Anastasios T Dimou1, Konstantinos N Syrigos2, Muhammad Wasif Saif3
1Department of Pathology, Yale University School of Medicine. New Haven, CT, USA.
2Oncology Unit, Third Department of Medicine, University of Athens. Athens, Greece.
3Columbia University College of Physicians and Surgeons and Pancreas Center, New York Presbyterian Hospital. New York, NY, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Columbia University
College of Physicians and Surgeons and the Herbert Irving Cancer Center
177 Fort Washington Avenue, Suite 6-435
New York, NY 10032; USA
Phone: +1-212.305.4954
Fax: +1-212.3050.3035
E-mail: mws2138@columbia.edu
Keywords
adverse effects; Clinical Trials, Phase I as Topic; Mitogen-Activated Protein Kinase Kinases; Pancreatic Neoplasms
Abbreviations
CTGF: connective tissue growth factor; HSV: herpes simplex virus; MAPKK, MEK: mitogen-activated protein kinase kinase
Background
Prognosis for pancreatic adenocarcinoma remains dismal [1]. In the metastatic setting, gemcitabine and erlotinib treatment results in a median overall survival of 6 months [2] whereas recently, the combination of 5-fluorouracil, leucovorin, irinotecan and oxaliplatin (FOLFIRINOX) has proven superior to the gemcitabine-erlotinib regimen at the cost of significant toxicity [3]. Thus, taking into account the shortage of effective compounds, development and testing of novel agents is necessary.
KRAS is a small GTPase bound to the cell membrane that drives major oncogenic pathways in human cancer. In addition, KRAS is mutated and constantly active in the vast majority of pancreatic adenocarcinomas [4] rendering a rationale for inhibition of that particular pathway at a level downstream of KRAS. Mitogenactivated protein kinase kinase (MAPKK or MEK) is an appealing target in this regard. Desmoplasia is another property of pancreatic adenocarcinoma that is responsible for resistance to existing treatments, since systemic compounds find it hard to penetrate through the thick fibrotic stroma [5]. Hence, designing treatment strategies that reduce tumor stroma emerges as an interesting approach. Anti-angiogenesis drugs have failed to prove effective in clinical trials illustrating the complex biology of tumor angiogenesis in pancreatic cancer [6]. It has been shown that anticoagulation can exert some anti-angiogenic properties in pre-clinical models providing an additional strategy of targeting tumor vasculature [7]. Finally, gene therapy might be an alternative for clinical trial design, given the emerging technology of gene delivery and engineering of tumor genomes.
What We Learnt at 2011 ASCO GI Cancer Symposium
Addition of MEK Inhibition to Standard Gemcitabine Treatment in Pancreatic Cancer
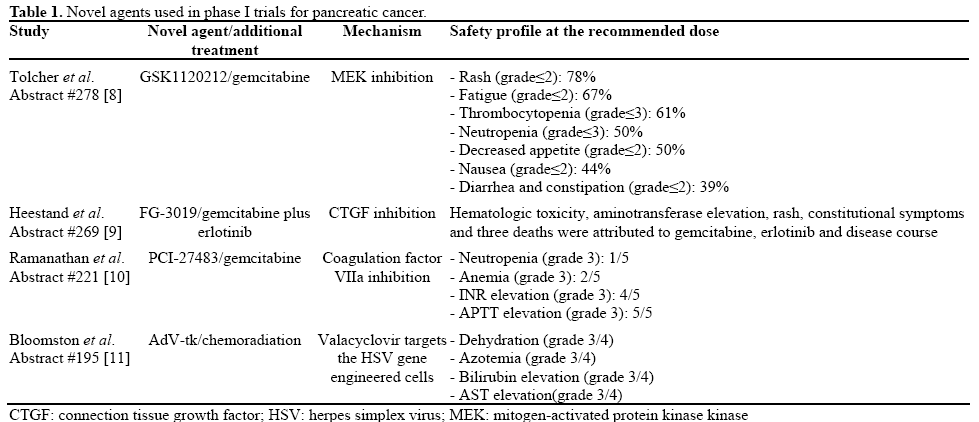
GSK1120212 is a reversible and specific inhibitor of MEK. Toicher et al. [8] (Abstract #278)have studied the safety profile, pharmacokinetic properties and potential efficacy of this compound in combination with gemcitabine in a panel of advanced solid tumors in the context of a phase Ib trial. Eight patients with pancreatic cancer were included in the studied population. Maximal tolerated dose was defined to be the combination of 2 mg of GSK1120212 given orally once daily with 1000 mg/m2 given on days 1, 8 and 15 every 28 days. Febrile neutropenia, aminotransferase elevation and uveitis limited further increase in dosage. Pneumonitis, febrile neutropenia and dyspnea were attributed to treatment on five occasions among 16 serious adverse events that were observed. Hematologic and gastrointestinal toxicity, as well as rash and constitutional symptoms (fatigue, loss of appetite), were the most frequent adverse events reported. There was no pharmacokinetic interaction between gemcitabine and GSK1120212. Interestingly, one patient with pancreatic cancer achieved a partial response and another 3 patients experienced stabilization of their disease for several months.
