Keywords
Alkylating Agents; Meta-Analysis, Neuroendocrine Tumors;
O(6)-Methylguanine-DNA Methyltransferase
INTRODUCTION
Neuroendocrine tumors (NETs) are a group of rare and
heterogeneous tumors. According to the National Cancer
Institute Surveillance, the incidence rate of NET is 0.43
patients per 100000 persons, which is double than that
seen 20 to 30 years ago [1] . Based on the primary tumor
site, NETs can be divided into subgroups, such as pancreatic
NET (pNET) and gastrointestinal NET (GI-NET). In China,
pNET is the most common form, which accounts for 49.8%
of the total patients with NET in the country [2]. Alkylating
agent chemotherapy, particularly temozolomide-based
chemotherapy, is a standard treatment for certain NETs,
which has exhibited a promising overall response rate in
the treatment of NET [3, 4].
Temozolomide produces anti-tumor activity by
inducing DNA methylation at the O6 and N7 positions of
guanine, which leads to DNA mismatch and tumor cell
death [5, 6]. DNA repair enzyme O-6-methylguanine
DNA methyltransferase (MGMT) is crucial for genome
stability as it repairs DNA mismatch and transcription
errors [5]. MGMT removes a mutagenic alkyl group from
O6-guanine and transfers it to an active cysteine. Studies
have shown that diminished MGMT expression increases
the carcinogenic risk in mice exposed to alkylating agents
[7], whereas high MGMT expression counteracts the
therapeutic effect of alkylating agents, thus contributing to
chemoresistance [8].
Loss of MGMT expression in high-grade gliomas is
predictive of improved survival with temozolomide-based
therapy [9, 10]. However, the role of MGMT methylation
status in predicting the response to alkylating agents in
patients with NET is still controversial. And we aimed to
perform a meta-analysis of recent literature to elucidate
the relationship between the predictive efficacy of
MGMT expression and the response to alkylating agent
chemotherapy in patients with NET.
MATERIALS AND METHODS
Literature Search Strategy
We searched PubMed, Cochrane Library, and Web
of Science for articles published up to December 12,
2016. The following keywords were used in our search
strategy: (“O-6-methylguanine-DNA methyltransferase”
OR “MGMT”) AND (temozolomide OR [8-carbamoyl-3-
methylimidazo (5,1-d) -1,2,3,5-tetrazin-4 (3H) one] OR
methazolastone) AND (Neuroendocrine neoplasm[Mesh]).
We limited our search to studies written in English. The
reference lists of the selected articles were searched to
ensure that no studies were overlooked.
Selection Criteria
The meta-analysis included studies that met the
following standards: (1) all patients with NET were
diagnosed by histopathology; (2) the study reported
data of MGMT expression levels or MGMT promoter
methylation status; (3) the results were part of an original
analysis; and (4) if the same patient population was used
in several publications, then only the most complete
study was included in the meta-analysis. The exclusion
criteria were as follows: (1) publication type as abstract;
(2) studies focusing on the value of MGMT co-expression
and other factors rather than MGMT expression levels
or MGMT promoter methylation status; and (3) studies
without hazard ratios (HRs) or 95% confidence intervals
(CIs), or without a Kaplan-Meier curve to calculate these
data.
Data Extraction
Each article was reviewed independently by two
authors. If differences in opinion arose between these
two authors, then the articles were discussed with a third
author. The selected articles were assessed according to
“The Newcastle-Ottawa Scale for assessing the quality
of non-randomized studies in meta-analyses” [11]. The
following data were collected from each study: first
author’s name, country, publication year, number of
patients, primary location of NET, methodology of MGMT
analysis, and objective response rate and progression-free
survival (PFS) with HR and 95% CI. If the prognostic data
were not directly expressed, we obtained the data from
Kaplan-Meier curves (using Engauge Digitizer version 4.1)
and calculated the HR and 95% CI by previously reported
methods [12].
