Key words
Drug Evaluation, Preclinical; Nutrition Therapy; Pancreatitis; Pancreatitis, Acute Necrotizing; Pancreatitis, Alcoholic; Pharmacological Actions Category; Practice Guidelines

This slide presentation took place at the Meeting of the European Societies of Pancreatology held in Lisbon in October 2005.
In the last few years, several new therapeutic options have changed the management of acute pancreatitis; for example, the therapeutic ERCP with endoscopic sphincterotomy in severe biliary pancreatitis, the use of early antibiotic treatment in necrotizing pancreatitis and the demonstration that enteral feeding is able to decrease the inflammatory response. In this paper we describe the therapeutic news which could modify the current approach to acute pancreatitis in the near future. This is possible only because we have new information in order to better understand the pathophysiological processes of the disease.
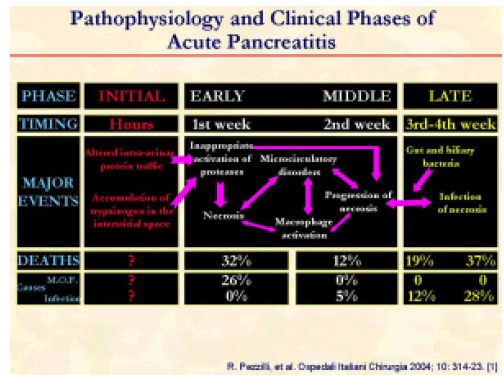
We can distinguish three clinical phases regarding the pathophysiology of acute pancreatitis. There is not very much information on the initial phase of the disease in humans and, for the most part, it comes from experimental studies [1]. Of course, it is apparent that we can obtain good therapeutic results only if we treat the pancreatitis as soon as possible.
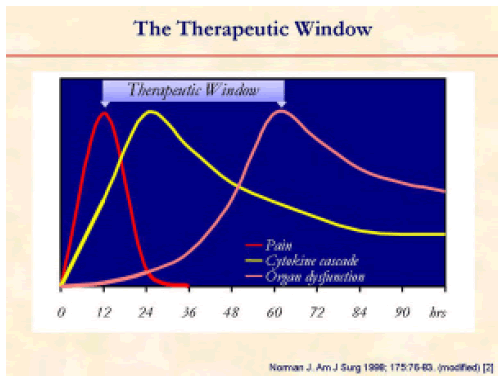
The time limit for efficacious medical treatment is of no more than 60 hours from the onset of symptoms of acute pancreatitis [2].
Another important aspect as to the correct approach to the management of acute pancreatitis is the correct clinical classification of acute pancreatitis. We should thank Dr. Bradley for his efforts in changing the classification of the disease from a pathological to a clinical point of view [3].
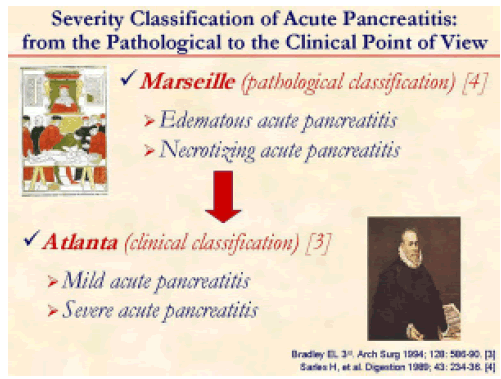
The work of Bradley can be summarized in the evolution from the Marseille [4] to the Atlanta [3] classification system.
As in other diseases, also in acute pancreatitis, the pathophysiological aspects of the disease should guide our therapeutic approach. On the other hand, we should also consider that the treatment needs to be tailored to each individual patient and we also should take into account the available resources of each Institution.
In the last few years, the need has emerged to treat patients with acute pancreatitis according to new knowledge accumulated from clinical research in order to improve the morbidity and the mortality of the disease.
Since 1994, many papers have been published suggesting the good medical practice to be followed in the treatment of acute pancreatitis [3, 5, 6, 7, 8, 9, 10, 11, 12].
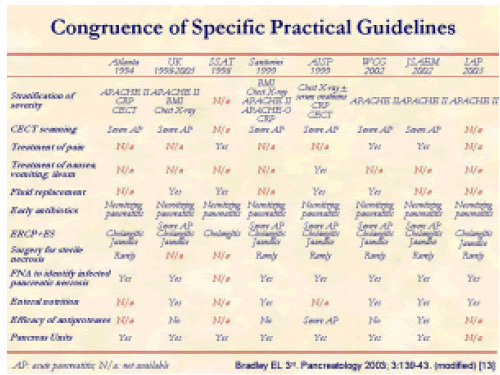
There is no congruence in the various guidelines regarding stratification of severity, diagnosis, treatment and presence of Pancreas Units [13].
