What is known on this subject
• In daily nursing work, conflict is inevitable.
• The conflict management styles used by nurse managers have an important effect on their performance.
• Effective conflict management promotes motivation, enhances morale and promotes individual and organisational growth.
What this paper adds
• Courses in conflict management should be available for all nurses, and especially for the nurse manager.
• Prior training that focuses on cultural factors must be given to non-national nurse managers before they arrive in Arab countries.
• Research is needed to establish the cultural meanings of the five conflict management styles.
Key words
Arab countries, conflict management, Ibadhiyah, nurse managers, Oman
Introduction
Nurse managers work in environments in which conflict is likely to arise due to both the nature of their work and the need to interact with a wide range of individuals. Although the management of conflict has been studied previously, no research has examined the conflict management styles of nurse managers in Oman or any other Arab country. The present study sought to address this issue by examining the conflict management styles used by nurse managers in the Sultanate of Oman, with the aim of increasing understanding of the behaviour of nurse managers from different backgrounds, and their ability to deal with conflict.
Background to Oman
The Sultanate of Oman is located in the south-eastern corner of the Arabian Peninsula. The total Sultanate population is 2 508 837, and the country’s coastline extends for 1700 kilometres, from the Strait of Hormuz in the North to the borders of the Republic of Yemen. Agriculture and fishing are the traditional occupations in Oman, and 40% of the labour force is involved in agriculture or trade. Oil is considered to be the primary source of income in Oman (Ministry of National Economy, 2004).
The results of the 2003 census (Ministry of National Economy, 2004) showed that the male:female ratio is 128:100 in the population as a whole, and 102:100 among Omani nationals. In ethnic terms, the population is predominantly Arab, with significant minorities of Indians, Pakistanis and East Africans, mostly living in the principal ports. In terms of religion, the majority (around 55%) of the population is Ibadhi Muslim, and Sunni Muslims form the other major religious group. Arabic is the official language, but English is widely used as a second language.
Ibadism, a distinct sect of Islam that is neither Sunni nor Shi’i, exists mainly in Oman, East Africa, the Mzab valley of Algeria, the Nafus mountains of Libya, and the island of Jerba in Tunisia. Ibadi communities are generally regarded as conservative. Sunni Muslims traditionally regard the Ibadiyya as a khariijite group, but Ibadis reject this designation. Ibadis regard other Muslims not as kafir (unbelievers), but as kuffar annima (those who deny God’s grace). Ibadi beliefs differ in several respects from those of Sunni Muslims, chief among them being that:
• Muslims will not see God on the day of Judgement
• whosoever enters the Hellfire, will live therein forever
• the Qur’an was created by God at a certain point of time.
Subdivisions of the Ibadhiyah include the following sects: Al-Wahbiyah, Al-Nukkar, Khalafiyah, Al- Naffathiyah, Al-Husainiyah, Al-Sakakiyah, Umairiyah and Al-Farthiyah (Ennami, 1996).
The rapid growth of healthcare services has led to an increasing demand on the medical and nursing workforce. During the last three decades, the number of nurses working inOmanas a proportion of the general population has increased dramatically from 5.6 per 10 000 in 1975 to 31.5 per 10 000 in 2005 (Ministry of Health, 2006). The nursing profession is the fastest growing health profession in the country. In 1975 there were just 450 nurses working for the Ministry of Health (MOH), but this figure rose to 7909 in 2005, and 59% of these nurses were Omani (Ministry of Health, 2006). In total, 743 nurses were male and the remainder were female. TheMinistry ofHealth employs 2981 doctors, of whom 29% are Omani and 64% are male.
Literature on conflict management
Conflict is a natural and pervasive phenomenon in human experience (Pondy, 1967;De Dreu and Van De Vliert, 1997; Jameson, 1999; Tengilimoglu and Kisa, 2005). It is a part of people’s lives in organisations as well as being a part of domestic life. Indeed, it is inevitable, especially in a highly stressful environment (Shockley-Zalabak, 1981; Forte, 1997; Jameson, 1999; Hurst and Keenan, 2000, Tengilimoglu and Kisa, 2005). The management of conflict is extremely important both for the effective functioning of organisations and for the personal, cultural and social development of individuals. The term conflict management strategy is used to describe any action that is taken by a disputant or a third party tomanage or resolve a conflict (Jameson, 1999). Effective conflict management is a vital skill that can be learned (Bartol et al, 2001).
Blake and Mouton (1964) were the first to formalise a framework for managing organisational conflict. They developed a managerial grid composed of five basic styles of management that characterise an individual’s likely behaviour in a conflict situation (see Box 1). The grid model consists of two measurable dimensions which have the greatest effect on the way that people work, namely concern for production and concern for people. Production is ‘whatever an organisation hires people to accomplish’ (Blake and Mouton, 1985, p. 10). Conflict management is also a function of high or low levels of concern for self, combined with high or low levels of concern for others (De Dreu et al, 2001)
The five ways of handling conflict can be defined as avoiding, compromising, integrating, obliging and dominating (Blake andMouton, 1964; Thomas and Kilmann, 1974; Rahim, 1983; De Dreu et al, 2001).
Avoiding conflict results from low levels of concern for the self and others. It involves reducing the importance of the issues, and attempting to suppress thoughts about them (Keenan et al, 1998). In avoiding conflict the individual simply refuses to address it, and is unassertive and uncooperative. Conflict avoidance is particularly appropriate when the other party is more powerful (McElhaney, 1996; De Dreu et al, 2001; Tabak and Koprak, 2007).
