Keywords
Carcinoma; Pancreatectomy; Pancreatic Neoplasms; Pancreaticoduodenectomy
INTRODUCTION
The no-touch isolation technique was originally adopted as a strategy to protect cancer cells from spreading as a result of handling malignant tumors during colon and eye cancer surgery [1, 2]. Because a pancreatic tumor is generally often grasped by the surgeon prior to the ligation of surrounding vessels during pancreatectomy, squeezing and handling of the tumor could increase the risk of cancer cell shedding into the portal vein, retroperitoneum, and/or peritoneal cavity [3]. Hence, there is a potential benefit for using a no-touch approach in pancreatectomy as well [4, 5]. Although the concept of no-touch pancreatectomy has attracted some pancreatic surgeons, presumably because of complexity of the technique, such operation does not become popular yet.
Pancreatoduodenectomy (PD) is the only effective treatment for cancers of the pancreatic head region. Even for patients who have undergone curative resection (R0), survival analysis has revealed a poor survival rate because of cancer recurrence, although attempts to reduce the frequency of recurrence have resulted in numerous modifications in PD techniques [6-9]. Most postoperative recurrence is because of by hepatic metastasis, local recurrence, and peritoneal dissemination. Because surgeons usually grasp tumors during PD, this procedure may increase the risk of squeezing and shedding of the cancer cells into the portal vein, retroperitoneum, and/or peritoneal cavity. In an effort to overcome these problems, we have developed a surgical technique for improved en bloc dissection of the peripancreatic retroperitoneal margin without grasping tumors [3].
Whereas operable cancers of the pancreatic body and tail are less common than those of the pancreatic head, distal pancreatectomy (DP) is the only effective treatment for cancers of the pancreatic body and tail. DP has been the standard procedure for these cancers for decades. However, the recurrence rate after DP has remained high [10-14]. One of the possible factors for high recurrence rate may also be a squeezing out of cancer cells during the resection even in this case. In an effort to overcome this problem, we developed a no-touch surgical technique for DP as well. All drainage vessels are ligated during the early phase of the operation.
In this manuscript, outcome after no touch pancreatectomy in our hospital, including prognosis according to cancer stages, was reviewed.
MATERIAL AND METHODS
Patients
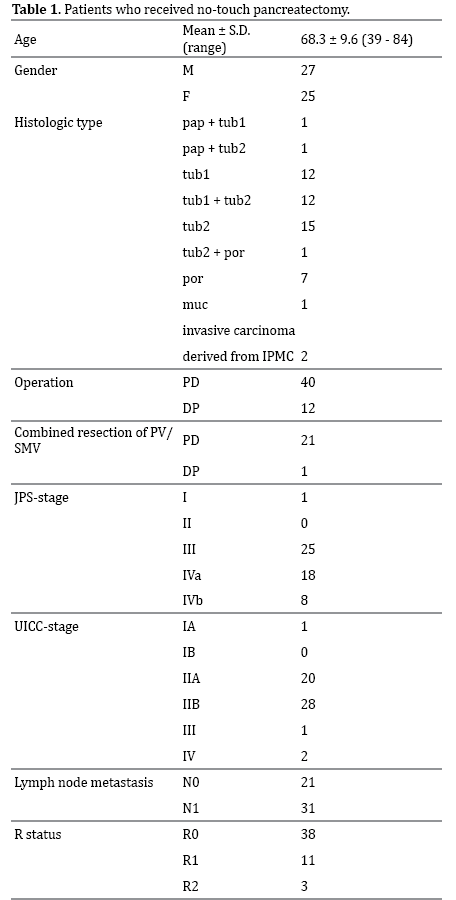
From April 2008 through September 2013, 52 pancreatic ductal adenocarcinoma patients have been operated on using this technique by a single operator (M. H. ). Patient characteristics were summarized in Table 1. Although we had started to perform no-touch pancreatectomy beforehand, the method of the operation was a little bit changed with the purpose of improvement and as a result of learning curve. Outcome of no-touch pancreatectomy after the top author (M. H. ) got a position at the current hospital (after April 2008) was summarized in the present manuscript. Among them, 40 received PD and 12 did DP. Combined resection of PV/SMV was performed in 22 patients (42%) (21 in PD, 1 in DP). Combined resections of left adrenal, left kidney, colon, stomach due to cancer invasion were in 3 (6%), 2 (4%), 5 (10%), 4 (8%), respectively. All patients were Japanese. In addition to those 52 patients, 10 patients received further advanced operations during the same period: DP-CAR (combined resection of celiac axis) 3; subtotal DP (combined resection of PV/SMV & bile duct) 3; total pancreatectomy (combined resection of PV/SMV) 1; extended paraaortic lymphadenectomy 3. Because it is rather difficult to pursue these advanced procedures using standard no-touch techniques, these patients are excluded from this analysis.