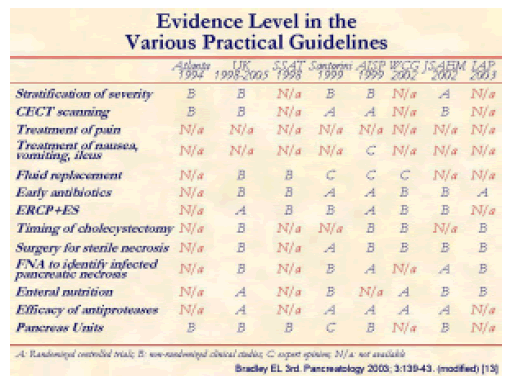
In the same way, there are no homogeneous evidence levels in the various guidelines [13].
These differences are quite surprising because most of the participants are the same experts who decide on the various guidelines.
In addition to the suggestion of Bradley about the need of guiding the reluctants [13], there is also the need to unify the various guidelines.
One example of rapid evolution of the knowledge of acute pancreatitis is the following: the UK guidelines were released in 1998 [5], revised in 2005 [6] and, after just a few weeks, some researchers asked to change the new 2005 UK guidelines [14].
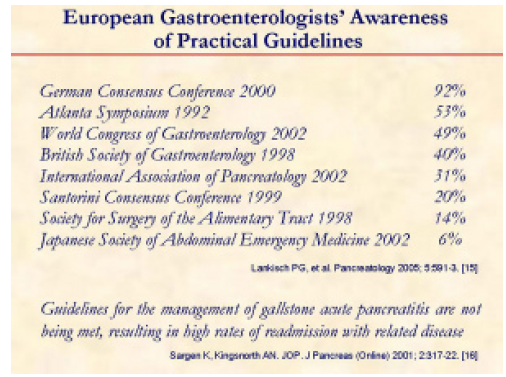
Another problem with the guidelines is that many clinical practitioners in the same country follow different guidelines [15] and others do not fully apply them in clinical practice [16].
In most of the guidelines, the basic management of acute pancreatitis is not reported: some examples are the control of pain and the control of the nausea, vomiting and ileus.
First of all, what about the control of pain?
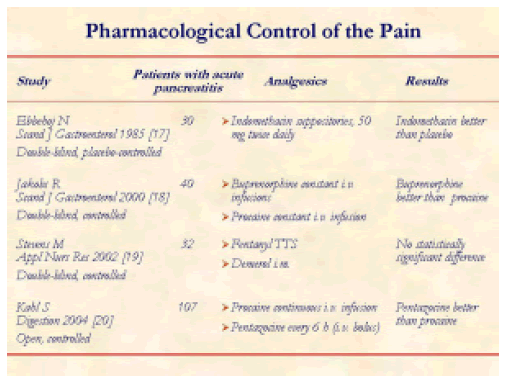
There are no extensive studies on the pharmacological control of pain in acute pancreatitis [17, 18, 19, 20]; this is quite surprising due to importance of this symptom.
Second, what about the control of nausea, vomiting, and ileus?
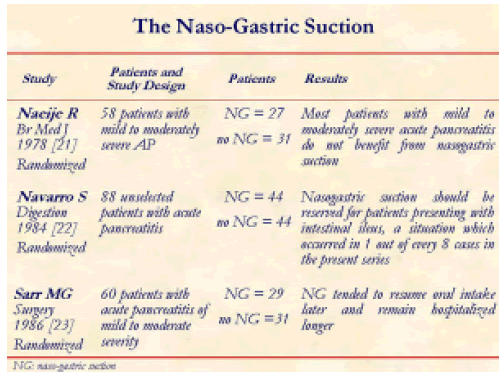
Naso-gastric suction is often used in patients with acute pancreatitis, even if most of the published studies limit this approach only to the patients with severe disease [21, 22, 23].
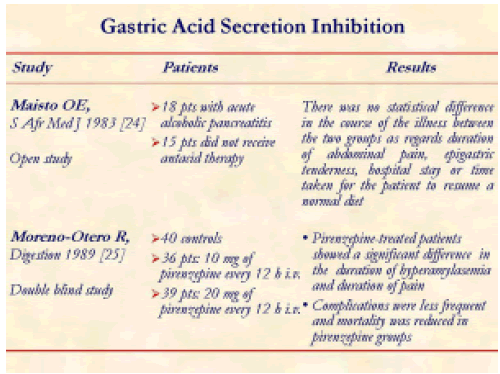
Gastric acid secretion inhibition is largely used in patients with acute pancreatitis, even if there are very few studies on this issue and the results are not conclusive [24, 25].
Even if many studies have been carried out, only a few of the substances tested have been applied in clinical practice.
This is the first experimental study exploring the usefulness of Infliximab in the treatment of severe acute pancreatitis [26].
Antioxidant treatment for acute pancreatitis is a neverending story; this is one of the most recent studies exploring the usefulness of a new antioxidative drug in experimental acute pancreatitis [27].
A paper published in 2001 highlighted the limitations of experimental models in acute pancreatitis [28].
