Keywords
cytotoxic T-lymphocyte antigen 4; ixabepilone; Pancreatic Neoplasms; Receptor, IGF Type 1; Receptors, Somatomedin; Taxoids
Abbreviations
CTLA-4: cytotoxic T lymphocyte antigen 4; IGF- 1R: insulin growth factor receptor-1
Introduction
Pancreatic cancer is the fourth leading cause of cancer related death in USA [1]. Despite the efforts and the research done so far, the prognosis of the disease remains dismal. In the metastatic setting of the disease, only gemcitabine and erlotinib have demonstrated some efficacy. Eventually, the tumors become refractory to those agents and treatment options after that point are limited to best supportive care or participation in a clinical trial [2]. It is therefore necessary that new targets will be discovered and novel compounds will be tested in clinical trials.
This is a review from the recent 2010 American Society of Clinical Oncology (ASCO) Annual Meeting concerning abstracts about new drugs tested in clinical trials in patients with pancreatic adenocarcinoma. Five abstracts were reviewed: the first two include inhibition of the insulin growth factor receptor-1 (IGF-1R) pathway, another two test the combination of microtubule stabilization and epidermal growth factor receptor (EGFR) inhibition and the last one assesses the toxicity profile of a cytotoxic T lymphocyte antigen 4 (CTLA-4) inhibitor.
Insulin Growth Factor Receptor-1 (IGF-1R) Blockade in Pancreatic Cancer
IGF-1R pathway has been described in pancreatic adenocarcinoma [3]. Briefly, PI3K and AKT which control mTOR activation in stimulating cell survival and growth lay downstream of the receptor. Crosstalk with the EGFR and other pathways may account for the resistance of the tumor cells to anti EGFR therapy and underscores that single pathway inhibition might not be enough. There have been two studies that were recently presented and that include inhibition of the IGF-1R pathway in one of their arms.
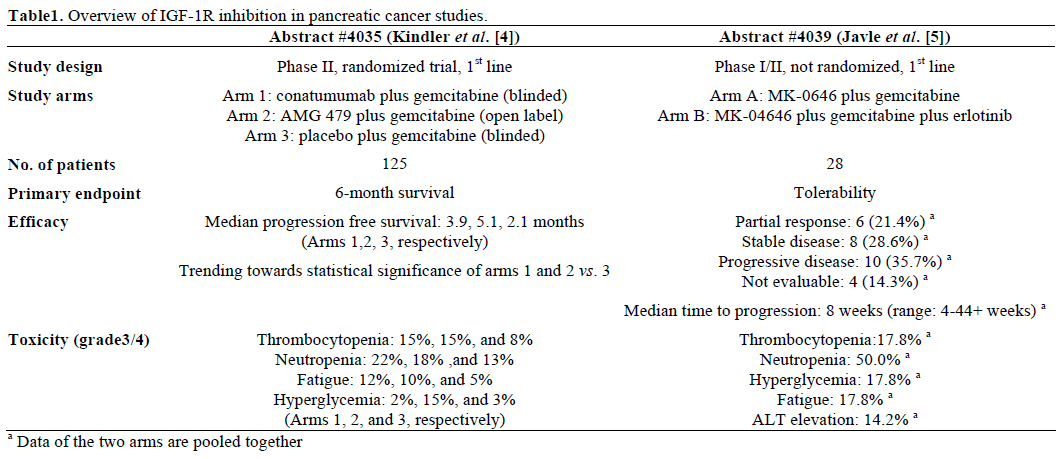
Kindler et al. [4] presented a phase II trial in the first line setting of metastatic pancreatic cancer introducing AMG 479, an anti-IGF-1R compound and conatumumab, a death receptor 5 agonist among the treatment arms. Patients were randomized to receive conatumumab plus gemcitabine (1st arm), AMG 479 plus gemcitabine (2nd arm) or gemcitabine plus placebo (3rd arm). The study did not meet its primary endpoint which was an improvement in 6-month survival among the experimental and the placebo arms. However, the results look promising as a trend towards improved progression free survival was shown, as well as an increase in the percentage of patients that achieved stable disease. Treatment was generally well tolerated with most common grade 3/4 toxicities being neutropenia, thrombocytopenia, fatigue and hyperglycemia. It is important that AMG 479 administration was not blinded at the fear of thrombocytopenia and hyperglycemia which along with the large number of centers that participated in the study (37 for 125 patients) could introduce a possible bias. Last but not least, the study was designed to detect a difference of 24% in 6-month overall survival between the placebo and the experimental arms with a power of 80%, but it was under powered to demonstrate smaller differences. Overall, there was a trend towards benefit from adding IGF-1R inhibition, or even conatumumab to gemcitabine in patients with metastatic pancreatic cancer in this study but larger studies are needed to prove whether this strategy can be a realistic treatment option.