Connective Tissue Growth Factor is a Candidate Target in Pancreatic Cancer
FG-3019 is a monoclonal antibody against connective tissue growth factor (CTGF) which was tested in a phase I study by Heestand et al. [9] (Abstract #269). The experimental drug was administered every 2 weeks at 4 dose levels: 3, 10 and 15 mg/m2. After the first dose, erlotinib and gemcitabine were added. Seven severe adverse events and three additional adverse events including rash, hematologic toxicity and aminotransferase elevation were reported after gemcitabine and erlotinib were administered. Toxicity did not seem to be related to FG-3019. On the contrary, it correlated with the known spectrum of gemcitabine or erlotinib toxicity and the natural history of the disease. In this context, three deaths from sepses, suicide and tumor progression were reported among the severe adverse events. Patients progressed after a median time of 3.7 months and had a median survival of 9.4 months. Since a maximal tolerated dose was not defined, more patients were accrued to receive 25 mg/m2 FG-3019.
Anti-Coagulation as a Possible Anti-Angiogenesis Strategy
Ramanathan et al. [10] (Abstract #221) have studied the safety profile of PCI-27483, a small inhibitor that inhibits the coagulation factor VIIa in a selective fashion. They administered this compound in combination with gemcitabine in patients with advanced pancreatic cancer in the context of a phase I trial. Gemcitabine was administered at a fixed dosage of 1,000 mg/m2 on days 1, 8 and 15 every 4 weeks, whereas for the experimental drug, dosage was escalated in each patient in a three step fashion: 0.8, 1.2 and 1.8 mg/kg over the course of 4 to 8 weeks administered subcutaneously twice daily. An INR of 3 measured 2 hours after the injection of PCI-27483 was targeted as a surrogate for adequate anti-coagulation. Among the 5 evaluable patients of the study, grade 3 hematologic toxicity was observed in 3 patients whereas all the patients experienced a grade 3 elevation of INR, APTT or both. Four out of five patients were able to stabilize their disease for at least 4 months. The dose of PCI-27483 recommended for phase II trials is 1.2 mg/kg.
Anti-Herpetic Treatment Following Integration of a Herpes Simplex Virus (HSV) Gene in Pancreatic Cancer Cells
Bloomston et al. [11] (Abstract #195) performed a phase I study where they delivered an adenovirus vector containing HSV thymidine synthase gene in patients with locally advanced pancreatic cancer via endoscopic ultrasound or externally under computerized tomography guidance. Subsequently they treated their patients with the anti-herpetic drug valacyclovir for 14 days following the adenoviral delivery. Finally, patients received 5-FU based chemoradiation following the standard protocol and beginning from week 3. A total of 12 patients were accrued and assigned to 4 different dose levels of the adenoviral vector ranging from 3x1010 to 1012 vector particles. Although a number of grade 3 or 4 toxicities were observed including dehydration, azotemia, bilirubin and aminotransferase elevation, no dose limiting adverse events were reported. Efficiency of the protocol was promising with median overall survival being 12.2 months and 2 patients achieving a partial response (Table 1).
Discussion
MEK inhibition has been tested before in pancreatic and other cancers using a different compound, CI-1040 but proved inefficient [12]. GSK1120212, is a novel MEK inhibitor that has unique pharmacokinetic properties and a broader therapeutic window than previous MEK inhibitors [13]. It might therefore prove more effective in phase II studies. FG-3019 has been tested before in a phase I study in patients with diabetes and albuminuria [14]. Likewise to the current study by Heestand et al., it was well tolerated by patients in the non-oncology setting. PCI-27483 inhibits coagulation factor VIIa which is a serine protease. Tissue factor localizes VIIa to the cell membrane and it has been suggested that the tissue factor:VIIa complex promotes pro-angiogenic signals in tumors [7]. Adenovirus mediated HSV gene delivery followed by anti-herpetic drugs has been tested in glioblastoma [15], retinoblastoma [16], hepatocellular carcinoma [17] and head and neck tumors [18] previously. It has been shown both promising and safe in all those settings. Given the results of Bloomston et al. [11] (Abstract #195), it remains to see whether this strategy is of any value in pancreatic cancer phase II studies.