Statistical Analysis
Based on immunohistochemistry cut-off values used in
each study, we categorized the expression of MGMT as either
“deficient” or “intact”. The MGMT promoter methylation
was determined as “methylation” or “non-methylation” by
pyrosequencing or quantitative methylation-specific PCR.
The end-points were objective response rate and PFS; and
the association between MGMT and clinical outcome was
evaluated by using the HR of negative/methylation MGMT
status over positive/non-methylation MGMT status and
the 95% CI. Multivariate Cox proportional hazards models were applied for this purpose. For patients with a positive/
non-methylation status, a HR greater than one with a 95%
CI that did not overlap with one implied a good predictive
value, whereas an HR lower than one with a 95% CI that did
not overlap with one indicated a poor outcome in survival.
An HR of one indicated a lack of association between MGMT
expression and clinical prognosis. All data were synthesized
by Review Manager (version 5.2). The Mantel-Haenszel
test was used to test significance; a p<0.05 was considered
statistically significant. Statistical heterogeneity was assessed
by the visual inspection of forest plots, by performing the χ2
test, and by calculating the I2 value. Significant heterogeneity
across studies was indicated by p<0.1 or I2>50% and a
random-effects model was performed to calculate the pooled
estimate; otherwise, the heterogeneity is not significant and a
fixed-effects model was applied.
RESULTS
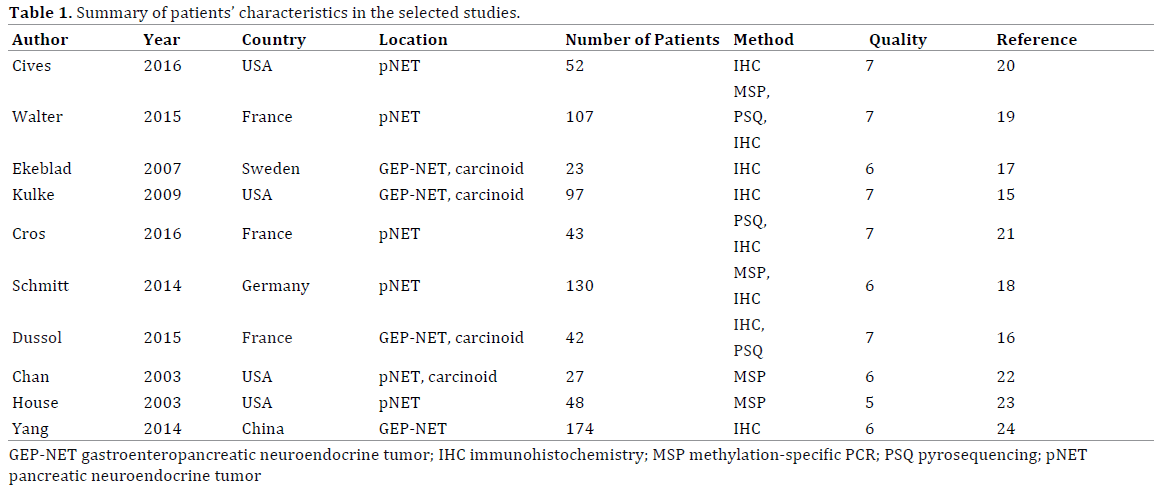
Characteristics of Studies
A flow chart of the study selection criteria is shown
in Figure 1. Twelve articles with a total of 835 patients
with NET were chosen based on the eligibility criteria;
all studies tested MGMT expression or MGMT promoter
methylation status. One article was excluded because it
involved neuroendocrine cancer(NEC) patients [13]. One
article was excluded because of unavailable data on MGMT
expression level [14]. Thus ten articles were included in
expression analysis. Seven articles with 519 patients with
NET included objective response rate data [15, 16, 17, 18, 19, 20, 21]. Four articles with 289 patients with NET included
PFS data [15, 16, 19, 21]; Two of these directly indicated the
HR and 95% CI for PFS, and the remaining two studies did not
include the HR and 95% CI, which we estimated from Kaplan-
Meier curves. The patient characteristics and study quality
levels are listed in Table 1. Three articles have no predictive
data about MGMT expression in patients with NET treated
with alkylating agents [22, 23, 24].