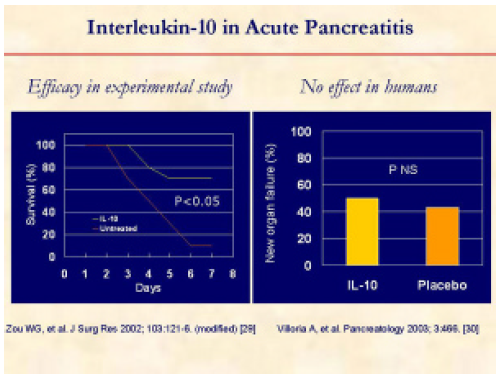
Interleukin-10 represents a case of limitation of experimental research. In fact, this molecule was unable to prevent new organ failures in clinical practice [29, 30].
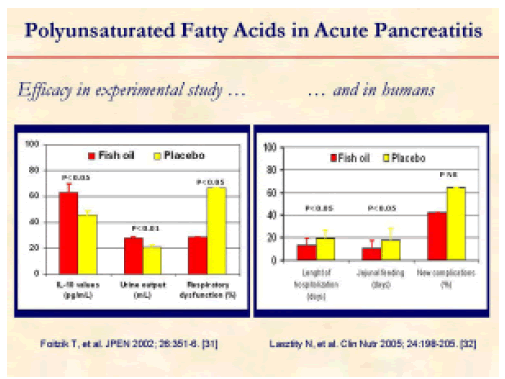
On the other hand, polyunsaturated fatty acids were able to decrease the length of hospitalization and the duration of jejunal feeding in humans, even if they were not able to decrease the number of new complications [31, 32].
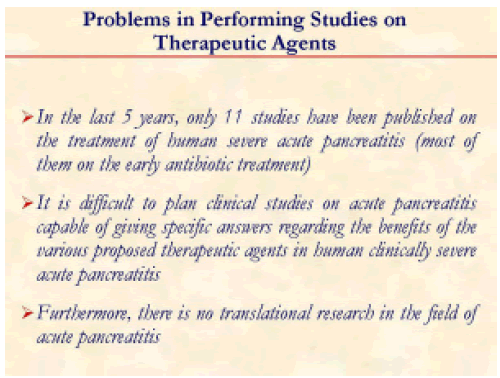
What are the problems in carrying out studies on therapeutic agents in acute pancreatitis?
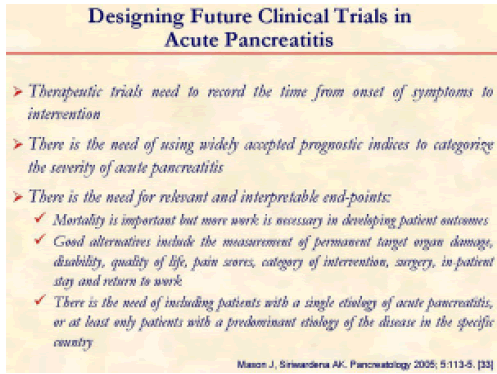
There is the need to better design future clinical trials in acute pancreatitis [33].
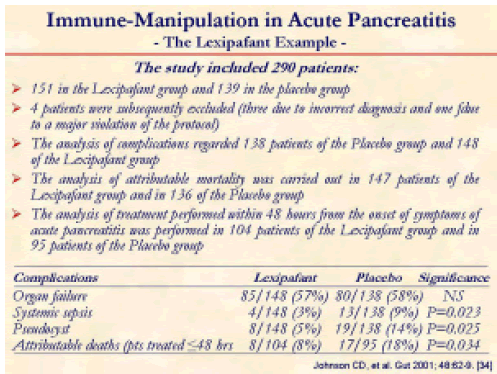
The high incidence of organ failure within 72 hours after the onset of symptoms has undermined the primary hypothesis, and power calculations for future studies on severe acute pancreatitis will need to allow for this. Lexipafant had no effect on new organ failure during treatment. This study - performed with an adequately sized sample - has shown that antagonism of the PAF activity on its own is not sufficient to ameliorate SIRS in severe acute pancreatitis: However, if we look at the data reported, we cannot exclude that Lexipafant may have some effect, especially in patients treated within 48 hours from the onset of symptoms [34].
The restoration of homeostasis with a single intervention belies the complex and coordinated nature of the inflammatory response. In clinical practice there is necessity of not using “magic” drugs alone: there is the need for more drugs capable of involving the different aspects of the disease [35].
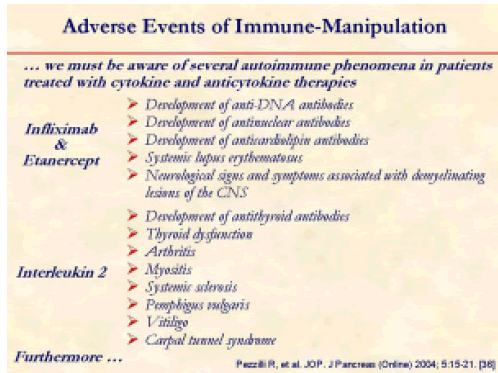
Furthermore, we must be aware of several autoimmune phenomena in patients treated with cytokine and anticytokine therapies [36].