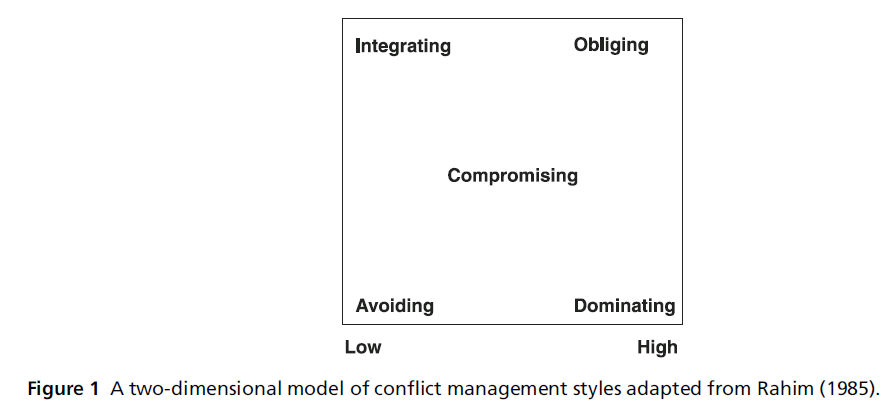
Figure 1 :A two-dimensional model of conflict management styles adapted from Rahim (1985).
Compromising when faced with conflict results from moderate concern both for oneself and for others. It involves intermediate levels of both assertiveness and cooperation. This approach focuses on quick, mutually agreeable decisions that partially satisfy both parties (Rahim, 1983). Compromising emerges when there is negotiation and exchange. Each person gains something but also gives up something else in the process.
Integrating or collaborative approaches to dealing with conflict involve one party working with the other to find a solution that satisfies both parties. Integrating confronts issues and arises from high levels of concern for the self and others. It is both assertive and cooperative, and involves an attempt to work with the other person to find a solution that fully satisfies the concerns of both parties. This approach leads to mutually satisfying decision making (Marriner, 1982; Vivar, 2006).
Obliging or accommodating approaches to managing conflict result from low levels of concern for oneself and high levels of concern for others. These approaches are orientated towards accepting and incorporating the other party’s will, and thus involve unilateral concessions, unconditional promises and offers of help. Accommodating is characterised by cooperative but unassertive behaviour. The accommodating individual exhibits self-sacrificial behaviour by neglecting his or her own concerns in order to satisfy those of the other person (Marriner, 1982; McElhaney, 1996; Valentine, 2001; Tabak and Koprak, 2007).
Dominating or forceful approaches to managing conflict focus on imposing one’s will on others through threats and bluffs, persuasive arguments and power. Dominating is an aggressive, uncompromising approach to conflict. It is power-driven, and the individual pursues his or her own personal goals without regard for others (McElhaney, 1996; Valentine, 2001; Vivar, 2006).
Conflict management in nursing
Conflict in nursing is frequently described in terms of the relationship between two occupational groups, such as physicians and nurses, staff nurses and nurse managers, or two different departments (Hendel et al, 2005; Vivar, 2006; Tabak and Koprak, 2007). Managing such conflict makes a crucial contribution to the effective functioning of nursing organisations, and consequently to the excellence of nursing care (Vivar, 2006). An individual’s cultural and family traditions, personality and life experience all shape the ways in which he or she handles conflict (Campbell, 2003). There has been no research examining how nurses in Oman manage conflict, which styles of conflict management they use and why.
Aims of the study
The study reported here is part of a much larger project with the following aims:
• to explore and compare the conflict management styles used by nurse managers in the Sultanate of Oman
• to identify the roles of culture, gender, and other variables related to nurse managers working in the Sultanate of Oman, in conflict management
• to add to existing knowledge in this area of work.
This paper presents a report of a survey of conflict management styles used by nurse managers in Oman.
Study design
A survey methodology was developed based on an adapted version of the Rahim Organisational Conflict Inventory II (ROCI-II) (Rahim, 1983). This tool was developed from a sample of 1219 American managers from different management levels and sectors. Of these, 185 were hospital management personnel (Rahim, 1983). ROCI-II is valid and reliable. It is used internationally, including in Middle Eastern countries (Kramer, 1989; Elsayed-Ekhouly and Buda, 1996; Kozan and Ergin, 1999; Kozan, 2002; Boonsathorn, 2003). The tool consists of 28 items, presented using a 5-point Likert scale (where 5 = strongly agree and 1 = strongly disagree), that reflect conflict management styles based on individual disposition. These items cover the five styles as follows: items 2, 4, 5, 12, 22, 23 and 28 cover integrating styles; items 1, 10, 13, 17, 19 and 24 cover obliging styles; items 6, 9, 18, 21 and 25 cover dominating styles; items 7, 8, 11, 16, 26, and 27 cover avoiding styles; items 3, 14, 15 and 20 cover compromising styles. The five conflict management styles reflect different combinations of concern for self and concern for others (Rahim, 1983). The tool was adapted in that some words in the tool were changed so as to be more appropriate to an Arab culture, and some complex terms were altered to facilitate ease of understanding.
Data collection and analysis
The study was introduced to the head of the nursing department in each participating hospital. The head of nursing distributed the survey to their nurse managers and the researcher collected the completed questionnaires from the nursing office at an agreed later date.
A data analysis plan was developed to guide the analysis of the study. This was derived from the research questions, the research design, the method of data collection and the level of measurement of the data. The data were coded to ensure anonymity and confidentiality. Before selecting suitable tests, data from the demographic questions were consolidated and coded at the nominal level to facilitate analysis. The statistical package SPSS was used to aid data analysis. Mean values, standard deviations and percentages were derived for the overall sample, and were categorised by age, gender, nationality, nursing qualifications, and number of years of experience as registered nurses and as nurse managers. Number of years of experience in this post, and level of nursing management were also analysed. Non-parametric tests were employed to determine the relationship between the following variables: age, nationality, marital status and qualifications. The one-sample Kolmogorov–Smirnov test was applied in order to ascertain whether the data were normally distributed. The same testwas also used to explore the conflictmanagement styles used by nurse managers. A non-parametric Spearman’s rho test was used to determine whether there was any relationship between age and number of years of experience with regard to conflict management style. The Mann- Whitney U-test was used to compare male and female managers with regard to conflict management styles. The Kruskal–Wallis test was used to test the remaining variables, because there were three or more ordinal independent variables.
Sample
The population for the survey consisted of the 321 nurse managers in the nine Ministry of Health referral hospitals. No exclusion criteria were set, so all nurse managers from different levels and different hospitals were included (see Table 1).
Ethics
The Research Ethics Committees at De Montfort University, UK and the Ministry of Health, Sultanate of Oman reviewed and approved the study.