Figure 1. PRISMA flow chart of the selection process toward identifying eligible studies.
MGMT Expression in Patients with NET
The MGMT expression data are shown in Table 2.
Seven studies used the immunohistochemistry method
for MGMT analysis and three applied pyrosequencing
method. In immunohistochemistry subgroup, the MGMT
expression level was evaluated according to the intensity
or positive percentage of the staining. From these seven
studies, three defined MGMT deficiency as complete
absence of staining in all tumor cells [15, 16, 20], two
described MGMT deficiency as a cut-off value of 10% [17, 19], and three defined MGMT status by using unique score
systems. In pyrosequencing method subgroup, a threshold
of 7–8% was used to classify the patients in “methylation”
and “non-methylation” categories [16, 19, 21]. For NETs
of all primary sites, the MGMT methylation rate detected
by methylation-specific PCR and pyrosequencing was
12.7% and 24.8%, respectively. The MGMT deficiency
rates were 27.3% for an immunohistochemistry cutoff
value of 0% and 35.7% (range: 33–43.5%) for an
immunohistochemistry cut-off value of 10%.
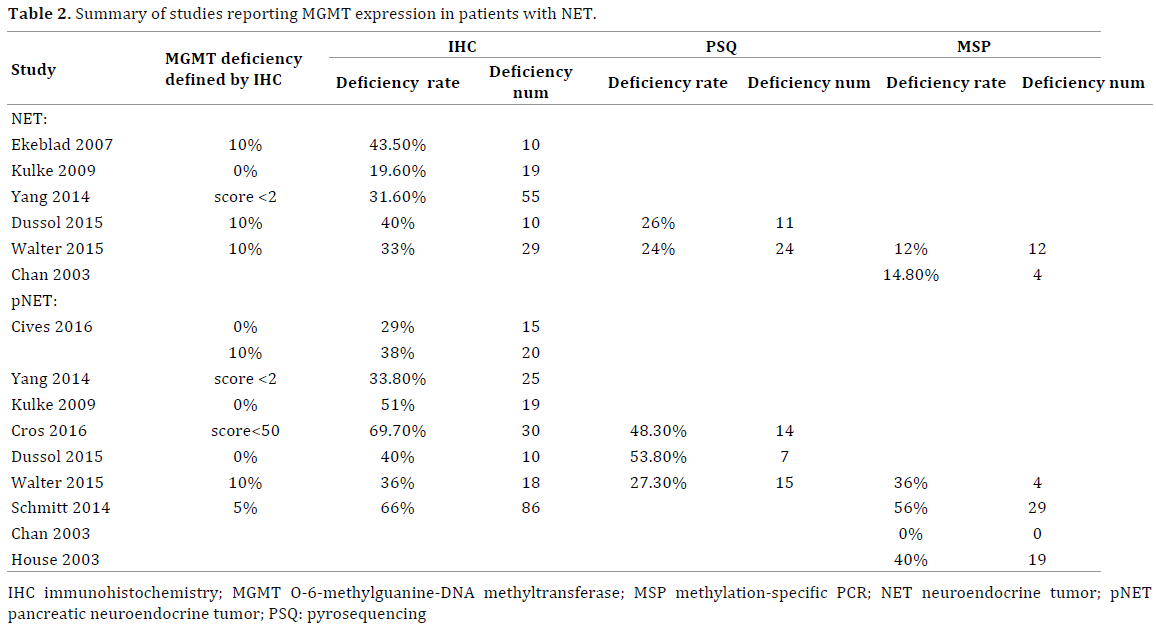
In the pNET subgroup, the MGMT deficiency rates were
35.9% (range: 36–38%) for an immunohistochemistry
cut-off value of 0% and 32.1% (range: 29–51%) for an
immunohistochemistry cut-off value of 10%. Further,
the MGMT promoter methylation rates were 31.7%
(range: 0–56%) by methylation-specific PCR and 37.1%
by pyrosequencing. Although the MGMT deficiency rate
indicated by methylation-specific PCR was lower than that
indicated by pyrosequencing, the MGMT deficiency rates
measured by the three methods of MGMT analysis were
not significantly different (p>0.05).
