Keywords
Pancreas; Pancreatic Fistula
Abbreviations
CR Clinically relavent; LP Left sided pancreatectomy;
PD pancreaticoduodenectomy; PF Pancreatic fistula; PPH postpancreatectomy
hemorrhage; PR Pancreatic resections
INTRODUCTION
The association between hospital procedure volume
and their surgical outcomes has been a medical and social
concerns. This volume-outcome relationship has been
studied extensively, and considerable evidence seems to
support it for a variety of surgical procedures [1, 2, 3, 4, 5, 6].
Pancreatic resections (PR) are complex and associated
with a high risk of complications. Birkmeyer et al. reported
that mortality of pancreatoduodenectomy (PD) in lowvolume
(LV) hospitals can be three- to four-fold greater
than in high-volume (HV) hospitals [1]. Hospitals with a
HV of pancreatectomies have been shown to have better
post-operative outcomes than LV hospitals [7, 8, 9, 10, 11]. Therefore, there is growing trend toward referral of
patients to HV hospitals [12]. Moreover, a new legislative
reform was introduced defining a threshold of pancreatic
resections in Germany [13]. The National Cancer Policy
Board of USA has recommended selective referral to
HV centers for pancreatectomy, this procedures with
the strongest volume-mortality relationships [14].
Both hospital and surgeon procedure volume predicted
mortality [15].
However, PR previously reserved for severe
complication and carried a high mortality, has evolved
into a common and safe procedure performed by many
surgeons today. Major PR can be performed safely at
community hospitals [16]. This study was undertaken to
investigate outcome of PR in a LV hospital through short
term surgical results.
PATIENTS AND METHODS
Between March 2012 and June 2016, 68 patients
underwent PR at Yeouido St. Mary’s Hospital in Seoul,
Korea. Among them, 8 patients were excluded who
underwent unplanned and planned PR by Gastrointestinal
surgeon during same periods. Consecutive 59 patients
underwent PR for pancreatic disease by single HBP
Surgeon (KY.P), including periampullary malignancy and
various pancreatic diseases at a LV hospital.
PD was performed using conventional type or
pylorus-preserving. Almost of pancreaticoenterostomy
was pancreaticojejunostomy with external pancreatic
stent drainage. When jejunal diameter was smaller than
pancreas stump thickness, pancreaticogastrostomy was
selected instead of pancreaticojejunostomy. Left sided
pancreatectomy (LP) included distal pancreatectomy or
subtotal pancreatectomy which was defined as pancreas
stump was located at porto-splenic vein junction
level. In case of pancreatic ductal adenocarcinoma
(PDAC), we performed radical antegrade modular
pancreaticosplenectomy [17]. When tumor was suspected
to benign, LP was performed under laparoscopic approach
with or without splenectomy. Total pancreatectomy
(TP) was performed when entire pancreas was involved
pathology or pancreas neck margin revealed existence
of PDAC cell on frozen biopsy during pancreatectomy.
Central pancreatectomy (CP) was performed when benign
tumor was located on neck or body area and distal remnant
pancreas was inserted into stomach body.
We retrospectively analyze the demographics,
resection types, pathologic diagnosis, and clinical outcome
including the postoperative complication. We analyzed PD
group including 2 patients with CP because of existence of
pancreaticoenterostomy.
All patients received octreotide routinely given
subcutaneously (100 μg every 8 hour for 7 days).
The volume of fluid drained from the peripancreatic
drains and that drained from the pancreatic duct were
measured daily, and serum and drain fluid amylase
levels were measured on postoperative days 1, 3, 5,
and 7. A computed tomography scan was performed
on postoperative day 7, and if there was no evidence
of leakage or fluid collection, the peripancreatic drains
were removed.
Postoperative outcomes were followed until 90 days
after surgery and were graded according to the Clavien-
Dindo system [18]. A final overall patient complication
grade was given to the highest-rated complication
grade experienced by patients. Clinically relavent (CR)
complications were defined as grade III-V complications.