Overall it appears that a number of novel compounds are ready to be tested in phase II trials in patients with pancreatic cancer taking into account their reasonable toxicity spectrum as presented in the 2011 ASCO GI Cancer Symposium.
Conflict of interest
The authors have no potential conflict of interest
References
- Hidalgo M. Pancreatic cancer. N Engl J Med 2010; 362:1605- 17. [PMID 20427809]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6. [PMID 17452677]
- Kim R. FOLFIRINOX: a new standard treatment for advanced pancreatic cancer? Lancet Oncol 2011;12:8-9. [PMID 21050812]
- Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell 1988; 53:549-54. [PMID 2453289]
- Mahadevan D, Von Hoff DD. Tumor-stroma interactions in pancreatic ductal adenocarcinoma. Mol Cancer Ther 2007; 6:1186- 97. [PMID 17406031]
- Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, et al. Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: phase III trial of the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol 2010; 28:3617-22. [PMID 20606091]
- Kasthuri RS, Taubman MB, Mackman N. Role of tissue factor in cancer. J Clin Oncol 2009; 27:4834-8. [PMID 19738116]
- Tolcher AW, Bendell JC, Patnaik A, Papadopoulos K, Bellew KM, Cox DS, Xu Y, et al. A phase Ib study of the MEK inhibitor GSK1120212 combined with gemcitabine in patients with solid tumors: Interim results. J Clin Oncol 2011; 29(Suppl. 4):Abstract 278.
- Heestand GM, Pipas JM, Valone F, Mc Mullen AD, Gadea P, Williams D, Zhong M, et al. A phase I trial of the monoclonal antibody FG-3019 to connective tissue growth factor (CTGF) in locally advanced or metastatic pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 269.
- Ramanathan RK, Gressler V, Shah S, Loury D, Hamdy A, Khorana A. A Phase I/II study of PCI-27483, a coagulation factor VIIa (FVIIa) inhibitor in patients with advanced pancreatic cancer receiving treatment with gemcitabine. J Clin Oncol 2011; 29(Suppl. 4):Abstract 221.
- Bloomston M, Marsh C, Walker J, Coyle W, Marx H, Tahiri S, Moran Cruz C, et al. Phase I trial of gene-mediated cytotoxic immunotherapy in combination with chemoradiation for locally advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 195.
- Rinehart J, Adjei AA, Lorusso PM, Waterhouse D, Hecht JR, Natale RB, Hamid O, et al. Multicenter phase II study of the oral MEK inhibitor, CI-1040, in patients with advanced non-small-cell lung, breast, colon, and pancreatic cancer. J Clin Oncol 2004; 22:4456-62. [PMID 15483017]
- Gilmartin AG, BleamMR, Groy A, Moss KG, MinthornEA, KulkarniSG, Rominger CM, et al. GSK1120212 (JTP-74057) is an inhibitor of MEK activity and activation with favorable pharmacokinetic properties for sustained in vivo pathway inhibition. Clin Cancer Res 2011 Jan 18. [PMID 21245089]
- Adler SG, Schwartz S, Williams ME, Arauz-Pacheco C, Bolton WK, Lee T, Li D, et al. Phase 1 study of anti-CTGF monoclonal antibody in patients with diabetes and microalbuminuria. Clin J Am Soc Nephrol 2010; 5:1420-8. [PMID 20522536]
- Sandmair AM, Loimas S, Puranen P, Immonen A, Kossila M, Puranen M, Hurskainen H, et al. Thymidine kinase gene therapy for human malignant glioma, using replication-deficient retroviruses or adenoviruses. Hum Gene Ther 2000; 11:2197-205. [PMID 11084677]
- Chévez-Barrios P, Chintagumpala M, Mieler W, Paysse E, Boniuk M, Kozinetz C, Hurwitz MY, et al. Response of retinoblastoma with vitreous tumor seeding to adenovirus-mediated delivery of thymidine kinase followed by ganciclovir. J Clin Oncol 2005; 23:7927-35. [PMID 16258092]
- Li N, Zhou J, Weng D, Zhang C, Li L, Wang B, Song Y, et al. Adjuvant adenovirus-mediated delivery of herpes simplex virus thymidine kinase administration improves outcome of liver transplantation in patients with advanced hepatocellular carcinoma. Clin Cancer Res 2007; 13:5847-54. [PMID 17908978]
- Xu F, Li S, Li XL, Guo Y, Zou BY, Xu R, Liao H, et al. Phase I and biodistribution study of recombinant adenovirus vector-mediated herpes simplex virus thymidine kinase gene and ganciclovir administration in patients with head and neck cancer and other malignant tumors. Cancer Gene Ther 2009;16:723-30. [PMID 19363470]