Javle et al. [5] performed a phase I trial of an anti IGF- 1R antibody, MK-0646 in combination with gemcitabine or erlotinib in chemo-naïve patients with metastatic pancreatic cancer. A dose of 10 mg/kg over 60 min of MK-0646 weekly was tolerable in combination with 1,000 mg/m2 over 100 min of gemcitabine on days 1, 8 and 15 of 28 days cycles (arm A). When erlotinib (100 mg/day) was added to the previous regimen (arm B), MK-0646 was better tolerated at a dose of 5 mg/kg over 60 min weekly because of dose limiting febrile neutropenia and transaminases elevation occurring in two of the 28 patients (7.1%). Among grade 3/4 toxicities, neutropenia was a concern as it occurred in 50% of the 28 patients, whereas thrombocytopenia, fatigue, ALT elevation and hyperglycemia were less frequent. Interestingly, a partial response was reported in 6 out of the 28 patients enrolled (21.4%). A phase II trial is ongoing comparing these two regimens with the standard combination of gemcitabine plus erlotinib.
Table 1 summarizes the results of the two studies of IGF-1R inhibition in pancreatic cancer that were recently presented in the 2010 ASCO Annual Meeting.
Epothilones and Novel Taxanes in the Treatment of Pancreatic Cancer
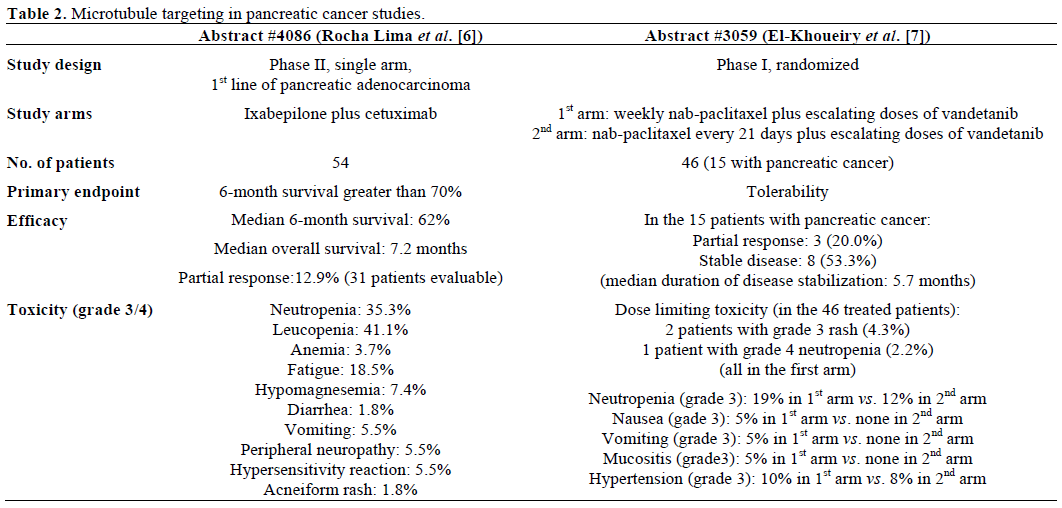
Ixabepilone, which acts in stabilizing microtubules in a different manner than taxanes, was used in combination with cetuximab in previously untreated patients with advanced pancreatic adenocarcinoma [6]. The primary endpoint of this non randomized single arm study (i.e., to show a 6-month survival greater than 70%) was not met. The study showed a trend of benefit among the patients that developed a rash. Most common grade 3/4 toxicity was neutropenia and fatigue. Biomarker analysis failed to show any impressive correlation of benefit from the combination with EGFR expression.