We also need to change the way results of drug trials are communicated to the medical world [35].
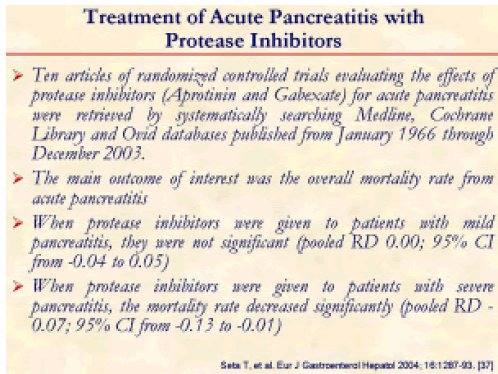
One example may be the highly debated efficacy of protease inhibitors in human acute pancreatitis [37].
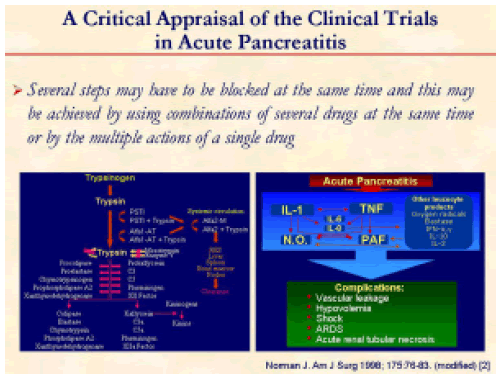
Several steps may have to be blocked at the same time and this might be achieved by using several drug combinations at the same time or by the multiple action of a single drug in order to block the protease cascade as well as the cytokine cascade [2].
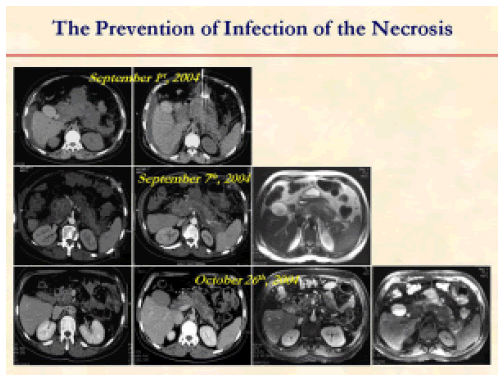
Another important aspect for the treatment of acute pancreatitis is the prevention of the infection of pancreatic necrosis.
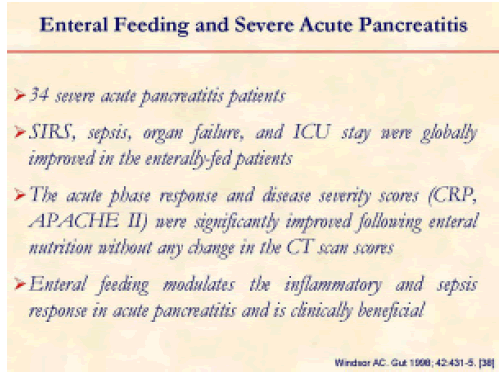
This is the first clinical study demonstrating the beneficial effect of enteral nutrition in decreasing the inflammatory and sepsis response in severe pancreatitis [38].
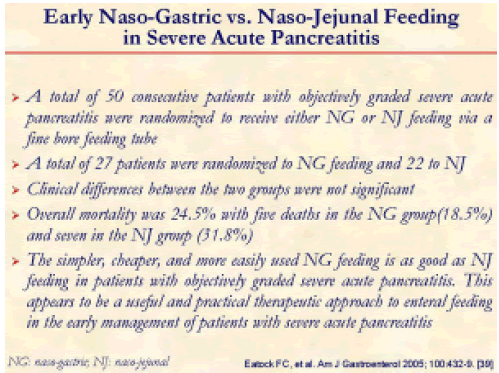
There is no doubt that it is better to administer enteral feeding via a naso-gastric tube than via a naso-jejunal tube [39].
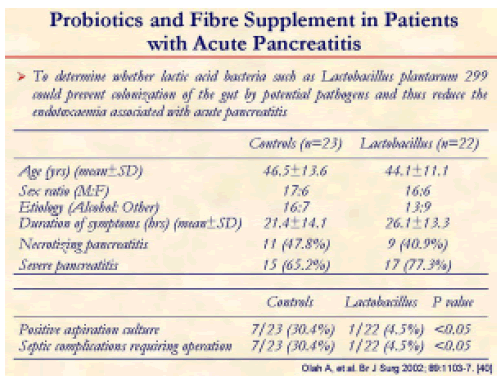
There is also no doubt that probiotics associated with enteral feeding may become an alternative therapy replacing early antibiotic use to prevent infection in severe pancreatitis [40].
