Keywords
dasatinib; Carcinoma, Pancreatic Ductal Tumor Necrosis Factor-alpha
Abbreviations
SBRT: stereotactic body radiotherapy
INTRODUCTION
Pancreatic adenocarcinoma is one of the most aggressive malignant tumors. Despite the available treatment options, it remains the fourth leading cause of cancer-related death. The only potentially curative treatment is surgical resection. Unfortunately, only 15- 20% of patients have resectable disease at initial diagnosis. About half of the patients with unresectable tumors have locally advanced disease with no evidence of metastasis. In the United States, most of the patients with locally advanced disease are treated with chemoradiation. The most commonly used chemotherapy is either fluorouracil (5-FU)-based or gemcitabine-based regimens [1]. However, accumulating data suggest that the impact of gemcitabine-based chemotherapy on survival may be of approximately the same magnitude as that achieved by earlier chemoradiotherapy techniques. Advances in radiotherapy technologies and techniques are being applied towards improving outcomes. Despite that, the median survival of locally advanced pancreatic carcinoma is ten to thirteen months which indicates the need for better treatment options. This article will discuss four abstracts published at 2012 American Society of Clinical Oncology (ASCO) Annual Meeting with the focus on locally advanced pancreatic cancer.
Update on Treatment of Locally Advanced Pancreatic Adenocarcinoma
Intratumoral Injection of TNF-alpha
In Abstract #4055, Wild et al. presented the results of a multi-center, randomized, phase III study using a novel tool of selective delivery of TNF-alpha to tumor cells by gene transfer through direct intratumoral injection [2]. Two-hundreds and 77 patients with locally advanced pancreatic adenocarcinoma were randomized 1:2 to the standard of care (5-FU/radiotherapy followed by gemcitabine) versus TNF-alpha plus standard of care.
Eighty-two percent of the patients in the TNF-alpha plus standard of care arm and 81% of the patients in the standard of care alone arm completed chemoradiation (P=0.80). Grade 2-4 adverse effects were observed in 76% of the TNF-alpha plus standard of care arm versus 66% of the standard of care alone arm (P=0.07).
The results are shown in Table 1. There were no significant differences in overall survival, progression free survival or time to radiologic progression between the two arms. However, subgroup analysis showed significant increase in overall survival in the TNFalpha plus standard of care arm (10.9 months) compared to the standard of care alone arm (9 months) in patients with T1-T3 disease (P=0.03)

Novel Agents in Combination with Gemcitabine
Two abstracts presented the use of novel agents in combination with Gemcitabine. In Abstract #TPS4134, Evans et al. presented a placebo-controlled, randomized, double blind phase II study evaluating the tolerability and the efficacy of adding the tyrosine kinase inhibitor, dasatinib, to gemcitabine in the treatment of locally advanced pancreatic cancer [3]. This study is multicenter, international targeting the accrual of 200 patients. Recruitment will occur in 120 participating centers in 15 countries. Patients will be randomized 1:1 to either i.v. gemcitabine 1,000 mg/m2 weekly for three weeks per cycle plus dasatinib 100 mg per day or gemcitabine plus placebo. Treatment will continue until unacceptable toxicity, disease progression, study termination or per patients choice. Study is still ongoing and results are not available yet. In Abstract #4050, Van Laethem et al. reported the results of phase I of a phase I/II study of the MEK inhibitor BAY 86-9766 in combination with gemcitabine in locally advanced and metastatic pancreatic cancer as first line therapy [4]. Ten patients were assigned to each of the two cohorts. In Cohort 1, patient received i.v. gemcitabine 1,000 mg/m2 weekly for 7 of 8 weeks in cycle one followed by 3 of 4 weeks in subsequent cycles in combination with oral BAY 86- 9766 30 mg twice daily. Median treatment duration with BAY 86-9766 was 105 days. Only one patient was still on treatment at data cut-off. Discontinuations were due to disease progression in 5 patients, adverse events not associated with clinical progression in 3 patients and adverse events associated with clinical progression in 1 patient. In this cohort, one patient died of acute liver failure due to chemotherapy-associated steatohepatitis. In Cohort 2, 10 patients received the same dose of gemcitabine in combination with BAY 86-9766 50 mg twice daily. Median treatment duration with BAY 86-9766 was 57 days. Four patients were still on treatment at data cut-off. Discontinuations were due to disease progression in one patient and adverse events not associated with clinical progression in 4 patients. One patient was withdrawn from the study and one patient developed grade 4 atypical pneumonia.