The consensus definition of borderline pancreatic cancer includes: 1. no distant metastases; 2. venous involvement of the superior mesenteric/portal vein demonstrating tumor abutment with impingement and narrowing of the lumen, encasement of the superior mesenteric/portal vein but without encasement of the nearby arteries, or short segment venous occlusion resulting from either tumor thrombus or encasement but with suitable vessel proximal and distal to the area of vessel involvement, allowing for safe resection and reconstruction; 3. gastroduodenal artery encasement up to the hepatic artery with either short segment encasement or direct abutment of the hepatic artery, without extension to the celiac axis; and 4. tumor abutment of the superior mesenteric artery not to exceed greater than 180 degrees of the circumference of the vessel wall [15, 16].
Surgical Technique
The detailed methods were previously described and published [4, 5]. The techniques are described briefly in this manuscript. This technique was devised by the top author (M. H. ) under direction by the last author (M. O. ).
PD
After transection of the pancreatic neck, all portal vein tributaries are ligated and divided individually until the SMV-PV is completely freed from the pancreatic head. If the tumor is approximated with or has invaded the SMV/PV, the involved SMV/PV is resected. This is usually performed with the help of an artificial bypass between the iliac vein and the femoral vein via saphenous vein using an antithrombogenic catheter [17]. The involved SMV/PV is later reconstructed without extreme concern for strict time limits [17]. Next, the anterior surface of the abdominal aorta, which corresponds to the posterior plane of Gerota fascia, is dissected from around the Treiz ligament towards a cranial direction along the right side of the origin of the superior mesenteric (SMA) and the celiac trunk arteries up to the crus of diaphragm. This plane is essentially avascular and easily dissectable. This procedure allows us two benefits; 1) efficient clearance of retroperitoneal margin between the SMA and aorta, and 2) steady wrapping of retroperitoneal margin with the Gerota fascia. The pancreatic side of the retroperitoneal margin is held using a long-nosed, right-angled DeBakey type aortic clamp (Figure 1a). Using rightward traction of the clamp, the peripancreatic retroperitoneal margin is transected along the right side surface of SMA, celiac artery, and the anterolateral surface of abdominal aorta. By this method, nervous and lymphatic tissue on the right and posterior aspects of the SMA is efficiently cleared. Step-by-step scooping of tissue along the SMA allows identification of the inferior pancreatoduodenal artery (Figure 1b) as well as the replaced right hepatic artery. To accomplish the notouch procedure safely in case of hepatic artery variant, it is important for surgeons to recognize its presence preoperatively using contrast enhanced CT. The tumor never serves as a “handle for retraction” of the specimen. The last procedure of the resection includes reversely directed Kocher maneuver. After the completion of “en bloc” PD, extensive peritoneal lavage was performed with 10 L of warm saline to remove any potential dissemination of cancer cells [18].
Figure 1. Clamping of the retroperitoneal margin. The pancreatic side of the retroperitoneal margin is held using a long-nosed, right-angled DeBakey type
aortic clamp (a). By rightward traction of the clamp, nervous and lymphatic tissue on the right and posterior aspects of the superior mesenteric artery
(SMA) is efficiently cleared. Step-by-step scooping of tissue along the SMA allows identification of the inferior pancreatoduodenal artery (IPDA)(b). The cut
line can be subjected to microscopic analysis by making a tissue slice along the clamp (c). PV: portal vein.