Post-operative pancreatic fstula (POPF) [19] and postpanceatectomy
hemorrhage (PPH) [20] were scored and
graded according to standard international consensus
definitions. Clinical relavent (CR) PF was defined grade
B or C. Delayed gastric emptying (DGE) was defined as
the need for nasogastric decompression beyond the 10th
postoperative days. Length of stay (LOS) was recorded
and was defined as postoperative day 1 through day of
discharge. Surgical site infection (SSI), intra abdominal
abscess and pneumonia were included postoperative
complication in this study. Readmission to any hospital
was defined as any unplanned admission and was tracked
for all patients through 90 days after surgery. Reoperation
was defined as any unplanned operation within 90 days of
the primary pancreatic resection.
All results are presented as mean (range). Statistical
analyses were performed with SPSS for Windows, version
16.0 (SPSS Inc, Chicago, Illinois). Univariate analyses were
conducted with T-test, Mann-Whitney, chi-square tests
as appropriate. All tests were 2 sided, and P<0.05 was
considered statistically significant.
RESULTS
Patients
During the 51-months study period, a total of 59
patients underwent a formal pancreatic resection by the
single surgeon included in this study. There were 29 PD, 22
LP, 6 TP, and 2 CP. The most common diagnosis prompting
an operation was periampullary carcinoma excluding
PDAC (n=22, 37.3%), followed by PDAC comprising 30.5%
(n=18), cystic neoplasms (including intraductal papillary
mucinous neoplasm; mucinous cystic neoplasm; serous
cystadenoma; and solid pseudopapillary neoplasm)
comprising 20.3% (n=12) and pancreatic neuroendocrine
tumors comprising 11.9% (n=7).
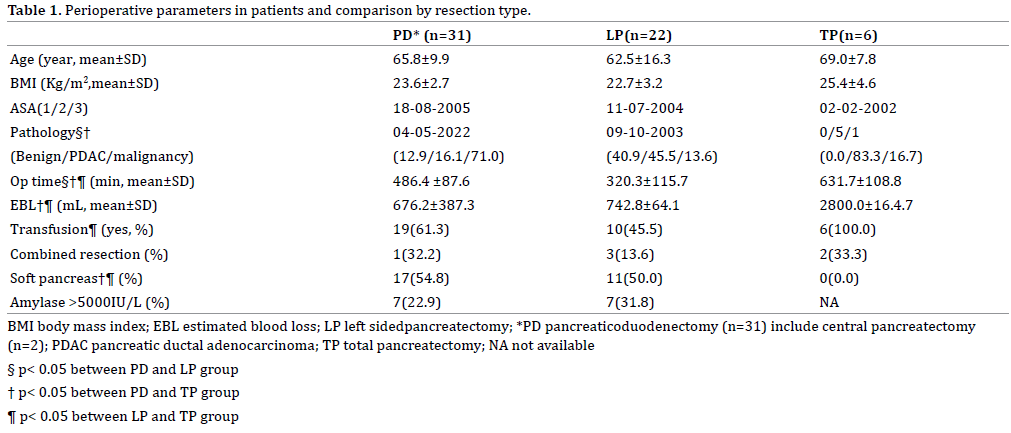
Clinical Parameters According to Resection Type
There were no differences of age, body mass index,
and American association of Anesthesiology risk among
three resection types. Most of pathology for PD was
periampullary neoplasm. 40.9% of LP (n=9) was performed
for benign pancreas neoplasm and 45.5% (n=10) of LP was
for PDAC. Almost of TP (83.3%, n=5) was performed for
PDAC. Operation time was significantly longer in PD and
TP than LP and TP was most time- consuming procedure
among three groups (mean 631 minute). There were
no differences of rate of transfusion, rate of combined
adjacent organ resection, proportion of soft pancreas and
above 5000IU/ml of drain amylase level on post-operative
one day among three groups. Above results were described
in Table 1.
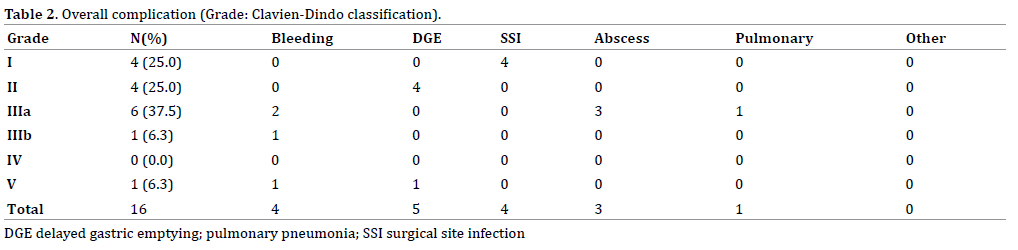
Postoperative Complication
There was one in hospital mortality (1.67%) due to
PPH derived from gastroduodenal artery pseudoaneurysm
caused by POPF. Mortality case was 78-year old man
who had diagnosed mid CBD cancer and underwent PD.