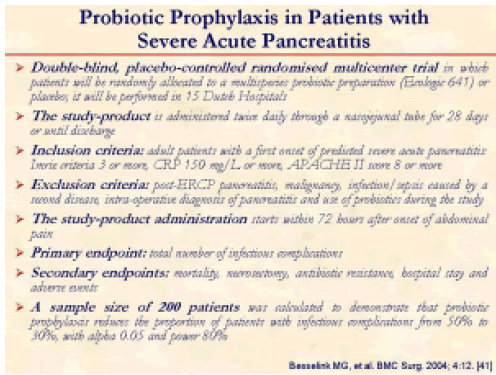
We are awaiting the results of this study in order to draw the final conclusion on the effectiveness of probiotic prophylaxis in preventing septic complications in severe acute pancreatitis [41].
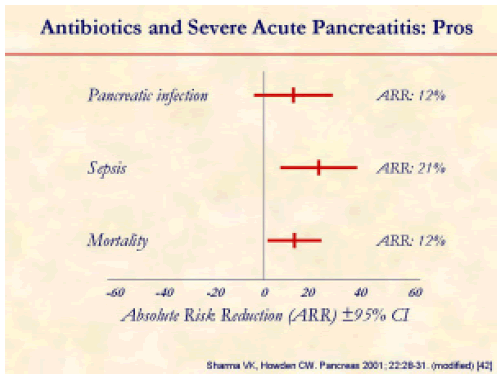
This meta-analysis shows the need for using early antibiotic therapy in order to prevent sepsis and mortality in severe acute pancreatitis [42].
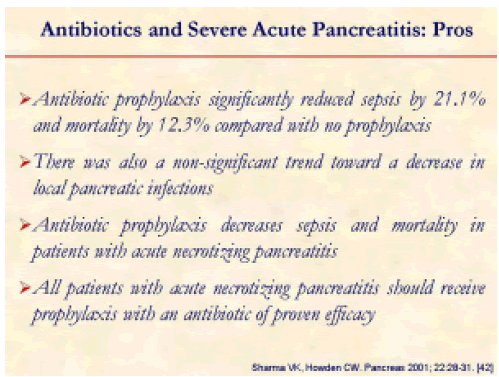
The authors concluded that all patients with acute necrotizing pancreatitis should receive early antibiotic treatment [42].
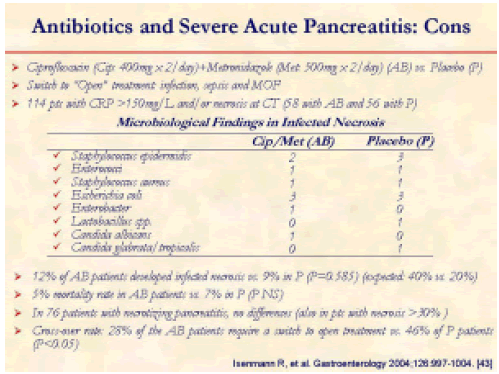
However, not all researchers agree that severe acute pancreatitis should be treated with early antibiotic administration [43].
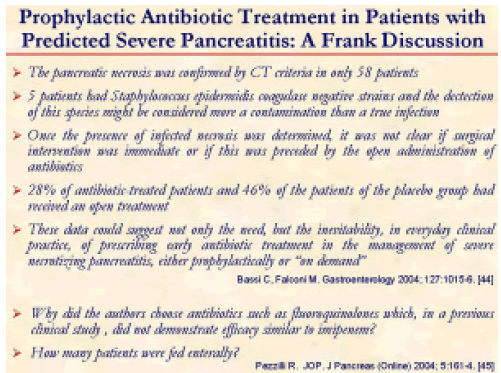
After the publication of the paper of Isenmann R, et al. [43], a discussion on its validity was opened [44, 45].
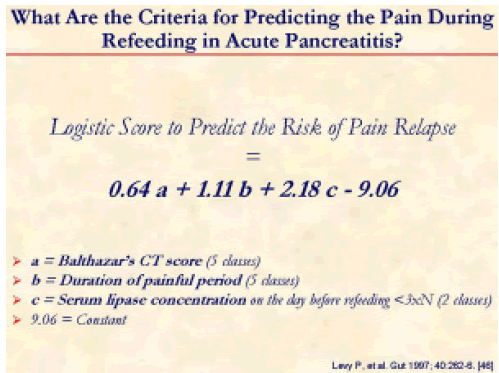
Refeeding is crucial in patients who have recovered from an acute episode of pancreatitis but there are very few studies on this issue [46].
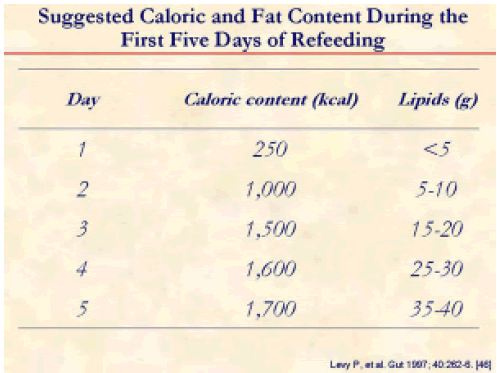
This is the suggested caloric intake for the refeeding of acute pancreatitis patients [46].
