Keywords
Adenocarcinoma; Carcinoma, Pancreatic Ductal; Fluorouracil; gemcitabine; Oxaliplatin; Pancreatic Neoplasms; Radiotherapy; Salvage Therapy; Treatment Failure; Genes; DNA; RNA
Abbreviations
PC Pancreatic Cancer; APC Advanced Pancreatic Cancer; EGF Epidermal Growth Factor; GEMCAP Gemcitabine Plus Capecitabine; CRT Chemoradiotherapy;
Introduction
Pancreatic cancer (PC) has the worst survival of any
solid tumor. The American Cancer Society’s estimates
that 57,600 people (30,400 men and 27,200 women) will
be diagnosed with PC in the United States for 2020 and
approximately 47,050 people (24,640 men and 22,410
women) will die of PC [1]. Overall, PC accounts for about
3% of all cancers in the US and about 7% of all cancer
deaths [1]. The incidence of PC is slightly more common
in men than in women and more common in African-
Americans than in Whites [2]. The average lifetime risk of
developing PC is about 1 in 64, however, the individual’s
risks of developing PC can be impacted by certain risk
factors, including both personal and genetic [3].
What We Knew Before the 2020 ASCO Annual
Meeting?
Even though surgery is the only potentially curative
treatment for patients with PC, but unfortunately less
than 20% are resectable at the time of diagnosis [4, 5]. Chemotherapy for 6 months including FOLFIRINOX
(5-fluorouracil, leucovorin, irinotecan, and oxaliplatin),
gemcitabine plus capecitabine, gemcitabine alone, or S-1
alone (where it is available) is generally the accepted
gold standard across the globe, except oncologists in USA
still include radiation in selected cases [5, 6, 7, 8, 9]. Even
in those patients who receive adjuvant chemotherapy,
majority of them succumb to death due to metastases
[4]. Neoadjuvant trials have been undergoing more
aggressively to address this issue. On the other end,
palliative chemotherapy remains the treatment of choice
in the management of those with advanced pancreatic
cancer (APC). Options in the first-line consist of single
agent gemcitabine, the combination of gemcitabine with
the epidermal growth factor (EGF) inhibitor erlotinib,
FOLFIRINOX, or the combination of gemcitabine with nabpaclitaxel
[10, 11, 12, 13]. Though few studies have tested
few agents in the second-line, but liposome irinotecan with
5-FU and leucovorin is the only FDA-approved regimen in
this setting [14]. It is evident that the currently available
options are limited and the window of opportunity to
offer treatment to these patients remain to be short, which
further compounded by the deteriorated quality of life due
to cancer-related symptoms. There it is imperative that
we develop molecularly-targeted agents, biomarkers to
select the available conventional chemotherapy to prevent
toxicity, such as organoids and explore other pathways
in the cascade of pancreatic carcinogenesis, including
immunotherapy.
What We Learnt at the 2020 ASCO Annual Meeting?
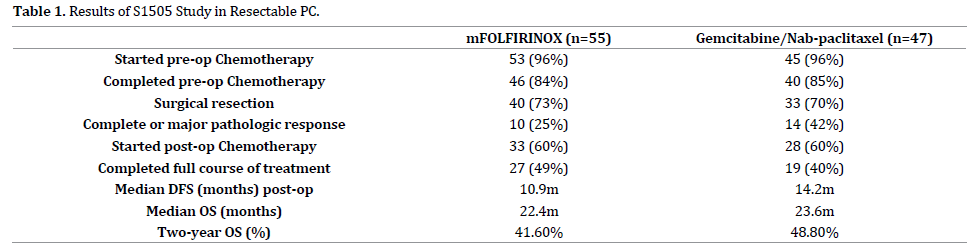
SWOG S1505 was presented at the meeting
(NCT02562716) [15]. S1505 was a randomized phase II
trial of peri-operative chemotherapy with mFOLFIRINOX
versus gemcitabine/nab-paclitaxel (12 weeks pre-op, 12 weeks post-op) for resectable PC (PDA). A total of
147 patients were enrolled and out of them, 102 were
found eligible. The outcomes of S1505 for each arm are
summarized in Table 1. Overall, neither arm’s 2-year OS
estimate was statistically significantly higher than the a
priori threshold of 40% (p=0.42 in Arm 1 and p=0.12 in
Arm 2). Toxicities were consistent with previous studies.