Clavien-Dindo grade I complication contained 4 surgical
site infection and grade II complication were 4 DGE. CRcomplication
rate was 13.3% (n=8) including 5 PPH (2
pseudoaneurysm, 2 gastric ulcer bleeding, and 1 omental
bleeding), 3 abscess, 1 pulmonary effusion (Table 2).
There were no significant differences in CR-complication
rates (20.7% vs. 4.5%, vs. 16.7% p=0.37) according to
operation type (PD vs. LP vs. TP).
Postoperative Pancreatic Fistula
Grade A POPF was observed 11 (35.5%) patients who
underwent PD and to 11 (50.0%) patients underwent
LP. Overall CR-POPF rate was 6.6% (n=4) including 3
occurrences in PD and one in LP (RAMPS). However, there
was no significant differences of CR-POPF between resection
type (PD vs. LP= 9.7% vs. 4.5% p=0.49) (Table 3).
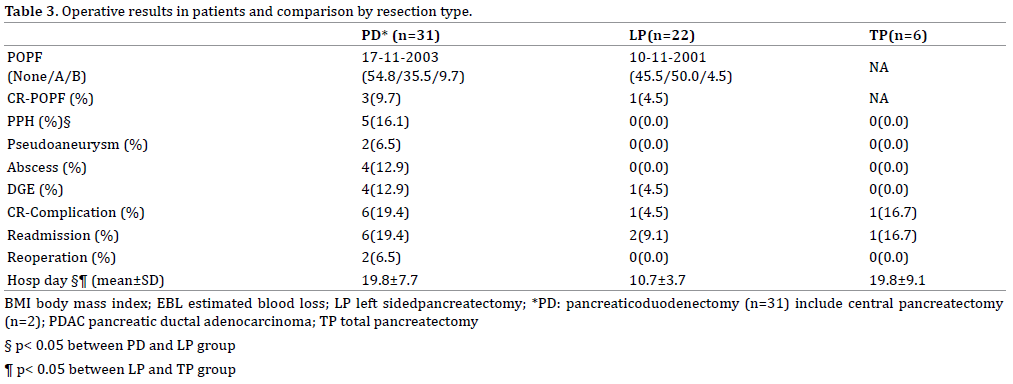
Readmission and reoperation
8 patients (13.3%) were hospitalized again after index
discharge. The cause of readmission was 4 poor oral
intakes, 1 poor glucose control, 1 hematemesis, and 2
ileus. Two patients (3.3%) had to undergo surgery again
due to intra-abdominal PPH. One patient underwent
relaparotomy owing to omental bleeding which was
easily controlled by bleeder ligation. Another patient was
mentioned above paragraph and he expired 10 days after
relaparotomy due to multi-organ failure. Reoperation
rates of PD was 6.9% (n=2) and there was no reoperation
after LP and TP (p=0.64).