Each of the 321 potential participants received a package containing the following:
• a letter introducing the researcher and the project
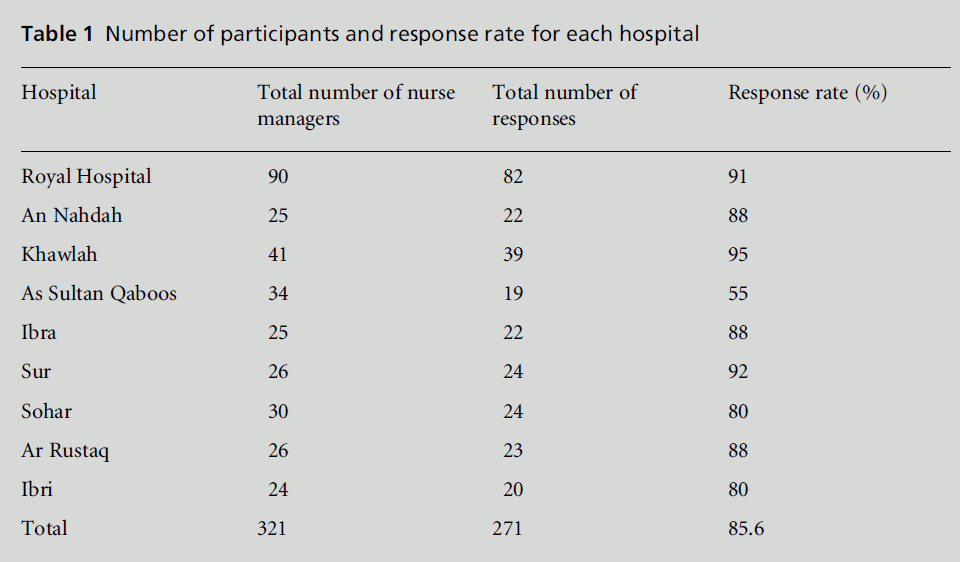
Table 1: Number of participants and response rate for each hospital.
• information for participants
• a consent form
• the research tool plus additional, mainly closed questions about national origin, age, gender, job position, qualifications, and number of years of experience.
Those who elected to take part were asked to sign the consent form, complete the questionnaire, and return both by a specified date. Participation in the study was voluntary, and confidentiality and anonymity were assured. Participants were advised of their right to withdraw from the study at any time. To ensure anonymity, the consent form and questionnaires were returned in separate envelopes.
Findings
Sample characteristics
A total of 271 responses were received. Managers in all of the hospitals responded. The highest response rate was from Sur (92%) and the lowest was from Sultan Qaboos (55%) (see Table 1). Analysis showed that 80.8% of respondents were female, 79% were married and 15.5% were single. A few were either widowed or divorced. In total, 68.3% of respondents held firstlevel management positions and a further 28.8%were employed at middle management levels (see Table 2).
Conflict management styles
Respondents reported using the integrating style as theirfirst choicewhenmanaging conflict.The preference rating for integrating was 4.31%, followed by compromising (3.46%), obliging (3.14%), dominating (2.93%) and avoiding (2.78%) (see Table 3). There was a positive but non-significant relationship between age and integrating style. Similarly, the relationship between age and the avoiding and compromising styles was negative but non-significant. However, there was a significant relationship between age and the dominating and obliging styles (P < 0.01 and P = 0.001, respectively).
There was a positive relationship between the number of years of experience as a registered nurse and the integrating style of conflict management. In contrast, there was a negative relationship between the number of years of experience as a registered nurse and the other four styles of conflict management. Table 4 shows that the relationship between number of years of experience and styles of conflict management is significant, with obliging style (P<0.001) and dominating style (P = 0.001) being associated with older age.
Table 4 demonstrates that number of years of experience as a nurse manager has the same relationship with conflict management styles. It is positively associated with the integrating style and negatively associated with the other four styles. The relationship between number of years of experience as a nurse manager and the dominating style was significant (P= 0.035), but this was not significant when using the revised alpha level, and the relationship with the obliging style was even stronger (P = 0.005).
There was no relationship between number of years of experience in the current post and integrating style, while the relationship between this factor and compromising style was positive but non-significant. Similarly, there were negative but non-significant relationships with avoiding, dominating and obliging styles.
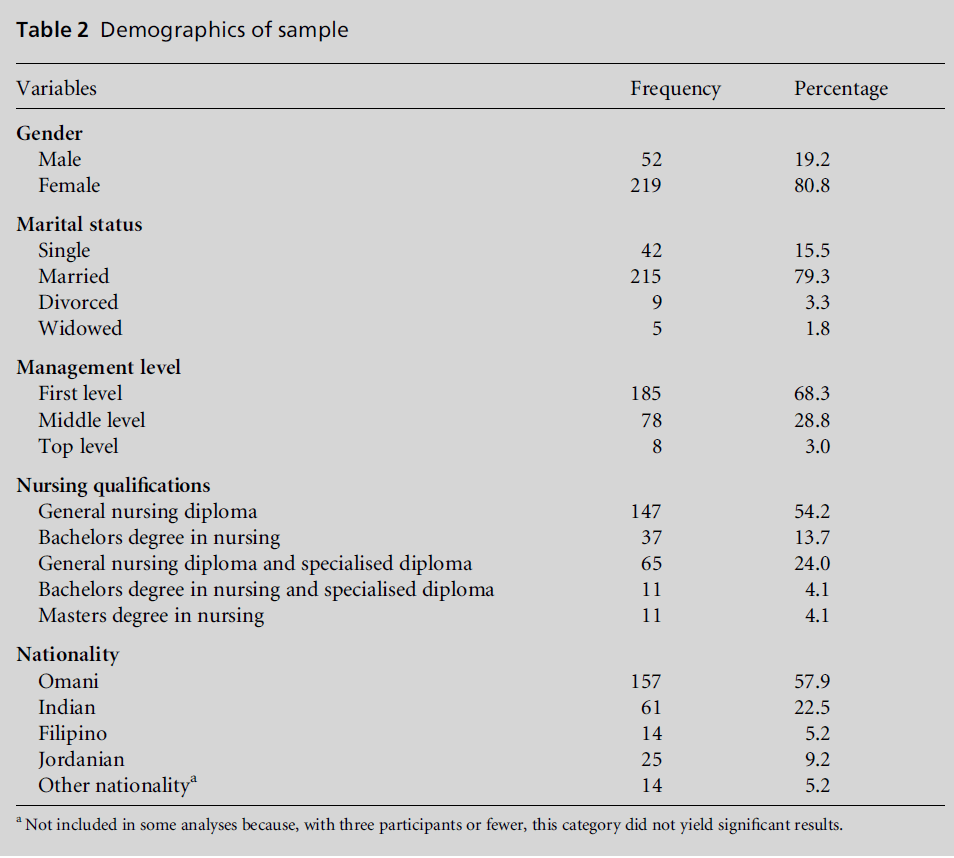
Table 2:Demographics of sample.
