Keywords
Carcinoid Tumor; Neuroendocrine Tumors;
Octreotide; TOR Serine-Threonine Kinases; Therapeutics
Abbreviations
RADIANT: RAD001 in Advanced Neuroendocrine
Tumors
What we Knew Prior to the 2013 ASCO Gastrointestinal
Cancers Symposium
Gastroenteropancreatic neuroendocrine tumors (NET)
are a clinically diverse group of diseases that arise from
tissue throughout the gastrointestinal tract. Symptoms
are often related to molecules secreted by the tumors.
Well differentiated tumors, traditionally referred to as
carcinoid and islet cell tumors or pancreatic NET, often
have more indolent courses compared to other
epithelial carcinomas, whereas poorly differentiated
tumors have a more aggressive course [1]. The
incidence and prevalence of these tumors have
increased over the past 30 years and a significant
percentage has distant disease at diagnosis [1, 2]. Fiveyear
survival is approximately 60%, but no significant
improvement has been made on overall survival over
the past 30-40 years [1].
Recently, treatment of advanced gastroenteropancreatic
NET has made significant advancements, with new
approved agents and new drug combinations.
Everolimus, a mammalian target of rapamycin (mTOR)
inhibitor showed benefit in pancreatic NET. In the
RAD001 in Advanced Neuroendocrine Tumors
(RADIANT)-3 study, patients with unresectable pNET
treated with everolimus had improved progression free survival compared to placebo (11.0 vs. 4.6 months) [3].
Similarly, patients with advanced pNET treated with
sunitinib vs. placebo showed improvement in
progression free survival (11.4 vs. 5.5 months) [4].
Along with these targeted therapies, somatostatin
analogs, long used to control symptoms in carcinoid
tumors, have been shown to have antitumor effect.
Octreotide was compared to placebo in the PROMID
trial in patients with metastatic carcinoid tumors of the
midgut, showing improved time to tumor progression
(14.3 vs. 6 months) [5]. Heightened interest in systemic
treatment of gastroenteropancreatic neuroendocrine
tumors has been increased due to these recent
advancements.
What We Learned from the 2013 ASCO Gastrointestinal
Cancers Symposium
Efficacy and Safety of Everolimus in Patients with
Advanced Low- or Intermediate-Grade Pancreatic
Neuroendocrine Tumors Previously Treated with
Chemotherapy: RADIANT-3 Subgroup Analysis.
(Abstract #224).[6]
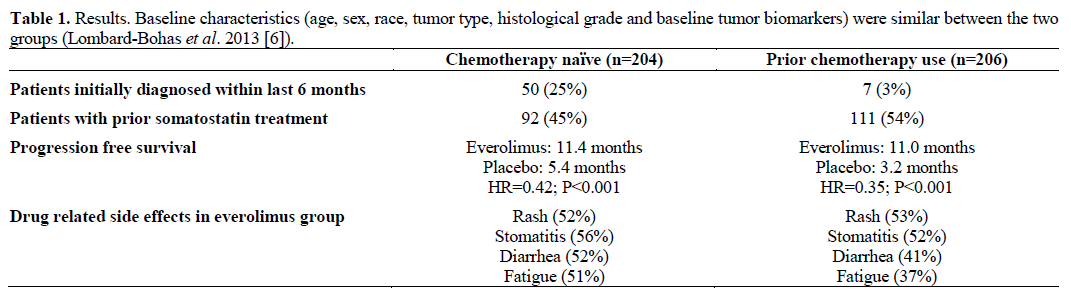
Lombard-Bohas et al. presented data from a planned
exploratory analysis of the phase III RADIANT-3 trial.
Patients with low or intermediate grade pancreatic NET
(pNET) were stratified prospectively by prior
chemotherapy use. The patients were then randomized
to receive either everolimus 10 mg daily or placebo
plus best supportive care. Results are summarized in Table 1. Best overall response was stable disease in
73% of everolimus treated patients in both groups.
Disease stabilization and decreased disease progression
was seen with everolimus regardless of prior chemotherapy. This subgroup analysis shows a benefit of
everolimus in low and intermediate grade pNETs
independent of prior chemotherapy use and supports
possible first-line use of everolimus.
Octreotide LAR Use Among Elderly Patients with
Carcinoid Syndrome and Survival Outcomes: A
Population-Based Analysis (Abstract #322) [7].