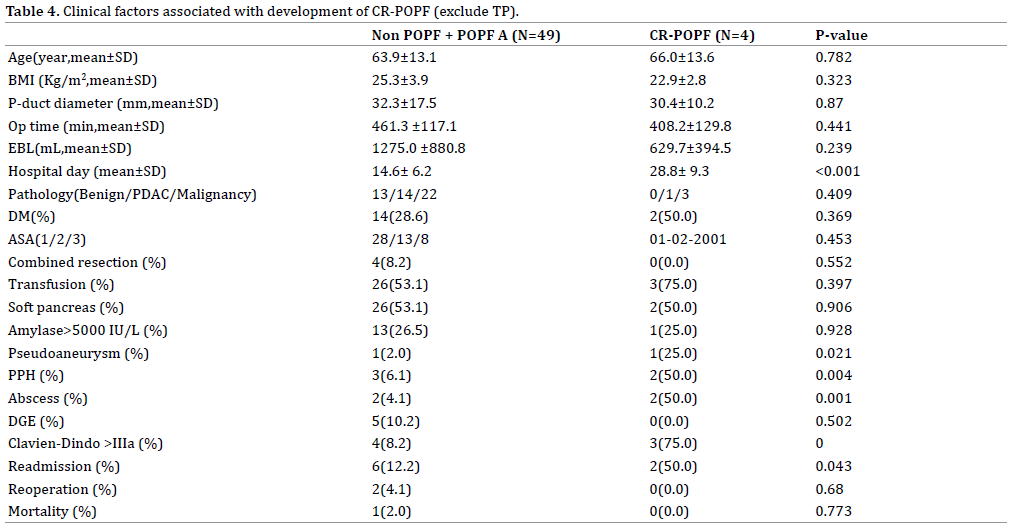
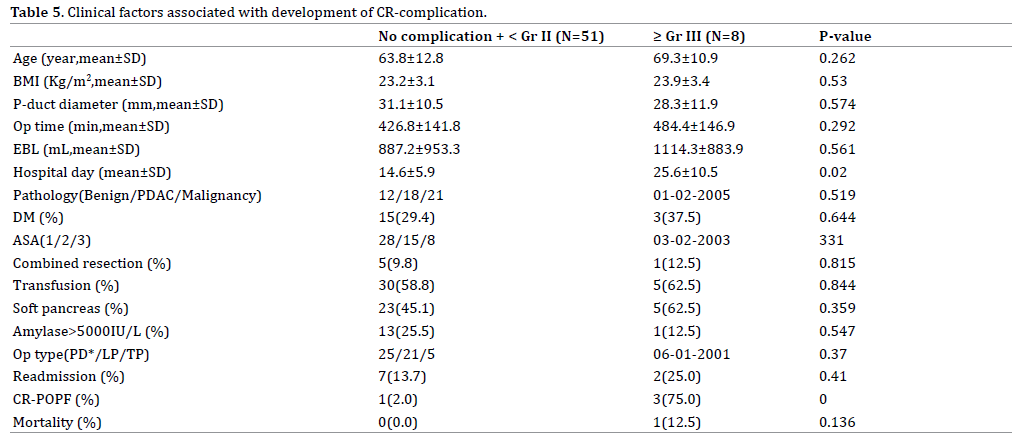
Clinical factors associated with development of CRPOPF
and CR-complication
CR-POPF was associated with CR-complication
(p<0.001), pseudoaneurysm (p=0.021), PPH (P=0.04),
intra-abdominal abscess (p=0.001), and readmission
(p=0.043) (Table 4). CR-complication was associated with
CR-POPF and longer LOS (P<0.001) (Table 5).
DISCUSSION
The aim of the present study was to investigate the
result of PR at a LV institution. To accomplish this aim,
we evaluated short term surgical result of all type of PR using various parameters. Despite of lower number of
entire PR, our results demonstrate that morbidity and
mortality were comparable those of previous HV centers
in literatures. Our 90-day hospital mortality was 1.67%,
surgical complication above Clavien-Dindo IIIa rate was
13.3%, 3.3 % reoperation rate and overall CR-POPF rate
was 6.6%.
In general, surgical outcome of PR had been focused
on large volume centers. It means PR result of LV center
overlooked so far. Although it was single center and single
surgeon experience for PR observed short term period, it
is shed light on result of PR at a LV institution. There was
only one study regarding PR in LV center with rough data
[16].
In terms of PD, evidence showing better outcomes in
HV centers was well established. Recent systemic analysis
[12] demonstrated strong evidence for inverse association
between higher hospital volume and lower mortality after
PD. In contrast, Schell et al. [21] showed that LV hospitals
were able to obtain results comparable to those of HV
providers if expertise and care pathways were imported.
Investigation based on nationwide administrative
data reported that hospital procedure volume is not a
significant predictor of mortality for the performance of
PR [22]. Pawlik et al. [15] revealed the analysis supporting
HV expertise in one area of hepatobiliary and pancreas
surgery does not translate into improved outcomes for
related procedures.
