatory for diagnosis or treatment?. Ann Surg 1989; 209:25-30. [PMID: 2910212]
- Hirabayashi K, Kawakami H, Aizawa T. A case of the primary pancreatic lymphoma. Rinsho Ketsueki 1991;32:414–418. [PMID: 2067088]
- Joly I, David A, Payan MJ, Sahel J, Sarles H. A case of primary non-Hodgkin lymphoma of the pancreas. Pancreas 1992;7:118–120. [PMID: 1557340]
- Van Beers B, Lalonde L, Soyer P, Grandin C, Trigaux JP, De Ronde T, et al. Dynamic CT in pancreatic lymphoma. J Comput Assist Tomogr 1993;17:94– 97. [PMID: 8419447]
- Behrns KE, Sarr MG, Strickler JG. Pancreatic lymphoma: is it a surgical disease. Pancreas 1994;9:662–667. [PMID: 7809023]
- Borrowdale R, Strong RW. Primary lymphoma of the pancreas. ANZ J Surg1994.
- Weinstock LB, Swanson PE, Bennett KJ, Van Amburg A, Wald SM, Shah NB. Jaundice Caused by a Clinically Undetectable T-Cell Lymphoma Infiltrating the Sphincter of Oddi. Am J Gastroenterol 2001;11:3186-3189. [PMID: 11721770]
- Salvatore JR, Cooper B, Shah I, Kummet T. Primary pancreatic lymphoma: a case report, literature review, and proposal for nomenclature. Med Oncol 2000;17:237–247. [PMID: 10962538]
- Nayer H, Weir EG, Sheth S, Ali SZ. Primary pancreatic lymphomas: acytopathologic analysis of a rare malignancy. Cancer 2004;102:315–321. [PMID: 15386314]
- Volmar KE, Routbort MJ, Jones CK, Xie HB. Primary pancreatic lymphoma evaluated by fine-needle aspiration: findings in 14 cases. Am J Clin Pathol 2004;121:898–903. [PMID: 15198364]
- Ji Y, Kuang TT, Tan YS, Chen Y, Zeng HY, Jin DY. Pancreatic primary lymphoma: a case report and review of the literature. Hepatobiliary Pancreat Dis Int 2005;4:622–626. [PMID: 16286277]
- Arcari A, Anselmi E, Bernuzzi P, Bertè R, Lazzaro A, Moroni CF, et al. Primary pancreatic lymphoma.Report of five cases. Haematologica 2005;90:ECR09. [PMID: 15713583]
- Lee MK, Jeon SW, Lee YD, Seo HE, Cho CM, Kim SG, et al. A case of primary pancreatic non-Hodgkin’s lymphoma. Korean J Intern Med 2006;21:123–126. [PMID: 16913443]
- Wang YJ, Jeng CM, Wang YC, Chang PP, Wang TH. Primary pancreatic Burkitt’s lymphoma mimicking carcinoma with obstructive jaundice and very high CA19-9. Eur J Gastroenterol Hepatol 2006;18:537–540. [PMID: 16607151]
- Lin H, Li SD, Hu XG, Li ZS. Primary pancreatic lymphoma: report of six cases. World J Gastroenterol 2006;12:5064–5067. [PMID: 16937508]
- Basu A, Patil N, Mohindra P, Zade B, Gujral S, Muckaden MA, et al. Isolated non-Hodgkin’s lymphoma of the pancreas: case report and review of literature. J Cancer Res Ther 2007;3:236–239. [PMID: 18270400]
- Saif MW, Khubchandani S, Walczak M. Secondary pancreatic involvement by a diffuse large B-cell lymphoma presenting as acute pancreatitis. World J Gastroenterol 2007;13:4909–4911. [PMID: 17828824]
- Liakakos T, Misiakos EP, Tsapralis D, Nikolaou I, Karatzas G, Macheras A. A role for surgery in primary pancreatic B-cell lymphoma: a case report. J Med Case Rep 2008;2:167. [PMID: 18489739]
- Hashimoto M, Umekita N, Noda K. Non-Hodgkin lymphoma as a cause of obstructive jaundice with simultaneous extrahepatic portal vein obstruction: a case report. World J Gastroenterol 2008;14:4093–4095. [PMID: 18609698]
- Sağlam M, Yilmaz MI, Mas MR, Tasci L, Örs F, Sönmez A, et al. A case of pancreatic Burkitt lymphoma: radiological findings. Diagn Interv Radiol 2009;15:39–42. [PMID: 19263373]
- Bautista F, Moreno L, Andrés MM, Fernández-Navarro JM, Fernández-Sanmartín M, Verdeguer A. Abdominal pain as the first manifestation of primary pancreatic lymphoma. J Pediatr Hematol Oncol 2009 ;31:222–223. [PMID: 19262254]
- Haji AG, Sharma S, Majeed KA, Vijaykumar DK, Pavithran K, Dinesh M. Primary pancreatic lymphoma: report of three cases with review of literature. Indian J Med Paediatr Oncol 2009;30:20–23. [PMID: 20668602]
- Sugishita H, Watanabe Y, Yamamoto Y, Yoshida M, Sato K, Horiuchi A, et al. Primary pancreatic lymphoma: the role of surgical treatment. Case Rep Gastroenterol 2010;4:104–110. [PMID: 21103236]
- Abe Y, Tamura K, Sakata I, Ishida J, Mukai M, Ohtaki M, et al. Unique intense uptake demonstrated by (18)F-FDG positron emission tomography/computed tomography in primary pancreatic lymphoma: a case report. Oncol Lett 2010;1:605–607. [PMID: 22966351]
- Alexander RE, Nakeeb A, Sandrasegaran K, Robertson MA, An C, Al-Haddad MA, et al. Primary pancreatic follicle center-derived lymphoma masquerading as carcinoma. Gastroenterol Hepatol (N Y) 2011;7:834–838. [PMID: 22347825]
- Anderloni A, Genco C, Ballarè M, Carmagnola S, Battista S, Repici A. A case of primary pancreatic non-Hodgkin B-cell lymphoma mimicking autoimmune pancreatitis. J Gastrointestin Liver Dis 2015;24:245–248. [PMID: 26114186]
- Fukuba N, Moriyama I, Ishihara S, Sonoyama H, Yamashita N, Tada Y, et al. Primary pancreatic malignant lymphoma diagnosed from endoscopic ultrasound-guided fine-needle aspiration findings. Intern Med 2016;55:31–35. [PMID: 26726082]
- Blouhos K, Boulas KA, Paraskeva A, Kariotis I, Barettas N, Hatzigeorgiadis A. Obstructive jaundice as primary presentation of a stage IIE Non-Hodgkin lymphoma: A decision making process between advanced lymphoma and locally advanced/metastatic pancreatic adenocarcinoma. Int J Surg Case Rep 2018;44:226-229. [PMID: 29547849]
- Konjeti VR, Hefferman GM, Paluri S, Ganjoo P. Primary Pancreatic Burkitt's Lymphoma: A Case Report and Review of the Literature. Case Rep Gastrointest Med 2018. [PMID: 29593916]