Fractionated Stereotactic Body Radiotherapy in Combination with Gemcitabine
In Abstract #4045 Herman et al. presented the results of their phase II, multi-institutional trial examining the role of gemcitabine and fractionated stereotactic body radiotherapy (SBRT) as an aggressive local treatment modality with acceptable toxicity [5]. While conventionally fractionated chemoradiotherapy is still the standard radiotherapy technique for pancreatic cancer, the promising results of SBRT in other settings, such as in lung cancer [6], have led to exploring their application in locally advanced pancreatic cancer. Earlier phase I/II studies with single fraction SBRT (25 Gray (Gy) x 1 fraction) showed excellent local progression free survival greater than 90% but with significant late gastrointestinal toxicity [7]. In this study, 32 patients with locally advanced pancreatic cancer who received gemcitabine in sequence with fractionated SBRT (6.6 Gy x 5 fractions, 33 Gy total) were enrolled and their local progression free survival, metastasis free survival, and overall survival were measured. A summary of their results are shown in Table 2.
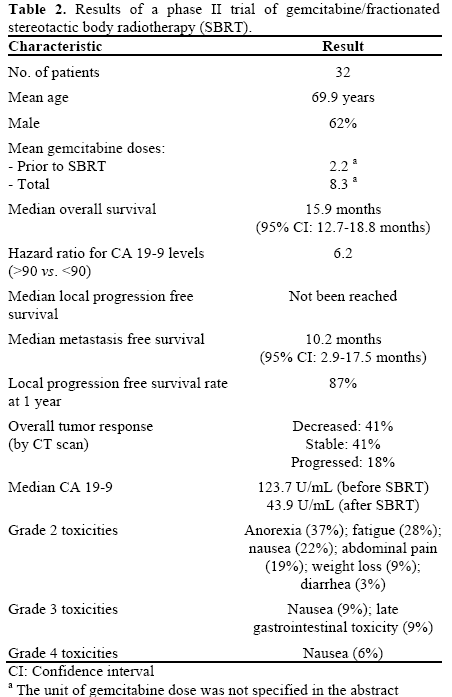
Given the encouraging results from this phase II trial, the authors concluded that fractionated SBRT with gemcitabine demonstrated excellent local control and tumor response with minimal grade 3 toxicities. Furthermore, there appeared to be a greater benefit for patients with CA 19-9 greater than 90 U/mL. The authors concluded that combining SBRT with more aggressive chemotherapy regimens may further improve efficacy.
Discussion
TNF-alpha is a 23 kilodalton type II transmembrane protein primarily produced by macrophages, but also by NK cells, T lymphocytes, smooth muscle cells, fibroblasts and others [8]. Release of TNF-alpha occurs in response to various inflammatory stimuli and cytokines [9]. Since the discovery of TNF-alpha in 1975, it has been the focus of considerable interest as an anticancer agent. However, the systemic use of recombinant human TNF-alpha (rhTNF-alpha) has been tested in several phase I and phase II clinical trials and has been associated with significant toxicities and a lack of evidence for therapeutic benefit [10]. The study presented by Wild et al. in Abstract #4055 explores a novel tool of selective delivery of TNFalpha intratumoral injection [2]. Although this is a negative study, there is a possible benefit of subgroup of patients such as patients with T1-T3 stage. In addition, Wild et al. utilized the intratumoral injection approach which limited the systemic toxicities and could be explored with other treatment agents.
Ras-Raf-MEK-ERK pathway is one of most extensively studied signaling pathways that connect various membrane receptors to the nucleus. Activation of this pathway controls a wide range of cellular processes such as proliferation, survival, and motility. Inappropriate activation has been shown to be a key regulatory factor for the pathogenesis of many types of human cancers [11]. K-ras, which is one isoform of Ras has been reported to be mutated in almost 100% of pancreatic ductal adenocarcinoma patients [12]. Two novel agents, targeting signaling pathways, have been tested, in combination with gemcitabine, based on preclinical data suggesting efficacy in treating pancreatic cancers. Van Laethem et al. is testing the MEK inhibitor, BAY 86-9766 in combination with gemcitabine [4]. The authors reported dose-limiting toxicity in each cohort (10%). However, there were 8 drug-related treatment-emergent serious adverse effects (50% in cohort 1 and 30% in cohort 2). Eight patients discontinued the treatment due to adverse effects (4, 40% in each cohort). The efficacy and tolerability of BAY 86-9766 50 mg bid in combination with gemcitabine is now being evaluated in the phase II part of this study. Dasatinib is an inhibitor of BCR-ABL, Src and other kinases. Src is a nonreceptor tyrosine kinase which activates Ras as well as many other pathways [13]. Preliminary data from a phase I clinical trial suggested efficacy of combining dasatinib with gemcitabine in solid tumors [14]. Evans et al. is studying this combination in a placebo-controlled, randomized, double blind phase II study [3]. The results are not available.