Four articles included data for the GI-NET subgroup.
Two studies applied the pyrosequencing method and
found MGMT promoter methylation rates of 12.5% and 24%. Three studies applied the immunohistochemistry
method with a cut-off value of 0% and found MGMT
deficiency rates in the range of 0 to 27.7%. The MGMT
deficiency rate measured by the immunohistochemistry
method is significantly lower in the GI-NET subgroup than
in the pNET subgroup (p<0.05).
Relationship between MGMT Promoter Methylation
Status and PFS of Patients with NET Treated with
Alkylating Agent Chemotherapy
The patient survival data are shown in Table 3. A total of
289 patients with NET were treated with alkylating agents
such as temozolomide. The results of the MGMT status
and the PFS of patients with NET are shown in Figure 2.
The meta-analysis based on the immunohistochemistry method indicated that patients with MGMT deficiency had
a significantly longer PFS when treated with alkylating
agent chemotherapy (Figure 2a, average HR = 0.39, 95%
CI 0.17–0.89). Similarly, the meta-analysis for studies that
applied the pyrosequencing method indicated that the PFS
is longer in patients with MGMT promoter methylation
than in patients with MGMT non-methylation (Figure 2b;
average HR = 0.33, 95% CI 0.19–0.56).

Figure 2. Forest plot showed the fixed effect model of the hazard ratio with 95% confidence intervals estimates of O-6-methylguanine-DNA methyltransferase
expression and PFS in patients with neuroendocrine tumor treated with alkylation agents. (a). O-6-methylguanine-DNA methyltransferase detected by
immunohistochemistry method and (b). pyrosequencing method.
Relationship between MGMT Promoter Methylation
Status and Objective Response Rate of Patients with
NET Treated with Alkylating Agent Chemotherapy
Seven articles provided objective response rate
data for the treatment of NET (Supplemental Table
1). The meta-analysis results for the MGMT status and
the objective response rate are shown in Figure 3. For the immunohistochemistry method, the meta-analysis
indicated a significantly lower objective response rate
in patients with intact MGMT compared to patients with
MGMT deficient when treated with alkylating agent
chemotherapy (average OR 7.21, p=0.01). Similarly, for the
pyrosequencing method, the objective response rate was
higher in patients with MGMT methylation than in patients
with intact MGMT.
Figure 3. Forest plot showed the fixed effect model of the risk ratio with 95% confidence intervals estimates of O-6-methylguanine-DNA methyltransferase
expression and objective response rate in patients with neuroendocrine tumor treated with alkylation agents. (a). O-6-methylguanine-DNA methyltransferase
status detected by immunohistochemistry method and (b). pyrosequencing method.
Six articles provided objective response rate data for
the treatment of pNET (Supplemental Table 1). The metaanalysis
results for the MGMT status and the objective
response rate are shown in Figure 4.The meta-analysis
for either the immunohistochemistry or pyrosequencing
methods showed no relationship between MGMT and
objective response rate of patients with pNET treated with
alkylating agent chemotherapy.
Figure 4. Forest plot showed the fixed effect model of the risk ratio with 95% confidence intervals estimates of O-6-methylguanine-DNA methyltransferase
expression and objective response rate in patients with pancreatic neuroendocrine tumor treated with alkylation agents. (a). O-6-methylguanine-DNA
methyltransferase detected by immunohistochemistry method and (b). pyrosequencing method.
Two articles provided objective response rate data
for the treatment of GI-NET; however, the number of
patients was too limited, thus we did not perform a GI-NET
subgroup meta-analysis.