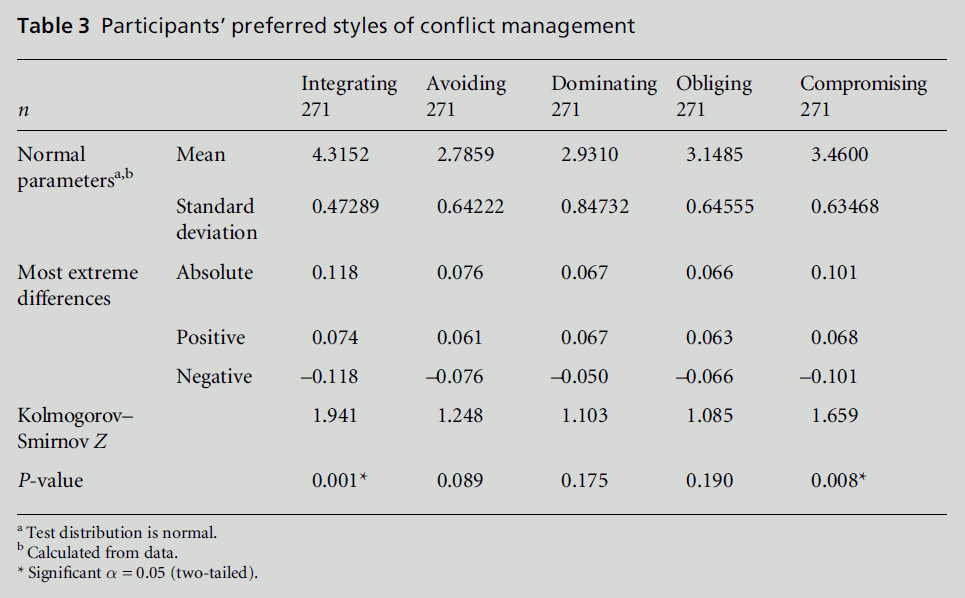
Table 3:Participantsâ€Âââ€Å¾Â¢ preferred styles of conflict management.
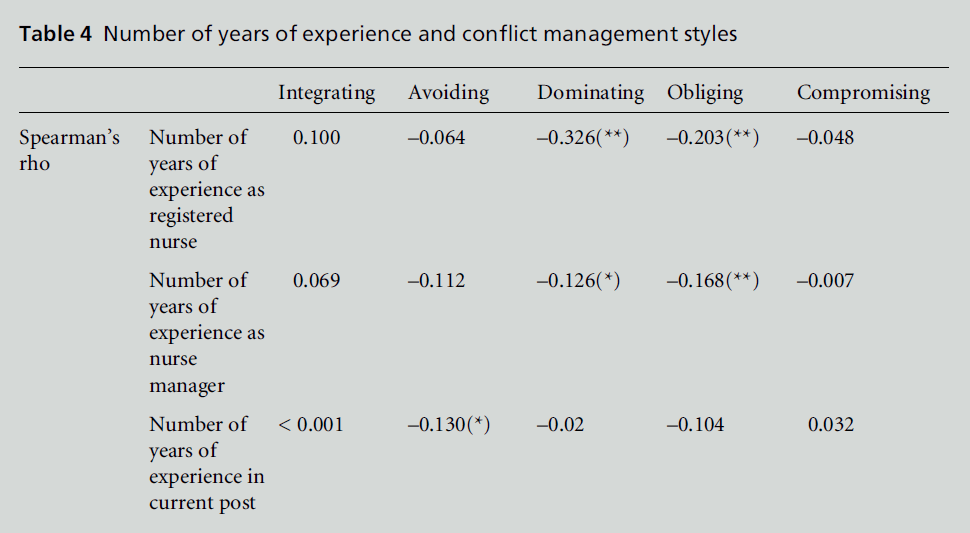
Table 4:Number of years of experience and conflict management styles.
Conflict management styles and gender
The Mann–Whitney U-test was used to determine possible differences between male and female nurse managers with regard to conflict management styles. Nurse managers did appear to show different preferences according to gender. Male nursemanagers favoured compromising, dominating, obliging, integrating and avoiding styles, in that order. Female nurse managers, on the other hand, preferred avoiding, integrating, obliging, dominating and compromising styles, in that order. Thus the preferred styles for the two genders are the direct opposite of each other. There was no significant difference between the genders with regard to the mean score for each style, except for compromising style.
Conflict management styles and nationality of the participants
The conflict management styles of nurse managers appeared to differ according to their nationality. Omani managers preferred dominating, obliging, integrating, compromising and avoiding styles, in that order. Jordanian managers preferred compromising, dominating, integrating, obliging and avoiding styles, in that order. Indian managers preferred avoiding, obliging, integrating, compromising and dominating styles, in that order. Filipino managers preferred integrating, avoiding, compromising, obliging and dominating styles, in that order.
Conflict management styles and nursing qualifications
The Kruskal–Wallis test was used to determine the relationship between conflict management styles and nursing qualifications. The results (see Table 5) indicated thatmanagers withMasters and Bachelors degrees in nursing with specialised diplomas preferred the compromising style. Diploma holders preferred the dominating style. Managers with a Bachelors degree in nursing preferred the integrating style.