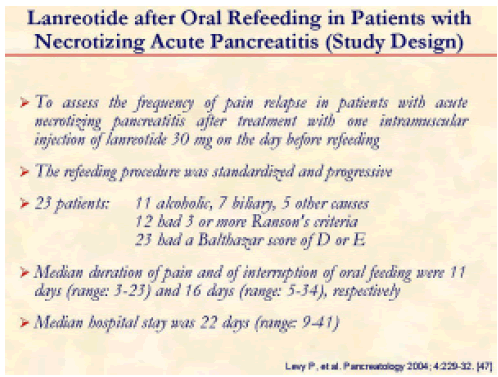
To prevent an acute relapse of acute pancreatitis, the use of lanreotide has been suggested [47].
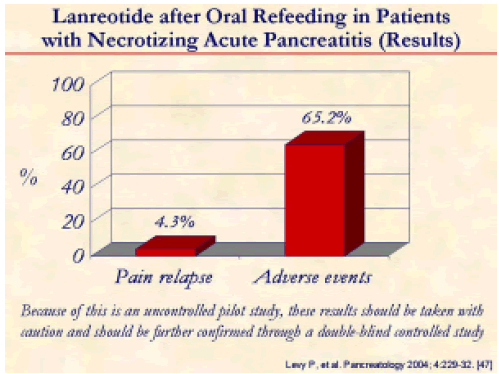
In this French study, only 4.3% of the patients treated with Lanreotide had relapse of pain from acute pancreatitis, but 65.2% experienced adverse effect using the drug [47].
There are very few studies evaluating the exocrine pancreatic function after an acute episode of pancreatitis [48, 49, 50, 51].
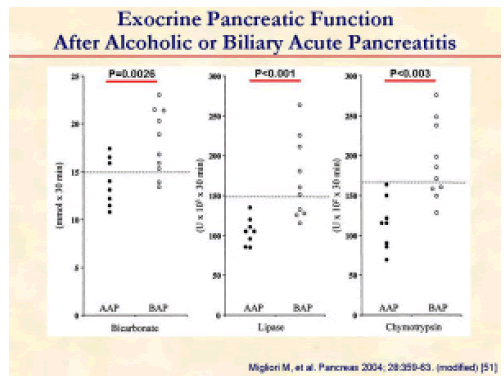
An example of the exocrine pancreatic study comes from the paper of Migliori et al. [51]. In this study patients with acute pancreatitis were studied using the secretin-cerulein test. After acute alcoholic pancreatitis, pancreatic insufficiency was significantly more frequent and more severe than after biliary pancreatitis. These findings, together with the fact that the insufficiency was also more persistent, suggest that acute alcoholic pancreatitis may occur in a pancreas which already has chronic lesions.
Enzyme supplementation during the refeeding of patients with acute pancreatitis represents an important issue regarding nutritional support. However, there are no studies showing the possible efficacy of enzyme oral supplementation especially in those patients who suffered from acute alcoholic pancreatitis.
References
- Pezzilli R, Ceciliato R, Corinaldesi R. The pathogenesis of acute pancreatitis: from basic research to the bedside. Osp It Chir 2004; 10:314-23.
- Norman J. The role of cytokines in the pathogenesis of acute pancreatitis. Am J Surg 1998; 175:76-83. [PMID 9445247]
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga., September 11 through 13, 1992. Arch Surg 1994; 128:586-90. [PMID 8489394]
- Sarles H, Adler G, Dani R, Frey C, Gullo L, Harada H, Martin E, et al. Classifications of pancreatitis and definition of pancreatic diseases. Digestion 1989; 43:234-6. [PMID 2612747]
- United Kingdom guidelines for the management of acute pancreatitis. Gut 1998; 42 (Suppl 2):1S-13S. [PMID 9764029]
- UK guidelines for the management of acute pancreatitis. Working Party of the British Society of Gastroenterology; Association of Surgeons of Great Britain and Ireland; Pancreatic Society of Great Britain and Ireland; Association of Upper GI Surgeons of Great Britain and Ireland. Gut 2005; 54(Suppl 3:iii):1- 9. [PMID 15831893]
- The Society for Surgery of the Alimentary Tract Patient Care Committee. Treatment of acute pancreatitis. J Gastrointest Surg 1998; 2:487-8. [PMID 9935328]
- Dervenis C, Johnson CD, Bassi C, Bradley EL III, Imrie CW, McMahon MJ, Modlin I. Diagnosis, objective assessment of severity, and management of acute pancreatitis: Santorini consensus conference. Int J Pancreatol 1999; 25:195-210. [PMID 10453421]
- Uomo G, Pezzilli R, Cavallini G, and ProInf- A.I.S.P. Study Group. The management of acute pancreatitis in clinical practice. Ital J Gastroenterol Hepatol 1999; 31:635-42. [PMID 10604108]
- Toouli J, Brooke-Smith M, Bassi C, Carr-Locke D, Telford J, Freeny P, et al. Working Party of the Program Commitee of the Bangkok World Congress of Gastroenterology 2002. Guidelines for the management of acute pancreatitis. J Gastroenterol Hepatol 2002; 17(Suppl):S15-39. [PMID 12000591]
- Mayumi T, Ura H, Arata S, Kitamura N, Kiriyama I, Shibuya K, et al. Working Group for the Practical Guidelines for Acute Pancreatitis. Japanese Society of Emergency Abdominal Medicine. Evidence-based clinical practice guidelines for acute pancreatitis: proposals. J Hepatobiliary Pancreat Surg 2002; 9:413- 22. [PMID 12483262]