DP
Following the transection of the pancreatic neck, the splenic artery and vein are ligated and divided at the origin and at the confluence with the superior mesenteric vein, respectively. Splenocolic and gastrosplenic ligaments including short gastric and left gastroepiploic vessels are divided. At this point, all drainage vessels from the pancreatic body and tail have been divided. Retrosplenic Gerota fascia is transected on the surface of the left kidney. Then, the anterior surface of the abdominal aorta, which corresponds to plane posterior to the Gerota fascia, is exposed from around the ligament of Treiz toward a cranial direction up to the crus of diaphragm. The peripancreatic retroperitoneal tissue is clamped by a DeBakey type aortic clamp. Using leftward traction of the clamp, the peripancreatic retroperitoneal tissue (rightward resection margin) is transected along left surface of the SMA and celiac trunk and anterolateral surface of the abdominal aorta. The posterior plane of Gerota fascia is dissected from medial to lateral direction, allowing exposure of the left adrenal gland and vein, and left kidney and renal vessels [19, 20]. After the “en bloc” DP, extensive peritoneal lavage was performed with 10 L of warm saline to remove any potential dissemination of cancer cells [18].
Follow-up and Adjuvant Therapy
All patients visited the out-patient clinic every 2 or 4 weeks. Chest & abdominal enhanced CT is performed every 2-3 months. Tumor markers were measured every 1 month. As an adjuvant chemotherapy, patients were administered with biweekly intravenous gemcitabine at a dose of 800 mg/m2 for 9 months for the first 32 patients whose operation dates were before the end of 2012, or with S-1 orally (80, 100, or 120 mg/day according to bodysurface area on days 1 through 14 of a 21-day cycle) for one year for the rest 20 patients whose operation dates were after January 1st, 2013.
RESULTS
From April 2008 through September 2013, 52 patients (all with invasive ductal carcinoma) have been operated on following this technique. Twenty two cases (42%) required SMV-PV resection. As for the tumor stages in these patients, the final pathological stage classification (I/II/III/IVa/IVb) by the Japan Pancreas Society (JPS) was 1/0/25/18/8. The International Union against Cancer (UICC) pTNM stage classification (IA/IB/IIA/IIB/III/IV) was 1/0/20/28/1/2. Postoperative complications were as follows: 3 patients with grade B pancreatic fistula (6%), 2 with pneumonia (4%), 2 with peptic ulcer (4%), 1 with delayed gastric emptying (2%), 1 with liver abscess (2%), 1 with arrhythmia (2%), 1 with sepsis (2%), and 1 with skin infection (2%). The overall morbidity rate was 23%. Resected margins were microscopically analyzed. Among these, 38 were R0 (microscopically margin free), 11 were R1 (microscopically margin positive), and 3 was R2 (macroscopically margin positive) (73%, 21%, and 6%, respectively). R1 resection was defined as cancer cells within 1 mm of a circumferential or transaction margin, independent of the mode of cancer spread [21]. The mean number of lymph nodes examined was 22, and 31 patients (60%) had at least one positive node.
Overall 2- and 5-year survival rates were 64 and 42% with mean follow-up periods of 34. 4 months (range: 6-68 months). Recurrence free 2- and 5-year survival rates were 49 and 31%, respectively (Figure 2). The numbers of observations for 2 and 5 years were 33 and 10. Six patients were actual 5-year survivors.
Figure 2. Survival curves (Kaplan-Meier) after no-touch pancreatectomy. Solid and dotted lines represent overall survival and recurrence free survival
curves, respectively. Number at risk at 10, 20, 30, 40, 50, and 60 was shown.
The 5-year survival rates of patients received with PD and those did with DP were 44 and 35%, respectively. Figure 3 shows the survival rate acceding to JPS-stages. The 5-year survival rates of patients with JPS-stage Ⅲ and those with JPS-stage Ⅳ were 57 and 20%, respectively. Survival rates were also calculated according to UICC-stages. The 5-year survival rates of patients with UICC-stage Ⅱ A and those with UICC-stage Ⅱ B were 49 and 39%, respectively (Figure 4). Patients with UICC-stage Ⅲ or Ⅳ did not survive for more than 2 years.
Figure 3. Survival curves according to JPS-stages. Solid and dotted lines represent JPS-stage Ⅲ and JPS-stage Ⅳ (Ⅳa+Ⅳb), respectively. Number at risk at 10, 20, 30, 40, 50, and 60 was shown.