Conflict management styles and nursing management level
There was a significant difference in preferred conflict management style between nurse managers according to their management level. The obliging style was the first choice among first-level (basic grade) nurse managers and the last choice among top-level managers, whereas the integrating style was the first choice among top-level managers and the last choice among first-level nurse managers. Middle-level managers preferred the integrating style, and the obliging style was their last choice.
Conflict management styles and marital status
There was a significant difference in the use of the obliging style by managers according to their marital status (P = 0.041). This is not significant according to the revised alpha level. Widows and divorcees preferred the integrating style, and only used the obliging style when absolutely necessary. Single and married participants did not show specific style preferences, although marital status had a significant effect on obliging style (P = 0.041).
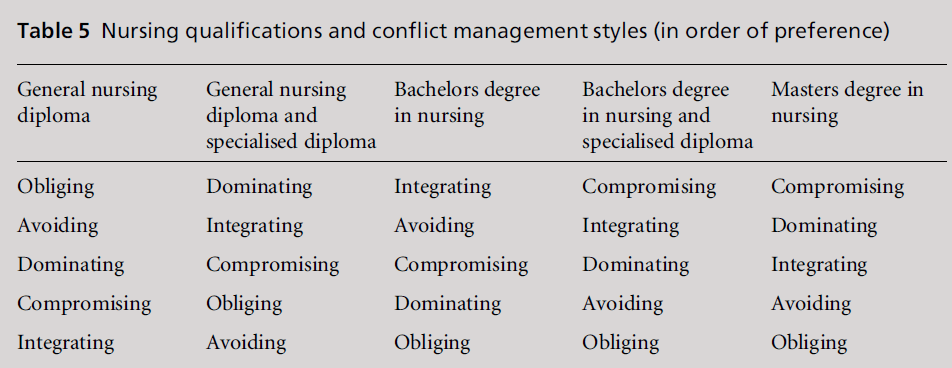
Table 5:Nursing qualifications and conflict management styles (in order of preference).
Discussion
Culture and conflict management styles
Four nationalities – Omani, Jordanian, Indian and Filipino – were included in the analysis, because the other nationalities were not well represented in the sample. The preferences with regard to conflict management style were different for each nationality. In his study of cultural consequences, Hofstede (2001) combined all of the Arab countries and dealt with them as one country with the same culture. Oman and Jordan are Arab countries that share the same culture, language and religion, and the culture in eachof the two countries is regarded as a subculture of the main Arab culture. The research reported here shows that nurse managers from each of the two nationalities had different preferences for conflict management style, although it is acknowledged that Jordanians in Oman were not in their own country. The findings of this study make a reasonable case for the effect of subcultures on conflict management style. Subculture, as defined by values, was as strong a predictor of conflict management style as organisational size and respondent age and gender. These findings extend Hofstede’s (2001) argument that national culture influences organisational behaviour. Like differences in national cultures, differences among subcultures of the same country significantly influence conflict behaviour in organisations.
This research is not supported by previous studies conducted in Oman and Jordan (Al Bawab, 1986; Qatan, 2001; Al Belbeisi, 2003; Harem, 2003; Dmour, 2004). Omani nurse managers preferred dominating and obliging styles, whereas Jordanian nurses preferred compromising and dominating styles. This finding is related to many factors. Most Omanis occupy the post of nurse manager without being designated for that post. They therefore tend to dominate their subordinates in order to control the department, and use the obliging style with the administrative staff and their supervisors in order to secure their positions. This pattern reflects the authoritarian tone of administration in Oman, and the role of collectivism in suppressing competition among peers. Moreover, frank conversation is not easy in a society that has high power differentials. Under such conditions, people are always careful about what they say and how they say it. In addition, Kozan and Ergin (1999) maintain that individuals who used the controlling style had stronger power values. Their style could be indicative of a desire to accommodate their peers and supervisors in order to secure positions in the company. In Arab culture, the individual must respect family elders and defend the family. The elders, in return, are expected to settle disputes. Growing up in a strong family-oriented culture is an emotionally rich and satisfying experience. Children receive attention from their parents and other family members and spend much time with them. Individuals are therefore deeply embedded in their ‘in-groups’, and their individual identities are defined in the context of these groups. As a result, there is a cost attached to the support received from the in-group. The individual has to be careful not to disappoint the other members, and to satisfy the other members’ expectations. In the context of nursing, supervisors have to maintain good relationships and secure their post.
The Jordanian nurse managers who were recruited to Oman were on a higher scale grade and received the highest salary of all the nurses. Most, if not all of them had many years of experience and at least a Bachelor’s degree in nursing. The Jordanian nurse managers who were working in Oman focused on improving nursing care, and planned to stay a long time, and therefore used compromising as a preferred style of conflict management. Kozan (1989) found that Jordanian managers were mainly compromising with peers. Valentine (2001) pointed out that the frequent use of the compromising style indicates a primary focus on the practical aspects of care.
Integrating was the third preference for conflict management style used by Omani and Jordanian nurse managers.This finding is not supported by the literature, as all previous studies conducted in both countries found this style to be the participants’ first choice (Al Bawab, 1986; Qatan, 2001; Al Belbeisi, 2003; Harem, 2003; Dmour, 2004). This difference relates mainly to the fact that the previous research was conducted in the field of education, where the participants did not have to deal with emergencies and life and death situations, so had time for negotiation and discussion to reach agreement and solve problems. It seems that the nurse managers in this study used an integrating style if there was a relationship or personal conflict that was not related to work or that was not affecting a patient’s life and quality of nursing care.
Compromising was the fourth preference for conflict management style used by Omani nurse managers, whereas it was the second choice for the participants in a study by Qatan (2001). In both studies, compromising was the next preferred style after integrating. A compromising style is used as a back-up to a dominating style.