Two decades ago, there was initial consensus regarding
hospital experience is particularly important with PD,
and patients considering this procedure should be given
the option of care at a HV referral center [1]. Recent two studies performed by Japanese and Swedish groups
insisted of evidence regarding centralization of PD in a
national healthcare system [23, 24]. Equally, participation
in regional quality collaboratives by LV hospitals can
attenuate the volume outcome relationship for pancreatic
surgery. Continued work in collaboratives with an
emphasis on technical and intraoperative aspects of care
may improve overall quality of care [25].
However, the optimal cutoff values for defining HV
hospital are currently under debate [12]. The Leapfrog
Group volume originally proposed cutoffs 11 PD per year
[26]. Previously published definitions of HV hospitals
showed ranging from 10 to 80 PD/year, with the majority
using a definition between 10 and 30 PD/year [27, 28, 29]. Systematic review suggested that variations in HV
cutoff values across studies majorly influenced the overall
heterogeneity of results. Accordingly, criteria for PR
volume might be debatable yet on the bases of previous
literatures [12].
Our hospital has been teaching and academic
University Hospital and average annual volume of PR has
been ten to twenty since 2000 steadily. In this study, PR
was performed by single surgeon who was trained in HV
center performing annual PR might be over 200. After twoyear
fellowship training, he worked at community hospital
its average PR volume was under 10 yearly during three
years and then moved to this University Hospital.
We believe that lower rate of CR-POPF in this study
was up to tailored pancreaticoenterostomy according
to risk for it. In previous study, we showed very lower
rate of POPF following external drainage with modified
pancreaticojejunostomy [30]. Also we performed
pancreaticogastrostomy if pancreas texture was soft and
pancreatic duct under 2 mm. With regard to LP, stump
closure method has changed using thickest stapler since
2013 under laparoscopy to reduce POPF and kept closing
the main duct and to reinforce whole stump during open
surgery.
However, inherent limitation of very short period of
study, we believe that the prolonged study period allows
us to accurately ascertain the accurate result of ours
through this method.
Recently, concern for improving surgical quality
focused on “failure to rescue” which means mortality
following complication [31]. Most previous research in
understanding volume-mortality relationships has focused
on the occurrence of complications [32, 33]. Differences in
mortality between HV and LV hospitals are not associated
with large differences in complication rates. Instead, these
differences seem to be associated with the ability of a
hospital to effectively rescue patients from complications.
Strategies focusing on the timely recognition and
management of complications once they occur may be
essential to improve outcomes at LV hospitals [31]. We
totally agree with this concept concerning a mortality case
in this study depended on insufficient management of PPH in intensive care unit, inappropriate patient selection and
multidisciplinary approach was lack.
Pawlik et al. [34] emphasized that improvement of
mortality in LV hospital after PR seems to be related
to a decreased FTR according to nationwide database.
Accordingly, we will try to do best to improve FTR in future
even in a LV hospital.
Interestingly, recent researches dealt with surgeon
factor for PR. Schmidt et al. [35] demonstrated experienced
surgeons had comparable outcomes irrespective of annual
volume. Toomy et al. [36] reported that salutary benefits
of undertaking PD at a HV hospital are transferred to
a LV hospital when HV surgeons relocate and the "best"
results follow HV surgeons. Surgeon in this study was
trained at a HV institute performing PR over 200 per year
and transferred to LV hospital. Italian study suggested
that the surgeon experience together with selection
of patients, team experience of LV hospital may be
important factor for overcoming volume effect [37]. This
point is very important to improve the short outcome
of PR at a LV hospital, as we mentioned above reflecting
our mortality case. Furthermore, sharing of operative
techniques and perioperative care pathways, which has
enabled the LV hospitals to develop a health care delivery
system that resembles the large-volume hospital and
achieves comparable results [22]. To improve and acquire
acceptable result of PR, LV institution should make every
effort that all above mentioned.
The limitation of the study is the short period of
observation and the low number of case. From a clinical
point of view, the manuscript would achieve more
relevance if multiple low-volume centers were included.
In addition, oncologic outcome measurements should
include 5-year and disease-free survival at a LV hospitals
in next study.
CONCLUSION
PR can be achieved at a LV hospital with good results,
but longer and more observation will be needed for
acceptable.
Conflict of Interest
None of the authors have any conflict of interest to
disclose related to this article.