Figure 4. Survival curves according to UICC-stages. Solid black, dotted black, and solid gray lines represent UICC-stage ⅡA, UICC-stage ⅡB, and UICC-stage
Ⅲ+Ⅳ, respectively. Number at risk at 10, 20, 30, 40, 50, and 60 was shown.
The 5-year survival rates of patients with potentially resectable lesion and patients with borderline resectable lesion were 50% and 0%, respectively. Patients with borderline resectable lesion did not survive for more than 3 years. Survival rates were also calculated according to R status. The 5-year survival rates of patients with R0 and R1 were 53 and 17, respectively (Figure 5). Patients with R2 did not survive for more than 2 years.
Figure 5. Survival curves according to R status. Solid black, dotted black, and solid gray lines represent R0, R1, and R2, respectively. Number at risk at 10,
20, 30, 40, 50, and 60 was shown.
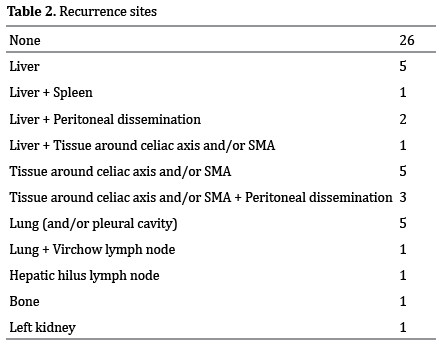
Recurrence was observed in 26 patients (50%) so far (Table 2). Frequent recurrence sites were the liver (9: 17%), tissue around celiac axis and/or SMA (9: 17%), and lung (6: 12%). Peritoneal dissemination was observed in 5 patients (10%).
DISCUSSION
We described a pancreatectomy involving a no-touch isolation technique. The aim of our method is to decrease the shedding of cancer cells, and to achieve negative transection margins. Pancreatic tumors are generally often grasped by surgeons before ligation of surrounding vessels during pancreatectomy. Squeezing and handling of the tumor prior to ligation of the surrounding vessels during pancreatectomy may increase the risk of cancer cell shedding into the portal vein, retroperitoneum and/ or peritoneal cavity. We found cancer cells in the droplets (exudate) from resected tissues [3] (Figure 6). Similarly, Ishikawa reported the presence of possibly viable cancer cells in the postoperatively drainaged fluid from the pancreatic bed [22]. Compared with other histopathologic parameters obtained from the resected specimens, the drain cytology was more specific in predicting the subsequent development of local recurrence [22]. Because our approaches also permit tumor resection without any grasping or squeezing, the technique has been named the “no-touch pancreatectomy. ” All drainage veins from the pancreas have been ligated and divided during the early phase of the no-touch pancreatectomy. During the procedure, the pancreatic tumor is neither grasped nor squeezed by the surgeon.
Figure 6. Cancer cell containing droplet from resected tissues. Arrow
shows the droplet from the resected tissue including cancer lesion. The
droplet (exudate) contains cancer cells (inset).
Another aim is to resect cancers by wrapping them within Gerota fascia. In severe acute pancreatitis, autodigestion of peripancreatic tissue by pancreatic proteases is generally provoked, whereas perirenal tissue beyond the Gerota fascia is often protected from the autodigestion [23]. Because cancer cell invasion is also dependent on protease activity produced by it, Gerota fascia may function as a barrier against protease-mediated invasion of cancer cells as in the blockage of perirenal tissue during acute pancreatitis.
A hanging and clamping maneuver of the peripancreatic retroperitoneal tissues allows not only proper clearance of tissue along SMA, celiac artery and abdominal aorta, but also easier dissection of the plane posterior to the Gerota fascia. Another aim of hanging and clamping maneuver was to facilitate negative resection margins. A majority of studies confirm the importance of R0 resection for pancreatic head cancers [24, 25], which may only be accomplished by techniques moving the dissecting line further away from the tumor [25, 26]. Even for pancreatic body and tail cancers, the importance of R0 resection is also applicable [21, 27]. By traction of the clamp on the peripancreatic retroperitoneal tissue may improve the clearance of the nervous and lymphatic tissues along the SMA and celiac artery. The traction procedure and dissection of the posterior plane of Gerota fascia increase the possibility to perform R0 resection of pancreatic adenocarcinoma.