Indian and Filipino nurse managers used different conflict management styles to Jordanian and Omani nurse managers. Filipino nurse managers seemed to prefer the integrating style, which was not unexpected given that they had earned a reputation for having a strong work ethic, being persistent and effective team players, always following directions, having excellent clinical skills and rarely complaining (Yu Xu and Davidhizar, 2004). The avoiding style was the first choice and obliging was the second choice for Indian nurse managers, while avoiding was the second choice for the Filipino nurse managers and obliging was their fourth choice. The majority of Indian nurse managers were recruited to Oman as staff nurses, and after many years of experience they were promoted to work as nurse managers. Some of them still had the designation of staff nurse, and therefore they used an obliging style with their managers and an avoiding style with their peers. Indian and Filipino nurse managers were highly concerned for the other. Valentine (2001) referred to the frequent use of the avoiding style, linking this with the sense of powerlessness associated with the nurse manager’s role. Furthermore, a high level of concern for others is most likely to occur when there is an expectation of a long-term dependency on the other party. This finding is supported by the literature. Yu Xu and Davidhizar (2004) state that Asian nurses, including Filipino and Indian nurses, who have a primarily communal mentality tend to use avoiding, obliging and integrating styles of conflict management to maintain interpersonal harmony. Asians are socialised into respecting authority, whether it be heads of households, community leaders, or managers and administrators in the workplace (Valentine, 2001).
Ting-Toomey et al (2000) noted that Latino and Asian Americans tended to use obliging and avoiding styles. Those authors argued that Latino and Asian-American cultures do not perceive these styles as negative, and went on to state that obliging and avoiding styles are not understood identically in all cultures. Asians, unlike individuals from Western cultures, do not view obliging and avoiding styles negatively. Compromising is the fourth choice of conflict management style among Indian nurse managers and the third choice among Filipinos. A dominating style is the last choice of Indian and Filipino nurse managers, as well as for the participants in the studies by Woodtli (1987), Cavanagh (1988, 1991), Barton (1991), Eason (1999) and Kunaviktikul et al (2000). Less use of the dominating style is related to less power. Nurse managers feel that they do not have the power to use this style because most Indian nurse managers do not have the designation of nurse manager. Both Indian and Filipino nurse managers feel that because they are in Oman temporarily, Omani nurses may perhaps take over their roles at any time. Thus culture does play a role in determining a person’s choice of conflict resolution strategy.
Despite the extant literature on strategies of conflict resolution, most of the studies that have investigated the effects of culture and personality have addressed these separately. To date, most of the research examining the impact of culture on conflict resolution styles has been done using the standard cultural variables of individualism–collectivism, power distance, masculinity– femininity, and short-term–long-term orientation as outlined by Hofstede (1983). However, in this research, all four nationalities are regarded as collectivist, and the conflict management styles are measured using tools developed in Western culture. There is no evidence regarding understanding of the same terms and no research into whether or not each nationality uses the same style in their own country. More studies need to be carried out to determine whether the same conflict management styles are used by nurse managers in their own countries, and to determine whether they use the same styles in other countries.
Gender and conflict management
The study findings show that gender may influence a nurse manager’s choice of conflict management style. To date, findings relating to gender and preferences for conflict management behaviour have been inconsistent. Some studies have produced evidence supporting such gender stereotypes, as women rely more on harmony-enhancing choices of style, selecting the avoiding style as their first choice (Cavanagh, 1988; Cavanagh, 1991; Eason, 1999; Valentine, 2001). However, there is other evidence that shows no significant differences with regard to gender and preferences for particular conflict management styles (e.g. Ting-Toomey et al, 2000). Woodtli (1987) and Hendel et al (2005) found that female nursing managers used compromising as their first choice of style. Other researchers have found that women use a cooperative style more often than their male counterparts (Levine and Feldman, 1997); research conducted in Arab countries has also yielded different findings. Qatan (2001) found that Omani men used avoidance more than women, but this was the only difference. Al-Bawab (1986) also found that female Jordanian principals were more compromising and less obliging than their male counterparts, while gender had no effect in the other studies (Al-Belbeisi, 2003; Harem, 2003; Dmour, 2004). In the present study, female nurse managers used avoiding as their preferred conflict management style, as did the participants in the studies by Cavanagh (1988, 1991), Eason (1999) andValentine (2001). For male managers a compromising style was their first choice, whereas for female managers this style was their last choice.
Viewed from the perspective of gender, the process by which women are socialised encourages them to build relationships and to bring people together, not to drive them apart. Women are generally culturally trained to bemore concerned with interpersonal aspects of relationships than are men, often subordinating their own interests, preferences and needs to those of others. Generally speaking, it is believed that cooperativeness is more characteristic of women and assertiveness is more representative of the traits that men possess. Therefore it is not surprising to find that the female nurse managers in this study preferred an avoiding style followed by a collaborating style, whereas the male nurse managers preferred a compromising style followed by an integrating style.
Female nurses tend to view the handling of conflict as a way to seek affirmation and support while also attempting to maintain harmony (Valentine, 2001). Because nurse managers work in contexts in which they are unlikely to occupy the most powerful positions, the choice of conflict management styles may, in part, be based on the powerlessness associated with these positions. Women have been accustomed to depend on others in order to meet their emotional needs, and to value support. Conflict is seen as a distancing behaviour that may result in rejection.
Nursing education and conflict management
This study found that nursing education has an effect on conflict management styles. There was a significant difference between compromising (P = 0.019), obliging (P = 0.003), dominating (P = 0.006) and integrating (P = 0.033) styles. Research findings on the effect of educational level on preferences for conflict management styles have been inconsistent. Qatan (2001), Dmour (2004) and Hendel et al (2005) found that educational level played no significant role in the choice of such styles. On the other hand, Harem (2003) observed a relationship between educational level and the dominating and avoiding styles. This study found that nursing education has an effect on conflict management styles. Nurse managers with a diploma degree in nursing preferred obliging and avoiding styles, because they felt powerless. Individuals may believe that knowledge confers power. This belief might cause someone with a diploma degree to feel powerless by comparison with an individual with a university or specialised degree. Those with diploma degrees are in nursing management posts without the appropriate designation, and therefore they try to oblige their supervisors and avoid conflict because they have no knowledge of conflict management styles. The specialised nursing diploma is a one-year course, and nursing management is one of the specialised diplomas offered in Oman. Students are taught conflict management strategies during this course. When such a student obtains a specialised diploma, they will be in charge of departments, secure in their management position, and more knowledgeable than other members of staff. The majority of nurses with Bachelor degrees who participated in this study were non-Omani, and nationality plays a role in the selection of conflict management style. The Omani nurse managers with Masters degrees mainly graduated fromUS institutions, and in addition to possessing qualifications that are considered to be the highest in the nursing profession in Oman, they are now also in the top nursing posts.