References
- Birkmeyer JD, Finlayson SR, Tosteson AN, Sharp SM, Warshaw
AL, Fisher ES. Effect of hospital volume on in-hospital mortality with
pancreaticoduodenectomy. Surgery 1999; 125:250-6. [PMID: 10076608]
- Kohn GP, Galanko JA, Meyers MO, Feins RH, Farrell TM. National
trends in esophageal surgery--are outcomes as good as we believe? J
Gastrointest Surg 2009; 13:1900-10; discussion 10-2. [PMID: 19760305]
- Birkmeyer JD, Dimick JB, Staiger DO. Operative mortality and
procedure volume as predictors of subsequent hospital performance.
Ann Surg 2006; 243:411-7. [PMID: 16495708]
- Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista
I, et al. Hospital volume and surgical mortality in the United States. N Engl
J Med 2002; 346:1128-37. [PMID: 11948273]
- Birkmeyer JD, Sun Y, Goldfaden A, Birkmeyer NJ, Stukel TA. Volume
and process of care in high-risk cancer surgery. Cancer 2006; 106:2476-
81. [PMID: 16634089]
- Learn PA, Bach PB. A decade of mortality reductions in major
oncologic surgery:the impact of centralization and quality improvement.
Med Care 2010; 48:1041-9. [PMID: 20966781]
- Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Relation of
perioperative deaths to hospital volume among patients undergoing
pancreatic resection for malignancy. Ann Surg 1995; 222:638-45.
[PMID: 7487211]
- Janes RH Jr, Niederhuber JE, Chmiel JS, Winchester DP, Ocwieja KC,
Karnell JH, et al. National patterns of care for pancreatic cancer. Results
of a survey by the Commission on Cancer. Ann Surg 1996; 223:261-72.
[PMID: 8604906]
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital
volume on operative mortality for major cancer surgery. JAMA 1998;
280:1747-51. [PMID: 9842949]
- Kotwall CA, Maxwell JG, Brinker CC, Koch GG, Covington DL. National
estimates of mortality rates for radical pancreaticoduodenectomy in
25,000 patients. Ann Surg Oncol 2002; 9:847-54. [PMID: 12417505]
- Evans DB, Tsai S. Volume-outcome in cancer surgery: why has the
data not affected policy change? Ann Surg Oncol 2014; 21:4056-8.
[PMID: 25239003]
- ReferenceHata T, Motoi F, Ishida M, Naitoh T, Katayose Y, Egawa S, et al. Effect of
Hospital Volume on Surgical Outcomes After Pancreaticoduodenectomy:
A Systematic Review and Meta-analysis. Ann Surg 2016; 263:664-72.
[PMID: 26636243]
- Alsfasser G, Kittner J, Eisold S, Klar E. Volume-outcome relationship
in pancreatic surgery: the situation in Germany. Surgery 2012; 152:S50-
5. [PMID: 22763260]
- Hewitt ME, Petitti DB, National Cancer Policy B, National Research C,
Division on E, Life S. Interpreting the volume-outcome relationship in the
context of cancer care. Washington, D.C.:National Academy Press, 2001.
- Nathan H, Cameron JL, Choti MA, Schulick RD, Pawlik TM. The
volume-outcomes effect in hepato-pancreato-biliary surgery: hospital
versus surgeon contributions and specificity of the relationship. J Am Coll
Surg 2009; 208:528-38. [PMID: 19476786]
- Cunningham JD, O'Donnell N, Starker P. Surgical outcomes following
pancreatic resection at a low-volume community hospital:do all patients
need to be sent to a regional cancer center? Am J Surg 2009; 198:227-30.
[PMID: 19306974]
- Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular
pancreatosplenectomy. Surgery 2003; 133:521-7. [PMID: 12773980]
- Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick
RD, et al. The Clavien-Dindo classification of surgical complications: fiveyear
experience. Ann Surg 2009; 250:187-96. [PMID: 19638912]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al.
Postoperative pancreatic fistula:an international study group (ISGPF)
definition. Surgery 2005; 138:8-13. [PMID: 16003309]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ,
et al. Postpancreatectomy hemorrhage (PPH):an International Study
Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20-5.