R0 even in our no-touch operation is not a true R0. Some cancer cells may be concealed somewhere. For such false R0, there are two possibilities; 1) a minute residual cancer foci might be left behind close to the cut lines, 2) some cancer cells might be exfoliated into lymphatic or vascular vessels, and/or abdominal cavity during pancreatectomy procedure. Even with no-touch pancreatectomy technique, we cannot reduce the residual or exfoliated cancer cells to nil completely. In such false R0 cases, we have to think about recurrence.
Because the performance of recent CT is excellent, we can judge whether the invasion extends beyond the “point of no return” or not preoperatively in most cases. However, preand intra-operative discrimination between inflammatory change and cancer invasion is difficult. Mostly microscopic evaluation is necessary for it. In some cases, surgeons may have to re-evaluate the local extension of the cancer during operation before going beyond the “point of no return” with resection [28]. Actually, 3 cases (6%) resulted in R2 operation in our series. They did not survive for more than 2 years. Surgeons operating pancreatic cancer should not stay focused on the planned approach, if the local reality requires. Future improvement in preoperative evaluation of the local extension of the cancer is eagerly awaited by pancreatic surgeons.
Conventionally the pancreatic tissue containing cancer is grasped by surgeons before the dissection of the drainage vessels as shown in Figure 1 of ref. 3. During the procedure minute cancer cells are exfoliated and are scattered as shown in Figure 6. Overall 5-year survival rate of our historical standard technique cohort was 13% [3]. On the other hand, 5-year survival rates in this series were as following; overall: 42%, recurrence free: 31%, JPS-stage III: 57%, UICC-stage IIA: 49%, and UICC-stage IIB: 39%. In conclusion, the “no-touch” pancreatectomy procedure using the hanging and clamping maneuver for peripancreatic retroperitoneal margin resection has many theoretic advantages that merit further investigation in future randomized controlled trials.
Conflict of Interest
The authors declare that there is no conflict of interest.
References
- Barnes JP. Physiologic resection of the right colon. Surg Gynecol Obstet. 1952; 94(6):722-6. [PMID:14931182]
- Turnbull RB Jr, Kyle K, Watson FR, Spratt J. Cancer of the colon: the influence of the no-touch isolation technique on survival rates. Ann Surg. 1967; 166:420-427. [PMID:6039601]
- Hirota M, Shimada S, Yamamoto K, Tanaka E, Sugita H, Egami H, Ogawa M. Pancreatectomy using the no-touch isolation technique followed by extensive intraoperative peritoneal lavage to prevent cancer cell dissemination: a pilot study. JOP. 2005; 6:143-151. [PMID:15767730]
- Hirota M, Kanemitsu K, Takamori H, Chikamoto A, Tanaka H, Sugita H, Sand J, et al. Pancreatoduodenectomy using a no-touch isolation technique. Am J Surg. 2010; 199:e65-e68. [PMID:19095210]
- Hirota M, Hashimoto D, Ishiko T, Satoh N, Takamori H, Chikamoto A, Tanaka H, et al. Distal pancreatectomy using a no-touch isolation technique. Scand J Surg. 2012; 101:156-159. [PMID:22968237]
- Fortner JG, Kim DK, Cubilla A, Turnbull A, Pahnke LD, Shils ME. Regional pancreatectomy: en bloc pancreatic, portal vein and lymph node resection. Ann Surg. 1977; 186:42-50. [PMID:195543]
- Yeo CJ, Cameron JL, Sohn TA, Coleman J, Sauter PK, Hruban RH, Pitt HA, et al. Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparison of morbidity and mortality and short-term outcome. Ann Surg. 1999; 229:613-622. [PMID:10235519]
- Weitz J, Kienle P, Schmidt J, Friess H, Büchler MW. Portal vein resection for advanced pancreatichead cancer. J Am Coll Surg. 2007; 204:712-716. [PMID:17382233]
- Mizuno S, Isaji S, Tanemura A, et al. Anterior approach to the superior mesenteric artery by using nerve plexus hanging maneuver for borderline resectable pancreatic head carcinoma. J Gastrointest Surg 2014 Mar 25. [Epub ahead of print]