Management level and conflict management styles
It seems that nurse managers at the three management levels used all of the conflict management styles, but in different orders of preference. There is a significant difference between the integrating, dominating and obliging styles. Previous research yielded conflicting findings regarding the effect of management levels on the choice of conflict management styles. Chusmir and Mills (1989) found no effect, whereas Barton (1991) reported that assistant heads of nursing used an avoiding style more than nurses at the other two management levels, and that nurse administrators used a competing style as their second choice, while for assistant heads and heads of nursing a competing style was their last choice. Harem (2003) showed that first-level department heads used the avoiding style more than administrators did. First-level nurse managers used the obliging and dominating styles as their first two choices, which may be due to the fact that their entry-level management position places them in the role of subordinate more frequently than is the case for the other two management groups. This means that they tend to oblige their supervisors and dominate their subordinates.
The top-level nurse managers have managerial positions in nursing departments and they report to the chief executive officer. It is therefore not unexpected that they used the integrating style with subordinates from the nursing staff to get work done. At the same time they used the compromising style with the administration. From the present researcher’s experience, when the administration asks them to move nurses they ask for some return for nursing. For example, they will agree to transfer a particular nurse to the laboratory or X-ray department if they are given one medical orderly.
Marital status and conflict management styles
The effect of marital status on the obliging style is clear. Previous research has found no effect of marital status on conflict management styles. Married nurses, especially women, who represented the majority of participants in this study, preferred the avoiding and obliging styles. As the majority of nurses are women, they have a busy home life and a large amount of domestic responsibility, so they try to avoid conflict at work so that their home lifewill not be affected by this.
Age and number of years of experience
There is a negative relationship between age and number of years of experience as registered nurse on the one hand, and the obliging and dominating styles on the other. Previous nursing research has found no effect of age on conflict management styles, although Harem (2003) found a negative relationship between the avoiding style and age, and a positive relationship between the dominating style and age. Cetin and Hacifazhoglu (2004) found a positive relationship between age and the integrating style. Age is a very important source of respect in traditional Arab society, and provides legitimacy and credibility for intervention in social conflict, regardless of the nature of the dispute (Abu-Nimer, 1996). In Arab countries, the age of a person is the one factor that commands respect regardless of their educational level or role in the organisation.
A negative relationship was found between experience in the current post and the avoiding style. In previous research, Hendel et al (2005) found that the longer nurse managers were in position, the more they used the collaborating style. The negative relationship between the avoiding style and experience in the current post was related to the effect of poor conflict management on the departments’ outcomes. The longer nurses stay in post, the less they will be able to avoid daily conflict, because any conflict that is avoided will reappear and will eventually affect the working environment. They therefore know that they must try to manage the conflict directly rather than ignore it.
Recommendations
Research is needed to establish the cultural meanings of the five conflict management styles. Studies can determine whether these meanings are understood differently by people from communalist and individualist cultures, as well as by various sub-cultural groups.
Future research could also establish new, standardised instruments for assessing conflict management style, which would eliminate any cultural biases. These instruments could then be used to accurately measure differences in management styles between cultures, when nurses from different cultural regions are participating in a study.
Further research is needed to explore the conflict management styles used by nurse managers in the countries whose nationals took part in this study, in order to find out whether they use different styles when working in their own countries.
Conclusion
Nurse managers work in an environment where conflict is likely to occur and can be difficult to manage because of the different ways in which participants view it, especially when they are from different cultures, of different genders, and have different nursing qualifications. There is a need to understand conflict management from the perspectives of nurse managers. This understanding would improve nurses’ evaluation of how to handle conflict situations. Conflict management styles that incorporate nurse managers from different cultures and of both genders will help to balance the knowledge base with regard to organisational, cultural diversity and administrative aspects of the nursing literature. Gaining insight into the values of culture and gender could help nurse managers to better understand conflict management styles using different perspectives, and thereby enhance the environment of nursing organisations.Most studies of conflict management styles have been conducted in Western countries. This study goes further by examining conflict management styles within an Arab country, and it shows how, in that setting, nurse managers at different levels in the organisation, from different cultures and with different qualifications, manage conflict.
Acknowledgment
The author would like to thank Professor Denis Anthony and Dr Raghda Shukri for their help in preparing this study by providing supervision and statistical advice during the completion of a PhD thesis, on which this paper is based.
CONFLICTS OF INTEREST
None.
References
- Abu-Nimer M (1996) Conflict resolution approaches: westernand Middle Eastern lessons and possibilities.American Journal of Economics and Sociology 55:35–44.
- Al-Bawab H (1986) Conflict management styles used bysecondary academic school principals in Jordan. UnpublishedMSc thesis, Jordan University, Amman, Jordan (inArabic).
- Al-Belbeisi S (2003) Conflict management styles used by publicsecondary school principals in Jordan and their relationshipto teachersâ€Âââ€Å¾Â¢ morale and organisation commitment. UnpublishedPhD thesis, Arabic University for Graduate Studies,Amman, Jordan (in Arabic).
- Bartol GM, Rebecca P and Maryellen M (2001) Effectiveconflict management begins with knowing your style.Journal for Nurses in Staff Development 17:34–40.
- Barton A (1991) Conflict resolution by nurse managers.Nursing Management 22:83–6.
- Blake R and Mouton J (1964) The Managerial Grid: keyorientations for achieving production through people.Houston, TX: Gulf Publishing.
- Blake R and Mouton J (1985) The Managerial Grid III.Houston, TX: Gulf Publishing.
- BoonsathornW (2003) Competence is in the eye of thebeholder: conflict management styles and perceived competenceof conflict management styles by Thais andAmericans in multinational corporations in Thailand.Unpublished PhD thesis, Pennsylvania State University,University Park, PA.