[PMID: 17629996]
- Schell MT, Barcia A, Spitzer AL, Harris HW. Pancreaticoduodenectomy:
volume is not associated with outcome within an academic health care
system. HPB Surg 2008; 2008:825940. [PMID: 18475317]
- LaPar DJ, Kron IL, Jones DR, Stukenborg GJ, Kozower BD. Hospital
procedure volume should not be used as a measure of surgical quality.
Ann Surg 2012; 256:606-15. [PMID: 22964735]
- Yoshioka R, Yasunaga H, Hasegawa K, Horiguchi H, Fushimi K, Aoki T,
et al. Impact of hospital volume on hospital mortality, length of stay and
total costs after pancreaticoduodenectomy. Br J Surg 2014; 101:523-9.
[PMID: 24615349]
- Ansari D, Williamsson C, Tingstedt B, Andersson B, Lindell G, Andersson
R. Pancreaticoduodenectomy-the transition from a low- to a high-volume
center. Scand J Gastroenterol 2014; 49:481-4. [PMID: 24255988]
- Healy MA, Krell RW, Abdelsattar ZM, McCahill LE, Kwon D, Frankel TL,
et al. Pancreatic Resection Results in a Statewide Surgical Collaborative.
Ann Surg Oncol 2015; 22:2468-74. [PMID: 25820999]
- Healy MA, Krell RW, Abdelsattar ZM, McCahill LE, Kwon D, Frankel TL,
et al. Pancreatic Resection Results in a Statewide Surgical Collaborative.
Ann Surg Oncol 2015; 22:2468-74. [PMID: 25820999]
- Marcaccio M, Langer B, Rumble B, Hunter A, Expert Panel on HPB
Surgical Oncology. Hepatic, pancreatic, and biliary tract (HPB) surgical
oncology standards. Progream in evidence-based care. Toronto,
ON:Cancer Care Ontario; 2006.
- Nordback L, Parviainen M, Raty S, Kuivanen H, Sand J. Resection of
the head of the pancreas in Finland: effects of hospital and surgeon on
short-term and long-term results. Scand J Gastroenterol 2002; 37:1454-
60. [PMID: 12523597]
- Pal N, Axisa B, Yusof S, Newcombe RG, Wemyss-Holden S, Rhodes
M, et al. Volume and outcome for major upper GI surgery in England. J
Gastrointest Surg 2008; 12:353-7. [PMID: 17805936]
- Kim DJ, Paik KY, Kim W, Kim EK. The effect of modified
pancreaticojejunostomy for reducing the pancreatic fistula after
pancreaticoduodenectomy. Hepatogastroenterology 2014; 61:1421-5.
[PMID: 25436320]
- Ghaferi AA, Birkmeyer JD, Dimick JB. Hospital volume and
failure to rescue with high-risk surgery. Med Care 2011; 49:1076-81.
[PMID: 22002649]
- Finks JF, Osborne NH, Birkmeyer JD. Trends in hospital volume and
operative mortality for high-risk surgery. N Engl J Med 2011; 364:2128-
37. [PMID: 21631325]
- Hollenbeck BK, Daignault S, Dunn RL, Gilbert S, Weizer AZ, Miller DC.
Getting under the hood of the volume-outcome relationship for radical
cystectomy. J Urol 2007; 177:2095-9; discussion 9. [PMID: 17509295]
- Amini N, Spolverato G, Kim Y, Pawlik TM. Trends in Hospital Volume
and Failure to Rescue for Pancreatic Surgery. J Gastrointest Surg 2015;
19:1581-92. [PMID: 25794484]
- Schmidt CM, Turrini O, Parikh P, House MG, Zyromski NJ, Nakeeb A,
et al. Effect of hospital volume, surgeon experience, and surgeon volume
on patient outcomes after pancreaticoduodenectomy:a single-institution
experience. Arch Surg 2010; 145:634-40. [PMID: 20644125]
- Toomey PG, Teta AF, Patel KD, Ross SB, Rosemurgy AS. High-volume
surgeons vs high-volume hospitals:are best outcomes more due to who or
where? Am J Surg 2016; 211:59-63. [PMID: 26542187]
- Stella M, Bissolati M, Gentile D, Arriciati A. Impact of surgical
experience on management and outcome of pancreatic surgery performed
in high- and low-volume centers. Updates Surg 2017. [PMID: 28215039]