In summary, this study showed the feasibility of the use of
both regimens but also failed to show any survival benefit
compared to the historical standard.
Our European researchers presented the results of the
ESPAC-5F (89500674), a 4-arm, prospective, multicenter,
international randomized phase II trial to determine the
feasibility and efficacy of a comparison of immediate surgery
compared with neoadjuvant gemcitabine plus capecitabine
(GEMCAP) or FOLFIRINOX or chemoradiotherapy (CRT) in
patients with borderline resectable PC [16]. The primary
objectives were recruitment rate and resection rate (R1/
R0) and secondary objectives were to assess overall
survival and toxicity. Patients were randomized to undergo
immediate surgery, or receive neoadjuvant therapy of
either 2 cycles of GEMCAP, or 4 cycles of FOLFIRINOX
or 50.4Gy capecitabine-based CRT in 28 daily fractions
over 5.5 weeks. Patients were restaged at an interval of
4-6 weeks and surgery was performed if stage remained
to be borderline resectable. Following surgical resection,
patients received adjuvant therapy.
18 of 20 patients received 2 cycles of GEMCAP while
the rest 2 did not receive any chemotherapy. 25% patients
were able to complete the planned GEMCAP. 15 of 20
patients received the 4 cycles of mFOLFIRINOX while
the rest 5 did not receive any chemotherapy. Akin to
GEMCAP, 25% patients were able to complete the planned
FOLFIRINOX. 12 of 20 patients received 5.5 weeks of CRT
while 2 patients in this arm did not receive any treatment.
38% patients in this arm finished the planned CRT.
Resection rates (including R0 and R1) was 62% for
those who underwent immediate surgery versus 55%
for those who received neoadjuvant therapy (GEMCAP,
FOLFIRINOX or CRT) with a p value of 0.668) while
R0 resection rate was 15% and 23% for the two arms
respectively (p=0.721). One-year survival rate was 40% [95% CI, 26% – 62%] for immediate surgery and 77%
[95%CI, 66% - 89%] for neoadjuvant therapy with an HR
ratio of 0.27 [95% CI, 0.13 – 0.55 and P value of <0.001
(Table 2). The investigators concluded that there was
no statistical difference in resection rates for immediate
surgery versus neoadjuvant therapy. However, there was a
significant survival advantage at one year for neoadjuvant
therapy versus immediate surgery. Among the three
treatment options, FOFIRINOX was the superior as shown
below:

In short, neoadjuvant should be considered for patients
with borderline resectable PC.
It is a known fact that age is a risk factor for PC and
majority of the patients are above the age of > 70 years.
ESPAC-4 study included patients with median age of
65 years (37-81) and ECOG performance status (PS) of
0 (43%), 1 (54%) and 2 (2%). Our group presented our
experience with an adopted biweekly regimen of s-GEMCAP
in patients who were ≥ 75 years and those who were
deemed not suitable for ESPAC-4 regimen [17]. Thirty-five
(22M, 13F) patients, ≥ 75 (median age 79), ECOG PS 1 in 7
(28%) patients and 2 in 28 (72%) who received a modified
regimen of gemcitabine (1000-2000 mg/m2) every 2
weeks and capecitabine (800-1000 mg/m2) day 1-7 every
2 weeks. Patients were evaluated for DFS, OS and sites
of recurrence. Toxicities were graded according to NCI
CTCAE v5.0. Updated data at the conclusion of 38 months
showed median DFS of 11 months and OS of 24.0 months.
Nine (25%) had local recurrence, 21 (60%) had metastatic
disease and 3 (8.6%) had NED. The most frequent toxicities
were grades 1-2 anemia (20%), thrombocytopenia (8%)
and hand-foot syndrome (HFS) (10%). Grade ≥3 included
diarrhea (4%) and HFS (1%) with no treatment-related
discontinuations. Treatment compliance was 100%.
Delays were necessary in 7% of cases and dose reduction
was required in 4% of cases. There was no treatment
related death. This schedule of biweekly s-GEMCAP
regimen suggests an acceptable option in for elderly,
frail patients with PC and warrants further exploration in
patients not suitable for FOLFIRINOX, full dose GEMCAP
or a clinical trial. In addition, this schedule is optimum for
administration of pegylated-filgrastim. Moreover, fewer visits to oncology and related expense do favor towards
benefit. Additionally, this tolerable regimen is ideal to be
combined with immunotherapy in clinical trials for this
patient population.