El-Khoueiry et al. [7] performed a phase I trial of nabpaclitaxel and vandetanib at different doses and schedules in patients with refractory metastatic solid tumors. A total of 15 patients with pancreatic cancer were included in the cohort (33%). Dose of nabpaclitaxel was fixed but given either on a weekly basis or every three weeks and escalating doses of vandetanib (100, 200 and 300 mg po daily) were added to both schedules. Maximal tolerated dose for vandetanib was decided to be 300 mg po daily for both nab-paclitaxel arms. Nab-paclitaxel was generally better tolerated when given every 3 weeks than weekly. Interestingly, even in this refractory setting, 3 out of 15 patients with pancreatic cancer (20.0%) achieved a partial response and, in addition, 8 patients (53.3%) had stabilization of their disease with a median duration of 5.7 months.
Table 2 summarizes the results of microtubule stabilization in pancreatic cancer studies.
CTLA-4 Blockade in the Treatment of Pancreatic Cancer
CTLA-4 is a receptor on the surface of T lymphocytes that interacts with B7 ligand on the surface of the antigen presenting cells and blocks the activation of T cells. The concept of CTLA-4 blockade in the treatment of tumors is based on the activation of the immune system and the cytotoxic T cells, which has proven effective for the case of melanoma [8].
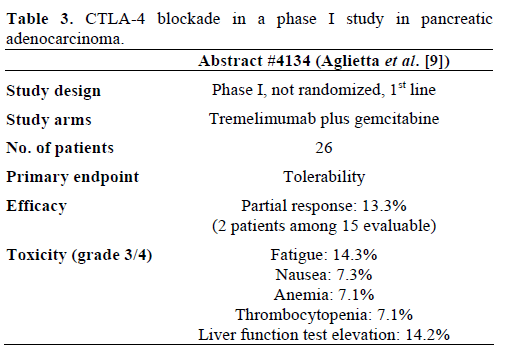
Aglietta et al. [9] presented a phase I study of tremelimumab, a CTLA-4 inhibitor, in escalating doses in combination with gemcitabine in patients with metastatic pancreatic cancer as a first line regimen. Primary endpoint of the study was determination of the maximal tolerated dose for tremelimumab. The regimen showed an acceptable toxicity profile and modest efficacy as shown in Table 3.
Discussion
Novel compounds are needed in the treatment of pancreatic cancer as current treatment options are limited and refractory tumors emerge early in the course of the disease. Here we review five of the trials that contained novel therapeutics and novel targets in their arms that were presented in the 2010 ASCO Annual Meeting.
Inhibition of the insulin growth factor 1 receptor has shown promising results and an acceptable toxicity profile. The phase II trial failed to meet its ambitious primary endpoint. However, given that there is a trending benefit in the phase II study as well as a number of responses in the phase I study, it is likely that the possible benefit from IGF-1R inhibition is modest and can be demonstrated only by a large phase III trial that will include the standard combination of gemcitabine and erlotinib plus placebo or an IGF-1R inhibitor. More importantly, tissue from the trials should be analyzed to answer questions for possible biomarkers:
Can IGF-1R immunohistochemistry predict benefit from IGF-1R inhibitors?
What is the status of the downstream molecules and the collateral pathways in the patients that are refractory to them?
These are only a few of them. It appears that the microtubules are not an appealing target for the patients with pancreatic cancer.