- Campbell K (2003) The efficacy of conflict-mediation trainingin elementary schools. Educational Forum 67:148–55.
- Cavanagh S (1988) The conflict management style of intensivecare nurses. Intensive Care Nursing 4:118–23.
- Cavanagh S (1991) Conflict management style of staff nursesand nurse managers. Journal of Advanced Nursing16:1254–60.
- Cetin OM and Hacifazhoglu O (2004) Conflict managementstyles: a comparative study of university academics andhigh school teachers. Journal of the American Academy ofBusiness 5:325–32.
- Chusmir L and Mills J (1989) Gender differences in conflictresolution styles of managers: at work and at home. SexRoles 20:149–63.
- De Dreu CK and Van De Vliert E (1997) Using Conflict inOrganizations. London: Sage.
- De Dreu C, Evers A, Beersma B et al (2001) A theory-basedmeasure of conflict management strategies in the
- workplace. Journal of Organizational Behavior 22:645–68.
- Dmour S (2004) Methods used by the educational supervisorin Jordan when dealing with organizational conflict. UnpublishedMSc thesis, Mutah University, Karak, Jordan(in Arabic).
- Eason FR (1999) Conflict management: assessing educationalneeds. Journal for Nurses in Staff Development15:92–6.
- Elsayed-Ekhouly S and Buda R (1996) Organizational conflict:a comparative analysis of conflict styles across
- cultures. International Journal of Conflict Management7:71–81.
- EnnamiAK(1996) Al-Ibadhiyah. Muscat: Ministry of Awqafand Religious Affairs.Forte PS (1997). The high cost of conflict. Nursing Economics15:119–23.
- Harem H (2003) Conflict resolution at the commercialbanks in Jordan. Jordanian Journal for Applied Sciences6:47–67 (in Arabic).
- Hendel T, Fish M and Galvon V (2005) Leadership style andchoice of strategy in conflict management among Israelinurse managers in general hospitals. Journal of NursingManagement 13:137–46.
- Hofstede G (1983) National cultures in four dimensions: aresearch-based theory of cultural differences amongnations. International Studies of Management and Organization8:46–74.
- HofstedeG(2001) Cultureâ€Âââ€Å¾Â¢s Consequences: comparing values,behaviors, institutions, and organizations across nations.Thousand Oaks, CA: Sage.
- Hurst JB and KeenanGM(2000) Conflict: the cutting edge ofchange. In: Yoder-Wise P (ed.) Leading and Managing inNursing. New York: Mosby.
- Jameson JK (1999) Towards a comprehensive model for theassessment and management of intra-organizational conflict:developing the framework. International Journal ofConflict Management 10:268–94.
- Keenan G, Cook R and Hillis S (1998) Norms and nursemanagement of conflict: keys to understanding nurse–physician collaboration. Research in Nursing and Health21:59–72.
- Kozan MK (1989) Cultural influences on styles of handlinginterpersonal conflict: comparisons among Jordanian,Turkish, and US managers. Human Relations 42:787–99.
- Kozan MK (2002) Subcultures and conflict managementstyle. Management International Review 42:89–105.
- Kozan MK and Ergin C (1999) The influence of intraculturaldifferences on conflict management styles. InternationalJournal of Conflict Management 10:249–67.
- Kramer RM (1989) Windows of vulnerability or cognitiveillusions? Cognitive processes in the nuclear arms race.Journal of Experimental Social Psychology 25:79–100.
- Kunaviktikul W, Nuntasupawat R, SrisuphanWet al (2000)Relationships among conflict, conflict management, jobsatisfaction, intent to stay, and turnover of professionalnurses in Thailand. Nursing and Health Sciences 2:9–16.
- Levine SP and Feldman RS (1997) Self-presentational goals,self-monitoring, and nonverbal behaviour. Basic andApplied Social Psychology 19:505–18.
- McElhaney R (1996) Conflict management in nursingadministration. Nursing Management 24:65–6.
- Marriner TA (1982) Managing conflict. Nursing Management13:29–31.
- Ministry of Health (2006) Annual Health Report 2005.Muscat: Ministry of Health; www.moh.gov.om/nv_menu.php?fNm=stat/HStatMOH.php (accessed 28 August2008).
- Ministry of National Economy (2004) Final Results of theCensus 2003; www.omancensus.net/english/pdf_files/
- final_results.pdf (accessed 17 September 2008).
- Pondy LR (1967) Organizational conflict: concepts andmodels. Administrative Science Quarterly 12:296–320.
- Qatan T (2001) Organizational conflict management stylesamong secondary school principals in the Sultanate ofOman. Unpublished MSc thesis, Sultan Qaboos University,Muscat, Oman.
- Rahim AM (1983) A measure of styles of handling interpersonalconflict. Academy of Management Journal 26:368–76.
- Shockley-Zalabak P (1981) The effects of sex differences onthe preferences for utilization of conflict styles of managersin a work setting. Public Personnel ManagementJournal 10:289–95.
- Tabak N and Koprak O (2007) Relationship between hownurses resolve their conflicts with doctors, their stress andjob satisfaction. Journal of Nursing Management 15:321–31.
- Tengilimoglu D and Kisa A (2005) Conflict management inpublic university hospitals in Turkey: a pilot study. HealthCare Manager 24:55–60.
- Thomas KW and Kilmann RH (1974) Thomas-KilmannConflict Mode Instrument. Mountain View, CA: Xicomand CPP, Inc.
- Ting-Toomey S, Yee-Jung KK, Shapiro RB et al (2000)Ethnic/cultural identity salience and conflict styles infour US ethnic groups. International Journal of InterculturalRelations 24:47–81.
- Valentine PE (2001) A gender perspective on conflict managementstrategies of nurses. Journal of Nursing Scholarship33:69–74.
- Vivar CG (2006) Putting conflict management into practice:a nursing case study. Journal of Nursing Management14:201–6.
- Woodtli A (1987) Deans of nursing: perceived sources ofconflict and conflict-handling modes. Journal of NursingEducation 26:272–7.
- Yu Xu and Davidhizar R (2004) Conflict management stylesof Asian and Asian American nurses. Health Care Manager23:46–53.