DISCUSSION
This study is the first meta-analysis focused on the
association between MGMT status and the response
of patients with NET to alkylating agent chemotherapy,
particularly temozolomide-based chemotherapy. We
aimed to solve three controversial questions regarding the
treatment of NET: whether MGMT methylation is predictive of NET response to alkylating agent chemotherapy, whether
the MGMT expression rate is different between pNET and GINET,
and whether methodology of MGMT analysis influences
the MGMT expression rate. In this meta-analysis, we showed
that MGMT deficient in temozolomide-treated patients, as
detected by immunohistochemistry and pyrosequencing, is
associated with higher objective response rate and longer
PFS. Further, we determined that the MGMT deficiency rate
is higher in patients with pNET than in patients with GINET.
We also found that the detection of MGMT status by
immunohistochemistry, pyrosequencing, or methylationspecific
PCR produces consistent results.
The predictive value of MGMT for NET remains
controversial; a reason for this is the primary tumor
location. Because NETs are clinically and biologically
heterogeneous, it is increasingly clear that pNET are
biologically distinct from GI-NET and carcinoid tumors
[25, 26]. Compared to other NET, pNET shows higher
objective response rate to cytotoxic chemotherapy [27, 28]. Walter et al. [19] found no difference in MGMT
deficiency rate between GI-NET and pNET. MGMT
promoter methylation is rarely detected in ileal NET but
are found in other digestive segments in up to 25% of all
patients [29]. Kulke et al. [15] found that MGMT deficiency,
as measured by immunohistochemistry, is more common
in pNET than in carcinoid tumors. In our meta-analysis,
we found that the MGMT deficiency rate, detected by both
immunohistochemistry and pyrosequencing, is higher
in pNET than in GI-NET. However, the small number of
patients with GI-NET may have influenced this result.
Thus, more studies on GI-NET are needed to indicate
with certainty whether MGMT deficiency has a predicting
role in the clinical outcome of patients with GI-NET and
patients with pNET after treatment with temozolomide
-based therapy.
The different techniques used to assess MGMT status
also contribute to the controversy behind the predictive
value of MGMT for NET. MGMT deficiency can be assessed by
three methods: immunohistochemistry to analyze MGMT
expression, or methylation-specific PCR or pyrosequencing
to analyze MGMT promoter methylation [30]. Although
immunohistochemistry is the most convenient technique,
it lacks standardization and reproducibility; thus,
methylation-specific PCR and pyrosequencing have been
explored as alternatives to assess MGMT status. Although
MGMT promoter methylation is difficult or impossible
to assess in fine-needle aspiration (FNA) biopsies
when the tumor cell count is too low, pyrosequencing
is more sensitive than methylation-specific PCR for
the detection of MGMT promoter methylation in flash frozen paraffin-embedded tissue samples [31]. Small and
heterogeneous cohorts applied different methods with
various standards [17]. Retrospective studies of MGMT
promoter methylation by pyrosequencing in patients with
glioblastoma have consistently shown that patients with
MGMT promoter methylation benefit from temozolomide
treatment [9]. Until recently, there had been a paucity
of information regarding NET analyzed by methylationspecific
PCR and pyrosequencing for MGMT promoter
methylation and by immunohistochemistry for MGMT
expression. Both PFS and OS were prolonged in patients
with MGMT deficiency/methylation after the first therapy
with alkylating agents (temozolomide, dacarbazine, and
streptozocin). Our study showed that the MGMT deficiency
rate determined by immunohistochemistry and the MGMT
promoter methylation rate determined by pyrosequencing
are similar, and both methods of MGMT analysis can
efficiently predict treatment response to alkylating agent
chemotherapy in patients with NET. Walter et al. [19]
compared immunohistochemistry, methylation-specific
PCR, and pyrosequencing for the detection of MGMT
status in patients with NET and found no difference
in MGMT deficiency rates. Cros et al. [21] found that
increased promoter methylation is associated with MGMT
deficiency; Our finding provides important information on
the role of immunohistochemistry, methylation-specific
PCR and pyrosequencing in MGMT analysis, highlighting
the need for prospective, randomized studies to address
these associations.