Ixabepilone failed to demonstrate any impressive activity that was apparently better than the course of the disease with the standard of care. Taxanes have failed to justify a phase III trial so far and antiangiogenetic factors have not added any benefit to the standard combination of gemcitabine and erlotinib [10]. However, the combination of anti-angiogenetic factors and taxanes has not been tested so far. The phase I trial by El-Khoueiry et al. [7] is testing the combination of an albumin bound taxane and vandetanib, a dual EGFR and VEGFR inhibitor, and demonstrates some efficacy with acceptable toxicity. A phase II study would further clarify the possible benefit from this combination in patients with metastatic pancreatic cancer.
Concerning CTLA-4 blockade, it appears that tremelimumab has an acceptable toxicity profile and demonstrates some efficacy in combination with gemcitabine. However, an appropriately designed phase II trial that contains a placebo arm is needed to prove the possible benefit if any, that patients with metastatic pancreatic adenocarcinoma can get from this compound. CTLA-4 blockade has already proven effective in patients with metastatic melanoma, a tumor where immune response is playing a major role and where immune response stimulating agents have been incorporated into clinical practice in the past. It remains to be clarified how pancreatic cancer can interact with the immune system and to what extent this can be of benefit for the patients with this disease. In conclusion, a lot of novel compounds are being tested in clinical trials in patients with pancreatic cancer. It is important that new trials are conducted on the grounds of preclinical evidence for the efficiency of the drugs and it is essential that tissue from the trials will be used in exploring the biology and behavior of those tumors.
Conflict of interest The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer
Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID
19474385]
- Hidalgo M. Pancreatic cancer. N Engl J Med 2010; 362:1605-
17. [PMID 20427809]
- Rozengurt E, Sinnett-Smith J, Kisfalvi K. Crosstalk between
insulin/insulin-like growth factor-1 receptors and G protein-coupled
receptor signaling systems: a novel target for the antidiabetic drug metformin in pancreatic cancer. Clin Cancer Res 2010; 16:2505-11.
[PMID 20388847]
- Kindler HL, Richards DA, Stephenson J, Garbo LE, Rocha Lima
CS, Safran H, et al. A placebo-controlled, randomized phase II study
of conatumumab (C) or AMG 479 (A) or placebo (P) plus
gemcitabine (G) in patients (pts) with metastatic pancreatic cancer
(mPC). J Clin Oncol 2010; 28(15 Suppl):4035.
- Javle MM, Varadhachary GR, Shroff RT, Bhosale B, Overman
BM, Weatherly J, et al. Phase I/II study of MK-0646, the humanized
monoclonal IGF-1R antibody in combination with gemcitabine or
gemcitabine plus erlotinib (E) for advanced pancreatic cancer. J Clin
Oncol 2010; 28(15 Suppl):4039.
- Rocha Lima CS, Lin EH, Kim GP, Giguere JK, Marshall J,
Zalupski M, et al. Phase II trial of ixabepilone (IXA) plus cetuximab
(C) as first-line therapy for advanced pancreatic carcinoma (PC). J
Clin Oncol 2010; 28(15 Suppl):4086.
- El-Khoueiry AB, Iqbal S, Lenz H, Roman L, Gitlitz BJ, Yang D,
et al. A phase I study of two different schedules of nab-paclitaxel
(Nab-p) with ascending doses of vandetanib (V) in patients (pts) with
advanced solid tumors. J Clin Oncol 2010; 28(15 Suppl):3059.
- Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA,
Haanen JB, et al. Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med 2010 Jun 5. [PMID 20525992]
- M. Aglietta M, C. Barone C, M. Muliello, C. Bagalà, D. Ferraro,
K. D. Fly, et al. A phase I dose escalation trial of CP-675206
(tremelimumab) in combination with gemcitabine in patients with
chemotherapy-naive metastatic pancreatic cancer. J Clin Oncol 2010;
28(15 Suppl):4134.
- Van Cutsem E, Vervenne W, Bennouna J Humblet Y, Gill S,
Van Laethem J, et al. Phase III trial of bevacizumab in combination
with gemcitabine and erlotinib in patients with metastatic pancreatic
cancer. J Clin Oncol 2009; 27:2231-7. [PMID 19307500]