Stereotactic radiotherapy is one of the more rapidly evolving radiotherapy technologies, and SBRT for locally advanced pancreatic cancer is an emerging application in radiation oncology. The use of larger radiation fractions, tighter immobilization, and better image guidance may show equivalent or superior efficacy to conventional fractionation for certain tumors. The therapeutic potential of SBRT is even more intriguing with recent literature suggesting that large radiation fractions may have therapeutic effects through the tumor microenvironment, angiogenesis, or immunomodulation. The comparative efficacy of single fraction radiation (as is often used in radiosurgery) vs. fractionated SBRT is still unknown, and Herman et al. in Abstract #4045 examines its role in locally advanced pancreatic cancer [5]. The results of the phase II trial in Abstract #4045 are promising with a median overall survival of 15.9 months, which would be an improvement from current survival outcomes. Chemoradiation, whether through conventional techniques and fractionation or through emerging technologies and hypofractionation, remains important in the multi-modality management of locally advanced pancreatic cancer.
Conflict of interest
The authors have no potential conflicts of interest
References
- Epelbaum R, Rosenblatt E, Nasrallah S, Faraggi D, Gaitini D, Mizrahi S, Kuten A. Phase II study of gemcitabine combined with radiation therapy in patients with localized, unresectable pancreatic cancer. J Surg Oncol. 2002 Nov;81(3):138-43.
- Wild AT, Laheru D, Wang H, Chang KJ, Taylor GE, Donehower RC, et al. A randomized phase III multi-institutional study of TNFerade biologic with 5-FU and radiotherapy for locally advanced pancreatic cancer: Final results J Clin Oncol 2012; 30(Suppl):Abstract 4055.
- Evans TRJ, Van Cutsem E, Moore MJ, Purvis JD, Strauss LC, Rock EP, et al. Dasatinib combined with gemcitabine (Gem) in patients (pts) with locally advanced pancreatic adenocarcinoma (PaCa): Design of CA180-375, a placebo-controlled, randomized, double-blind phase II trial. J Clin Oncol 2012; 30(Suppl):Abstract TPS4134 .
- Van Laethem JL, Heinemann V, Martens UM, Jassem J, Michl P, Peeters M, et al. A phase I/II study of the MEK inhibitor BAY 86- 9766 (BAY) in combination with gemcitabine (GEM) in patients with nonresectable, locally advanced or metastatic pancreatic cancer (PC): Phase I dose-escalation results. J Clin Oncol 2012; 30(Suppl):Abstract 4050.
- Herman JM, Chang DT, Goodman KA, AWild AT, Laheru D, Zheng L, et al. A phase II multi-institutional study to evaluate gemcitabine and fractionated stereotactic body radiotherapy for unresectable, locally advanced pancreatic adenocarcinoma. J Clin Oncol 2012; 30(Suppl):Abstract 4045.
- Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010 Mar 17;303(11):1070-6.
- Schellenberg D, Goodman KA, Lee F, et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy forlocally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2008 Nov 1;72(3):678-86.
- vanHorssen R, Ten Hagen TL, Eggermont AM. TNF-alpha in cancer treatment: molecular insights, antitumor effects, and clinical utility. Oncologist. 2006;11:397–408
- Locksley RM, Killeen N, Lenardo MJ. The TNF and TNF receptor superfamilies: integrating mammalian biology. Cell. 2001;104:487–501.
- Jones AL, O'Brien ME, Lorentzos A, Viner C, Hanrahan A, Moore J, Millar JL, Gore ME. A randomised phase II study of carmustine alone or in combination with tumour necrosis factor in patients with advanced melanoma. Cancer Chemother Pharmacol. 1992;30:73–76
- Hoshino R., Chatani Y., Yamori T., Tsuruo T., Oka H., Yoshida O., Shimada Y., Ari-i S., Wada H., Fujimoto J., Kohno M., Oncogene, 18, 813—822 (1999).
- Almoguera C, Shibata D, Forrester K, et al. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell 1988;53:549–554.
- Khoury HJ, Guilhot F, Hughes TP, et al. Dasatinib treatment for Philadelphia chromosome-positive leukemias: practical considerations. Cancer 2009;115:1381–1394.
- Uronis HE, Bullock K, Blobe G, Hsu S, Morse M, Nixon A, et al. A phase I study of gemcitabine plus dasatinib (GD) or gemcitabine plus dasatinib plus cetuximab (GDC) in refractory solid tumors. J Clin Oncol 2009; 27(Suppl):Abstract e15506.