Grading may influence our results. Researchers
nowadays agree that treatment options and prognosis of
NET are greatly influenced by pathologic differentiation
[28]. Welin et al. [13] reported that temozolomide-based
chemotherapy could induce partial response in highly
proliferative, poorly differentiated carcinomas. Civeset
al. [20] showed no correlation between tumor grade,
mitotic rate or Ki-67 labeling index, and tumor response
to capecitabine and temozolomide (CAPTEM). This finding suggests that the efficiency of alkylating agent chemotherapy
against NET may relate with Ki-67 scoring. However, due to
the limited information and number of patients available, we
were unable to divide data by grade subgroups.
Studies found three main DNA repair mechanisms are
involved in temozolomide resistance: MGMT repair, DNA
mismatch repair, and the poly(ADP)-ribose polymerase
(PARP) pathway [32]. The primary mechanism of
resistance to temozolomide is directly related to high
MGMT expression, whereas the secondary mechanism
is related to the DNA mismatch repair system in MGMTlacking
cells [33]. The third mechanism depends on the
PARP pathway, which may partly explain why not all
patients with MGMT deficiency respond to temozolomidebased
chemotherapy. Zhang et al. [34] showed that
temozolomide-induced DNA damage and tumor cell
death require a functional DNA mismatch repair system
in addition to low MGMT expression. Moreover, Cros et
al. [21] showed in their study that none of the low MGMT
expression patients with non-response to temozolomide
had a microsatellite instability phenotype. Further studies
are needed to elucidate the relationship between MGMT
status and other predictive biomarkers (e.g. microsatellite
instability) for NET treatments.
To conclude, our results showed that patients with
NET with MGMT deficiency/promoter methylation are
more likely to have a promising response to alkylating
agent chemotherapy, immunohistochemistry method
or pyrosequencing method did not influence the result.
However, the predictive role of MGMT is not significant
in pancreatic patients with NET. We expect that further
studies will apply the predictive value of MGMT to plan
clinical treatments.
Funding
This work was supported by grants from the National
Natural Science Foundation of China (81472670, 81172005,
81402397, 81402398, and 81172276), the National
Natural Science Foundation of Shanghai (14ZR1407600),
the“Yang-Fan”Plan for Young Scientists of Shanghai
(14YF1401100), and the PhD Programs Foundation
of Ministry of Education of China (20110071120096).
The funding agencies had no role in study design, data
collection and analyses, decision to publish, or preparation
of the manuscript.
Author Contributions
GHL and LL contributed to the literature searching,
WWQ and WCT reviewed the searching results. GHL and
ZSR wrote the manuscript. GHL, LL, and XHX performed
the statistical analyses. YXJ and NQX participated in study
design and coordination and helped to draft the manuscript.
All authors read and approved the final manuscript.
Acknowledgement
Heli Gao and Liang Liu contributed equally to this work.
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- Fraenkel M, Kim MK, Faggiano A, Valk GD. Epidemiology of
gastroenteropancreatic neuroendocrine tumours. Best Pract Res Clin
Gastroenterol 2012; 26:691-703. [PMID: 23582913]
- Linjie G. Current status of clinical research on gastroenteropancreatic
neuroendocrine tumors in China. China J Gastroenterol 2012; 17:276-8.
- de Mestier L, Dromain C, d'Assignies G, Scoazec JY, Lassau N, Lebtahi
R, et al. Evaluating digestive neuroendocrine tumor progression and
therapeutic responses in the era of targeted therapies: state of the art.
Endocr Relat Cancer 2014; 21:R105-20. [PMID: 24351682]
- Strosberg J, Goldman J, Costa F, Pavel M. The role of chemotherapy
in well-differentiated gastroenteropancreatic neuroendocrine tumors.