Many new agents were also presented at the meeting,
such as CPI-613 (Devimistat) and Cobimetinib, MEK
inhibitor and hopefully will be tested in randomized phase
III studies to confirm their benefit towards APC [18, 19].
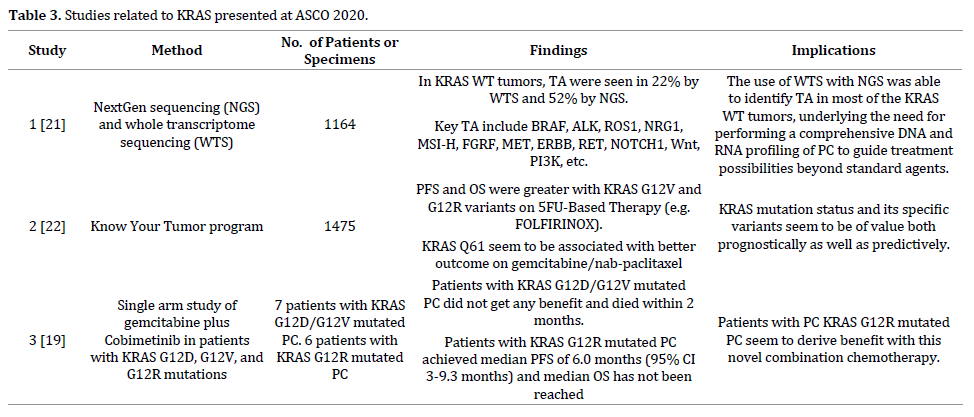
It is well-known that about 90% of PC tumors carry
KRAS mutations [20, 21, 22]. Recently investigators have
looked back at this abnormality to investigate the clinical
and biological impact of KRAS variants and The biological and clinical impact of common KRAS
variants, such as G12D, G12V, G12R as well as explore any
potential targetable alterations related to this pathway. Of
note, three studies related to this topic were presented as
summarized in Table 3.
What we need to do next?
It is extremely important to bear in mind that patients
with pancreatic cancer should be referred to centers
of excellence. Importance of multidisciplinary teams in
order to improve survival in these patients cannot be over
emphasized [23]. We need to develop of PC networks to
improve access to trials and to coordinate collaboration
between healthcare professionals and industry to
improve outcomes. Cooperation between industry and
academia needs to be further improved to ensure that
trials are relevant to clinical practice as well as Improve
access to newly registered drugs. Early introduction
of palliative care alongside chemotherapy to improve
quality of life, mood and outcomes. It is important that we
standardize the management of PC across the globe and
base treatment selection on evidence-based national and
international guidelines. Randomized controlled trials
using a standardized protocol for pancreatic specimen
examination for ease of comparison between studies
should be applied. Tumor and patient profiling are critical in understanding disease, developing new treatments and
better selecting patients for optimal therapy. Less invasive
strategies, such as profiling of CTDNA may overcome need
to procure tumor tissue [24]. NCCN also recommends germline
mutational analysis in patients with PC [25]. Detection
and treatment in high-risk patients should continue with
multidisciplinary teams, with comprehensive genetic
testing, counseling services and development of screening
markers.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- American Cancer Society. Facts & Figures 2020.
- SEER Cancer Statistics Review 1975-2015
- Noone AM, Howlader N, Krapcho M, Miller D, Brest A, Yu M, et al. (eds) SEER Cancer Statistics Review, 1975-2015. National Cancer Institute, Bethesda 2018.