- Uhl W, Warshaw A, Imrie C, Bassi C, McKay CJ, Lankisch PG, et al. IAP guidelines for the surgical management of acute pancreatitis. Pancreatology 2002; 2:565-73. [PMID 12435871]
- Bradley EL 3rd. Guiding the reluctant. A primer on guidelines in general and pancreatitis in particular. Pancreatology 2003; 3:139-43. [PMID 12748422]
- Gurusamy KS, Farouk M, Tweedie JH. UK guidelines for management of acute pancreatitis: is it time to change? Gut 2005; 54:1344-5. [PMID 16099804]
- Lankisch PG, Weber-Dany B, Lerch MM. Clinical perspectives in pancreatology: compliance with acute pancreatitis guidelines in Germany. Pancreatology 2005; 5:591-3. [PMID 16110257]
- Sargen K, Kingsnorth AN. Management of gallstone pancreatitis: effects of deviation from clinical guidelines. JOP. J Pancreas (Online) 2001; 2:317-22. [PMID 11877542]
- Ebbehoj N, Friis J, Svendsen LB, Bulow S, Madsen P. Indomethacin treatment of acute pancreatitis. A controlled double-blind trial. Scand J Gastroenterol 1985; 20:798-800. [PMID 2413519]
- Jakobs R, Adamek MU, von Bubnoff AC, Riemann JF. Buprenorphine or procaine for pain relief in acute pancreatitis. A prospective randomized study. Scand J Gastroenterol 2000; 35:1319-23. [PMID 11199374]
- Stevens M, Esler R, Asher G. Transdermal fentanyl for the management of acute pancreatitis pain. Appl Nurs Res 2002; 15:102-10. [PMID 11994827]
- Kahl S, Zimmermann S, Pross M, Schulz HU, Schmidt U, Malfertheiner P. Procaine hydrochloride fails to relieve pain in patients with acute pancreatitis. Digestion 2004; 69:5-9. [PMID 14755147]
- Naeije R, Salingret E, Clumeck N, De Troyer A, Devis G. Is nasogastric suction necessary in acute pancreatitis? Br Med J 1978; 2:659-60. [PMID 698650]
- Navarro S, Ros E, Aused R, Garcia Puges M, Pique JM, Vilar Bonet J. Comparison of fasting, nasogastric suction and cimetidine in the treatment of acute pancreatitis. Digestion 1984; 30:224-30. [PMID 6391981]
- Sarr MG, Sanfey H, Cameron JL. Prospective, randomized trial of nasogastric suction in patients with acute pancreatitis. Surgery 1986; 100:500-4. [PMID 3526610]
- Maisto OE, Bremner CG. Antacids in the treatment of acute alcohol-induced pancreatitis. S Afr Med J 1983; 63:351-2. [PMID 6828933]
- Moreno-Otero R, Rodriguez S, Carbo J, Garcia- Buey L, Pajares JM. Double-blind trial of pirenzepine in acute pancreatitis. Digestion 1989; 42:51-6. [PMID 2472988]
- Oruc N, Ozutemiz AO, Nart VY, Celik HA, Yuce G, Batur Y. Infliximab: a new therapeutic agent in acute pancreatitis? Pancreas 2004; 28:E1-8. [PMID 14707742]
- Lawinski M, Sledzinski Z, Kubasik-Juraniec J, Spodnik JH, Wozniak M, Boguslawski W. Does resveratrol prevent free radical-induced acute pancreatitis? Pancreas 2005; 31:43-7. [PMID 15968246]
- Pastor CM, Frossard JL. Are genetically modified mice useful for the understanding of acute pancreatitis? FASEB J 2001; 15:893-7. [PMID 11292648]
- Zou WG, Wang DS, Lang MF, Jin DY, Xu DH, Zheng ZC, et al. Human interleukin 10 gene therapy decreases the severity and mortality of lethal pancreatitis in rats. J Surg Res 2002; 103:121-6. [PMID 11855927]
- Villoria A, Abadía de Barbará C, Molero X, Álvarez A, Antolín M, Guarner L, Malagelada JR. Early treatment with interleukin-10 (IL-10) in severe acute pancreatitis. Pancreatology 2003; 3:466.