Front Horm Res 2015; 44:239-47. [PMID: 26303716]
- Natarajan AT, Vermeulen S, Darroudi F, Valentine MB, Brent TP, Mitra
S, et al. Chromosomal localization of human O6-methylguanine-DNA
methyltransferase (MGMT) gene by in situ hybridization. Mutagenesis
1992; 7:83-5. [PMID: 1635460]
- Kaina B, Christmann M, Naumann S, Roos WP. MGMT: key node in
the battle against genotoxicity, carcinogenicity and apoptosis induced by
alkylating agents. DNA repai 2007; 6:1079-99. [PMID: 17485253]
- Bugni JM, Meira LB, Samson LD. Alkylation-induced colon
tumorigenesis in mice deficient in the Mgmt and Msh6 proteins. Oncogene
2009; 28:734-41. [PMID: 19029948]
- Gerson SL. MGMT: its role in cancer aetiology and cancer therapeutics.
Nat Rev Cancer 2004; 4:296-307. [PMID: 15057289 ]
- Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et
al. MGMT gene silencing and benefit from temozolomide in glioblastoma.
N Engl J Med 2005; 352:997-1003. [PMID: 15758010]
- Weller M, Tabatabai G, Kastner B, Felsberg J, Steinbach JP, Wick A,
et al. MGMT Promoter methylation is a strong prognostic biomarker for
benefit from dose-intensified temozolomide rechallenge in progressive
glioblastoma: The DIRECTOR Trial. Clin Cancer Res 2015; 21:2057-64.
[PMID: 25655102]
- Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et
al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of
nonrandomised studies in metaanalyses. Available: https://www.ohri.ca/
programs/clinicalepidemiology/oxford.asp.
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical
methods for incorporating summary time-to-event data into metaanalysis.
Trials 2007; 8:16. [PMID: 17555582]
- Welin S, Sorbye H, Sebjornsen S, Knappskog S, Busch C, Oberg
K. Clinical effect of temozolomide-based chemotherapy in poorly
differentiated endocrine carcinoma after progression on first-line
chemotherapy. Cancer 2011; 117:4617-22. [PMID: 21456005]
- Gilbert JA, Adhikari LJ, Lloyd RV, Halfdanarson TR, Muders MH, Ames
MM. Molecular markers for novel therapeutic strategies in pancreatic
endocrine tumors. Pancreas 2013; 42:411-21. [PMID: 23211371]
- Kulke MH, Hornick JL, Frauenhoffer C, Hooshmand S, Ryan DP, Enzinger
PC, et al. O6-methylguanine DNA methyltransferase deficiency and response
to temozolomide-based therapy in patients with neuroendocrine tumors.
Clin Cancer Res 2009; 15:338-45. [PMID: 19118063]
- Dussol AS, Joly MO, Vercherat C, Forestier J, Hervieu V, Scoazec JY, et
al. Gemcitabine and oxaliplatin or alkylating agents for neuroendocrine
tumors: Comparison of efficacy and search for predictive factors guiding
treatment choice. Cancer 2015; 121:3428-34. [PMID: 26058464]
- Ekeblad S, Sundin A, Janson ET, Welin S, Granberg D, Kindmark H, et
al. Temozolomide as monotherapy is effective in treatment of advanced
malignant neuroendocrine tumors. Clin Cancer Res 2007; 13:2986-91.
[PMID: 17505000]
- Schmitt AM, Pavel M, Rudolph T, Dawson H, Blank A, Komminoth P,
et al. Prognostic and predictive roles of MGMT protein expression and
promoter methylation in sporadic pancreatic neuroendocrine neoplasms.
Neuroendocrinology 2014; 100:35-44. [PMID: 25012122]
- Walter T, van Brakel B, Vercherat C, Hervieu V, Forestier J, Chayvialle JA,
et al. O6-Methylguanine-DNA methyltransferase status in neuroendocrine
tumours: prognostic relevance and association with response to alkylating
agents. Br J Cancer 2015; 112:523-31. [PMID: 25584486]
- Cives M, Ghayouri M, Morse B, Brelsford M, Black M, Rizzo A, et al.
Analysis of potential response predictors to capecitabine/temozolomide
in metastatic pancreatic neuroendocrine tumors. Endocr Relat Cancer
2016; 23:759-67. [PMID: 27552969]
- Cros J, Hentic O, Rebours V, Zappa M, Gille N, Theou-Anton N, et al.