- Conlon KC, Klimstra DS, Brennan MF. Long-term survival after curative resection for pancreatic ductal adenocarcinoma. Clinicopathologic analysis of 5-year survivors. Ann Surg 1996; 223:273-279. [PMID: 8604907]
- Yeo CJ, Abrams RA, Grochow LB, Sohn TA, Ord SE, Hruban RH, et al. Pancreaticoduodenectomy for pancreatic adenocarcinoma: postoperative adjuvant chemoradiation improves survival. A prospective, single-institution experience. Ann Surg 1997; 225:621-633. [PMID: 9193189]
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelskiet K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 2007; 297:267-277. [PMID: 17227978]
- Conroy T, Hammel P, Hebbar M, Abdelghani MB, Wei AC, Raoul JL, et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N Engl J Med 2018; 379:2395-2406. [PMID: 30575490]
- Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 2017; 389:1011-1024. [PMID: 28129987]
- Uesaka K, Boku N, Fukutomi A, Okamura Y, Konishi M, Matsumoto I, et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: a phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet 2016; 388:248-257. [PMID: 27265347]
- Burris HA, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-2413. [PMID: 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-1966. [PMID: 17452677]
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarnet Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-1825. [PMID: 21561347]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369:1691-1703. [PMID: 24131140]
- Wang-Gillam A, Li CP, Bodoky G, Dean A, Shan YS, Jameson G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. Lancet 2016; 387:545-557. [PMID: 26615328]
- Davendra Sohal, Mai T. Duong, Syed A. Ahmad, Namita Gandhi, Muhammad Shaalan Beg, Andrea Wang-Gillam, James Lloyd Wade, Elena Gabriela Chiorean, Katherine A Guthrie, Andrew M. Lowy, Philip Agop Philip, Howard S. Hochster. SWOG S1505: Results of perioperative chemotherapy (peri-op CTx) with mfolfirinox versus gemcitabine/nab-paclitaxel (Gem/nabP) for resectable pancreatic ductal adenocarcinoma (PDA). J Clin Oncol 38: 2020 (suppl; abstr 4504)
- Ghaneh P, Palmer DH, Cicconi S, Halloran C, Psarelli EE, Rawcliffe CL, et al. ESPAC-5F: Four-arm, prospective, multicenter, international randomized phase II trial of immediate surgery compared with neoadjuvant gemcitabine plus capecitabine (GEMCAP) or FOLFIRINOX or chemoradiotherapy (CRT) in patients with borderline resectable pancreatic cancer. J Clin Oncol 2020; 38.
- Hakim N, Chi J, Rehman H, Nealon W, Deutsch GB, Newman E, et al. Safety and efficacy of biweekly gemcitabine in combination with capecitabine (GemCap) in elderly and frail patients (pts) with resected pancreatic cancer (PC). J Clin Oncol 2020; 38.
- Alistar AT, Morris B, Harrison L, Bickenbach K, Starker, Ginder N, et al. A single-arm, open-label, phase I study of CPI-613 (Devimistat) in combination with gemcitabine and nab-paclitaxel for patients with locally advanced or metastatic pancreatic adenocarcinoma. J Clin Oncol 2020; 38.
- Ardalan B, Cotta JA, Gombosh M, Azqueta JA. Cobimetinib plus gemcitabine is an active combination in KRAS G12R-mutated in previously chemotherapy-treated and failed pancreatic patients. J Clin Oncol 2020; 38.
- Agarwal A, Saif MW. KRAS in pancreatic cancer. JOP 2014; 15:303‐305. [PMID: 25076326]
- Philip PA, Xiu J, Hall MJ, Hendifar AE, Lou E, Hwang JJ, et al. Enrichment of alterations in targetable molecular pathways in KRAS wild-type (WT) pancreatic cancer (PC). J Clin Oncol 2020; 38.
- Hendifar AE, Blais EM, Ng C, Thach D, Gong J, Sohal D, et al. Comprehensive analysis of KRAS variants in patients (pts) with pancreatic cancer (PDAC): Clinical/molecular correlations and real-world outcomes across standard therapies. J Clin Oncol 2020; 38.
- Lidsky ME, Sun Z, Nussbaum DP, Adam MA, Speicher PJ, Blazeret DG, et al. Going the Extra Mile: Improved Survival for Pancreatic Cancer Patients Traveling to High-volume Centers. Ann Surg 2017; 266:333-338. [PMID: 27429020]
- Chen L, Zhang Y, Cheng Y, Zhang D, Zhu S, Ma X. Prognostic value of circulating cell-free DNA in patients with pancreatic cancer: A systemic review and meta-analysis. Gene 2018; 679:328‐334. [PMID: 30227250]
- NCCN Guidelines for Patients. Pancreatic Cancer 2019.