- Foitzik T, Eibl G, Schneider P, Wenger FA, Jacobi CA, Buhr HJ. Omega-3 fatty acid supplementation increases anti-inflammatory cytokines and attenuates systemic disease sequelae in experimental pancreatitis. JPEN J Parenter Enteral Nutr 2002; 26:351-6. [PMID 12405646]
- Lasztity N, Hamvas J, Biro L, Nemeth E, Marosvolgyi T, Decsi T, et al. Effect of enterally administered n-3 polyunsaturated fatty acids in acute pancreatitis: a prospective randomized clinical trial. Clin Nutr 2005; 24:198-205. [PMID 15784478]
- Mason J, Siriwardena AK. Designing future clinical trials in acute pancreatitis. Pancreatology 2005; 5:113-5. [PMID 15849481]
- Johnson CD, Kingsnorth AN, Imrie CW, McMahon MJ, Neoptolemos JP, McKay C, et al. Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis. Gut 2001; 48:62-9. [PMID 11115824]
- Abu-Zidan FM, Windsor JA. Lexipafant and acute pancreatitis: a critical appraisal of the clinical trials. Eur J Surg 2002; 168:215-9. [PMID 12440758]
- Pezzilli R, Ceciliato R, Barakat B, Corinaldesi R. Immune-manipulation of the inflammatory response in acute pancreatitis. What can be expected? JOP. J Pancreas (Online) 2004; 5:115-21. [PMID 15138332]
- Seta T, Noguchi Y, Shimada T, Shikata S, Fukui T. Treatment of acute pancreatitis with protease inhibitors: a meta-analysis. Eur J Gastroenterol Hepatol 2004; 16:1287-93. [PMID 15618834]
- Windsor AC, Kanwar S, Li AG, Barnes E, Guthrie JA, Spark JI, et al. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998; 42:431-5. [PMID 9577354]
- Eatock FC, Chong P, Menezes N, Murray L, McKay CJ, Carter CR, Imrie CW. A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis. Am J Gastroenterol 2005; 100:432-9. [PMID 15667504]
- Olah A, Belagyi T, Issekutz A, Gamal ME, Bengmark S. Randomized clinical trial of specific lactobacillus and fibre supplement to early enteral nutrition in patients with acute pancreatitis. Br J Surg 2002; 89:1103-7. [PMID 12190674]
- Besselink MG, Timmerman HM, Buskens E, Nieuwenhuijs VB, Akkermans LM, Gooszen HG. Dutch Acute Pancreatitis Study Group. Probiotic prophylaxis in patients with predicted severe acute pancreatitis (PROPATRIA): design and rationale of a double-blind, placebo-controlled randomised multicenter trial [ISRCTN38327949]. BMC Surg 2004; 4:12. [PMID 15456517]
- Sharma VK, Howden CW. Prophylactic antibiotic administration reduces sepsis and mortality in acute necrotizing pancreatitis: a meta-analysis. Pancreas 2001; 22:28-31. [PMID 11138967]
- Isenmann R, Runzi M, Kron M, Kahl S, Kraus D, Jung N, et al. Prophylactic antibiotic treatment in patients with predicted severe acute pancreatitis: a placebo- controlled, double-blind trial. German Antibiotics in Severe Acute Pancreatitis Study Group. Gastroenterology 2004; 126:997-1004. [PMID 15057739]
- Bassi C, Falconi M. Discussion on prophylactic antibiotic treatment in patients with predicted severe pancreatitis: a placebo-controlled, double-blind trial. Gastroenterology 2004; 127:1015-6. [PMID 15362072]
- Pezzilli R. Antibiotic prophylaxis in acute necrotizing pancreatitis: yes or no? JOP. J Pancreas (Online) 2004; 5:161-4. [PMID 15138342]
- Levy P, Heresbach D, Pariente EA, Boruchowicz A, Delcenserie R, Millat B, et al. Frequency and risk factors of recurrent pain during refeeding in patients with acute pancreatitis: a multivariate multicentre prospective study of 116 patients. Gut 1997; 40:262-6. [PMID 9071942]
- Levy P, Hastier P, Arotcarena R, Bartolie E, Bougeard-Julien M, Blumberg J, et al. Efficacy of lanreotide 30 mg on prevention of pain relapse after oral refeeding in patients with necrotizing acute pancreatitis. A phase II prospective multicentre study. Pancreatology 2004; 4:229-32. [PMID 15148442]
- Ibars EP, Sanchez de Rojas EA, Quereda LA, Ramis RF, Sanjuan VM, Peris RT. Pancreatic function after acute biliary pancreatitis: does it change? World J Surg 2002; 26:479-86. [PMID 11910484]
- Pareja E, Artigues E, Aparisi L, Fabra R, Martinez V, Trullenque R. Exocrine pancreatic changes following acute attack of biliary pancreatitis. Pancreatology 2002; 2:478-83. [PMID 12378116]
- Sabater L, Pareja E, Aparisi L, Calvete J, Camps B, Sastre J, et al. Pancreatic function after severe acute biliary pancreatitis: the role of necrosectomy. Pancreas 2004; 28:65-8. [PMID 14707732]
- Migliori M, Pezzilli R, Tomassetti P, Gullo L. Exocrine pancreatic function after alcoholic or biliary acute pancreatitis. Pancreas 2004; 28:359-63. [PMID 15097850]