MGMT expression predicts response to temozolomide in pancreatic
neuroendocrine tumors. Endocr Relat Cancer 2016; 23:625-33. [PMID:
27353036]
- Chan AO, Kim SG, Bedeir A, Issa JP, Hamilton SR, Rashid A. CpG island
methylation in carcinoid and pancreatic endocrine tumors. Oncogene
2003; 22:924-34. [PMID: 12584572]
- House MG, Herman JG, Guo MZ, Hooker CM, Schulick RD, Lillemoe
KD, et al. Aberrant hypermethylation of tumor suppressor genes in
pancreatic endocrine neoplasms. Ann Surg 2003; 238:423-31; discussion
31-2. [PMID: 14501508]
- Yang QC, Wang YH, Lin Y, Xue L, Chen YJ, Chen MH, et al. Expression
of O(6)-methylguanine DNA methyltransferase (MGMT) and its clinical
significance in gastroenteropancreatic neuroendocrine neoplasm. Int J
Clin Exp Pathol 2014; 7:4204-12. [PMID: 25120800]
- Basu B, Sirohi B, Corrie P. Systemic therapy for neuroendocrine
tumours of gastroenteropancreatic origin. Endocr Relat Cancer 2010;
17:R75-90. [PMID: 20008097]
- Kloppel G. Classification and pathology of gastroenteropancreatic
neuroendocrine neoplasms. Endocr Relat Cancer 2011; 18 Suppl 1:S1-16.
[PMID: 22005112]
- Kouvaraki MA, Ajani JA, Hoff P, Wolff R, Evans DB, Lozano R, et al.
Fluorouracil, doxorubicin, and streptozocin in the treatment of patients
with locally advanced and metastatic pancreatic endocrine carcinomas. J
Clin Oncol 2004; 22:4762-71. [PMID: 15570077]
- Turner NC, Strauss SJ, Sarker D, Gillmore R, Kirkwood A, Hackshaw
A, et al. Chemotherapy with 5-fluorouracil, cisplatin and streptozocin
for neuroendocrine tumours. Br J Cancer 2010; 102:1106-12. [PMID:
20234360]
- Liu L, Broaddus RR, Yao JC, Xie S, White JA, Wu TT, et al. Epigenetic
alterations in neuroendocrine tumors: methylation of RAS-association
domain family 1, isoform A and p16 genes are associated with metastasis.
Mod Pathol 2005; 18:1632-40. [PMID: 16258509]
- Preusser M, Charles Janzer R, Felsberg J, Reifenberger G, Hamou
MF, Diserens AC, et al. Anti-O6-methylguanine-methyltransferase
(MGMT) immunohistochemistry in glioblastoma multiforme: observer
variability and lack of association with patient survival impede its
use as clinical biomarker. Brain Pathol 2008; 18:520-32. [PMID:
18400046]
- Wick W, Weller M, van den Bent M, Sanson M, Weiler M, von Deimling
A, et al. MGMT testing--the challenges for biomarker-based glioma
treatment. Nat Rev Neurol 2014; 10:372-85. [PMID: 24912512]
- Boulton S, Pemberton LC, Porteous JK, Curtin NJ, Griffin RJ, Golding BT,
et al. Potentiation of temozolomide-induced cytotoxicity: a comparative
study of the biological effects of poly(ADP-ribose) polymerase inhibitors.
Br J Cancer 1995; 72:849-56. [PMID: 7547230]
- Koumarianou A, Kaltsas G, Kulke MH, Oberg K, Strosberg JR,
Spada F, et al. Temozolomide in advanced neuroendocrine neoplasms:
pharmacological and clinical aspects. Neuroendocrinology 2015;
101:274-88. [PMID: 25924937]
- Zhang J, Stevens MF, Hummersone M, Madhusudan S, Laughton CA,
Bradshaw TD. Certain imidazotetrazines escape O6-methylguanine-DNA
methyltransferase and mismatch repair. Oncology 2011; 80:195-207.
[PMID: 21720182]