- Shoup M, Conlon KC, Klimstra D, Brennan ME. Is extended resection for adenocarcinoma of the body or tail of the pancreas justified? J Gastrointest Surg. 2003; 240: 214-215. [PMID:14675703]
- Christein JD, Kendrick ML, Iqbal CW, Nagorney DM, Farnell MB. Distal pancreatectomy for respectable adenocarcinoma of the body and tail of the pancreas. J Gastrointest Surg. 2005; 9:922-927. [PMID:16137585]
- Shimada K, Sakamoto Y, Sano T, Kosuge T. Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery. 2006; 139:288- 295. [PMID:16546491]
- Murakami Y, Uemura K, Sudo T, Hayashidani Y, Hashimoto Y, Ohge H, Sueda T. Impact of adjuvant gemcitabine plus S-1 chemotherapy after surgical resection for adenocarcinoma of the body or tail of the pancreas. J Gastrointest Surg. 2009; 13:85-92. [PMID:18704593]
- Fujita T, Nakagohri T, Gotohda N, Takahashi S, Konishi M, Kojima M, Kinoshita T. Evaluation of the prognostic factors and significance of lymph node status in invasive ductal carcinoma of the body or tail of the pancreas. Pancreas. 2010; 39:e48-54. [PMID:19910836]
- Callery MP, Chang KJ, Fishman EK, Talamonti MS, William Traverso L, Linehan DC. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol. 2009; 16:1727-1733. [PMID:19396496]
- Springett GM, Hoffe SE. Borderline resectable pancreatic cancer: on the edge of survival. Cancer Control. 2008; 15:295-307. [PMID:18813197]
- Nakao A, Takagi H. Isolated pancreatectomy for pancreatic head carcinoma using catheter bypass of the portal vein. Hepatogastroenterology. 1993; 40:426-429. [PMID:8270230]
- Yamamoto K, Shimada S, Hirota M, Yagi Y, Matsuda M, Baba H. EIPL (extensive intraoperative peritoneal lavage) therapy significantly reduces peritoneal recurrence after pancreatectomy in patients with pancreatic cancer. Int J Oncol. 2005; 27:1321-1328. [PMID:16211228]
- Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular pancreatosplenectomy. Surgery. 2003; 133:521-527. [PMID:12773980]
- Strasberg SM, Linehan DC, Hawkins WG. Radical antegrade modular pancreatosplenectomy procedure for adenocarcinoma of the body and tail of the pancreas: ability of obtain negative tangential margins. J Am Coll Surg. 2007; 204:244-249. [PMID:17254928]
- Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A. Redifining the R1 resection in pancreatic cancer. Br J Surg. 2006; 93:1232- 1237. [PMID:16804874]
- Ishikawa O, Wada H, Ohigashi H, Doki Y, Yokoyama S, Noura S, Yamada T, et al. Postoperative cytology for drained fluid from the pancreatic bed after “curative “ resection of pancreatic cancers: does it predict both the patient’s prognosis and the site of cancer recurrence? Ann Surg. 2003; 238:103-110. [PMID:12832972]
- Imamura Y, Hirota M, Ida S, Hayashi N, Watanabe M, Takamori H, Awai K, et al. Significance of renal rim grade on computed tomography in severity evaluation of acute pancreatitis. Pancreas. 2010; 39:41-46. [PMID:19745776]
- Weitz J, Kienle P, Schmidt J, Friess H, Büchler MW. Portal vein resection for advanced pancreatic head cancer. J Am Coll Surg. 2007; 204:712-716. [PMID:17382233]
- Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Büchler MW. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg. 2004; 91:586-594. [PMID:15122610]
- Hartel M, Wente MN, Di Sebastiano P, Friess H, Büchler MW. The role of extended resection in pancreatic adenocarcinoma: is there good evidence-based justification? Pancreatology. 2004; 4:561-566. [PMID:15550765]
- Howard TJ, Krug JE, Yu J, Zyromski NJ, Schmidt CM, Jacobson LE, Madura JA, et al. A margin-negative R0 resection accomplished with minimal postoperative complications is the surgeon’s contribution to long-term survival in pancreatic cancer. J Gastrointest Surg. 2006; 10:1338-1346. [PMID:17175452]
- Dumitrascu T, David L, Popescu I. Posterior versus standard approach in pancreatoduodenectomy: a case-match study. Langenbecks Arch Surg. 2010; 395: 677-84.