Shen et al. performed a retrospective study evaluating
octreotide LAR use in elderly patients with carcinoid
syndrome and survival differences. NET patients were
identified using the Surveillance, Epidemiology and
End Results (SEER)-Medicare database from July
1999 to December 2007 (https://healthservices.cancer.
gov/seermedicare/). Indications for octreotide use
included 2 or more claims for carcinoid syndrome,
flushing, diarrhea or malignant islet cell neoplasm
within one year of diagnosis and the first claim within
6 months of diagnosis. Patients were excluded if under
age 65, enrolled in a health maintenance organization
(HMO) or without continuous part A and B enrollment
(https://www.medicare.gov/Pubs/pdf/11219.pdf) within
12 months of diagnosis. Cox proportional hazard
model and multivariate logistic regression analysis
were used to evaluate factors associated with octreotide
use and effect of octreotide on survival. The study
found that among patients with indications for
octreotide use, only 264/539 (49.0%) distant stage
patients and 83/850 (9.8%) local/regional stage patients
were started on therapy within 6 months of diagnosis.
Patients living in southern regions were less likely to
be treated. A significant 5-year survival benefit was
seen with distant stage disease (HR=0.80; P=0.047) but
no benefit in local/regional stage disease (HR=0.97;
P=0.89). This study shows a potential survival benefit
to octreotide use in elderly patients with distant stage
carcinoid syndrome and that many elderly patients with
indications for octreotide are not receiving therapy
early in the disease course.
Discussion
The treatment of advanced gastroenteropancreatic
NETs continues to rapidly evolve. Targeted therapies
have a significant role in this advancement. mTOR
inhibitors, such as everolimus target cell proliferation
and angiogenesis and sunitinib, a multikinase inhibitor,
inhibit vascular endothelial growth factor (VEGF).
Agents that disrupt angiogenesis have shown
significant activity in pancreatic NETs. Table 2 summarizes the use of everolimus in gastroenteropancreatic
NETs. Lombard-Bohas et al. showed in a
planned subgroup analysis of the RADIANT-3 trial
that everolimus improved progresssion free survival
irrespective of prior chemotherapy use with no
significant difference in side effect profiles [6]. This
data further supports upfront use of everolimus for
advanced pancreatic NETs.

Therapies for carcinoid tumors were also addressed at
the 2013 ASCO Gastrointestinal Cancers Symposium.
Octreotide LAR has long been used for treatment of
carcinoid syndrome symptoms, but more recently has
shown to also delay tumor progression [5]. The
retrospective analysis presented by Shen et al. found a
possible 5-year survival advantage of octreotide LAR
use in elderly (age older than 65 years) patients with
distant stage disease [7]. The group also found that a
minority of patients with symptoms of carcinoid
syndrome are receiving prompt treatment of their
disease. Further prospective trials are needed to
evaluate these findings.
Conflict of interest
The authors have no potential
conflict of interest
References
- Yao, James C et al. "One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States." Journal of Clinical Oncology 26.18 (2008): 3063-3072. PMID: 18565894
- Oberg, K. “Gastrointestinal Neuroendocrine Tumors.” Annals of Oncology Supplement 7.(2010):vii72-80.
- Yao, James C et al. "Everolimus for advanced pancreatic neuroendocrine tumors." New England Journal of Medicine 364.6 (2011): 514-523. PMID: 21306238.
- Raymond, Eric et al. "Sunitinib malate for the treatment of pancreatic neuroendocrine tumors." New England Journal of Medicine 364.6 (2011): 501-513. PMID: 21306237
- Rinke, Anja et al. "Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group." Journal of Clinical Oncology 27.28 (2009): 4656-4663. PMID: 19704057
- Lombard-Bohas et al. “Efficacy and safety of everolimus in patients with advanced low- or intermediate-grade pancreatic neuroendocrine tumors previously treated with chemotherapy: Radiant-3 subgroup analysis.” J Clin Oncol 2012; 30 (Suppl. 34): Abstract #224.
- Shen et al. “Octreotide LAR use among elderly patients with carcinoid syndrome and survival outcomes: A population-based analysis.” J Cinical Oncology 2012; 30 (Suppl. 34): Abstract #322.
- Pavel, Marianne E et al. "Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study." The Lancet 378.9808 (2011): 2005-2012. PMID: 22119496

